
Abstract
Background
The measurement of monoclonal free light chains is being increasingly utilized since the introduction of serum-based assays. It is important for laboratories to determine their own reference ranges in order to reflect the local population. The aim of this study was to determine if age-adjusted reference ranges for serum free light chains would have implications for demand management of further laboratory investigations including immunofixation.
Methods
After certain exclusions, 4293 samples from individuals seen in primary care across Oxfordshire between 2014 and 2016 were identified for analysis of patient characteristics, serum free light chain results and estimated glomerular filtration rate.
Results
We found age to be an independent variable when considering serum free light chain concentrations, ratio and estimated glomerular filtration rate. The reference ranges derived from our data differ markedly from the original Binding Site ranges. When the age-specific ranges are retrospectively applied to our population, there is a 38% decrease in follow-up testing with no loss of specificity.
Conclusion
We feel confident implementing new age-specific serum free light chain reference ranges in our laboratory. We have developed a simple algorithm for evaluating serum free light chains based on age and estimated glomerular filtration rate. We encourage laboratories to establish their own local reference ranges using large cohorts and their chosen serum free light chain assay platform.
Keywords
Background
The detection of monoclonal free light chains has historically been performed by urine electrophoresis, conducted alongside the serum investigations. Obtaining urine samples for immunological investigations from patients is challenging; studies from both primary and secondary care have shown that, at best, only 40% of patients have urine electrophoresis performed, and in some studies, this is as low as 5%.1,2
Serum free light chain (FLC) assays allow the identification and quantification of kappa and lambda immunoglobulin FLCs and indirect determination of monoclonality using the kappa:lambda ratio (FLCr). 3 Novel disease classifications have arisen using these methods including light chain MGUS, defined by the absence of paraprotein by serum protein electrophoresis (SPEP) and serum immunofixation (IFE) and the presence of abnormal FLCr and raised FLC concentrations. 4
In 2016, the NICE guidelines for myeloma diagnosis and management recommended the introduction of FLC measurement (alongside SPEP) into the myeloma diagnostic algorithm, ‘to confirm the presence of a paraprotein indicating possible myeloma or monoclonal gammopathy of undetermined significance (MGUS)’. 5 These guidelines also recommend performing IFE on all samples with abnormal FLCr. Both recommendations highlight the importance of having accurate reference ranges which reflect the population being tested. The 2009 International Myeloma Working Group (IMWG) guidelines recommend treating myeloma patients with LC ratio of >100 in the absence of other CRAB features (hypercalcaemia, renal failure, anaemia and bone lesions) due to increased risk of progression to active myeloma. 6
Accordingly, FLC measurements are now the standard of care for patients with plasma cell dyscrasias. In primary care, the FLC assay can aid decision-making regarding further laboratory investigations, including IFE, and onward referral to secondary care. In secondary care, FLC measurement can aid the diagnosis, prognostication and on-going management of patients with plasma cell dyscrasias.
The Freelite (The Binding Site, UK) assay is a turbidimetric assay which uses polyclonal antibodies directed at epitopes of the FLC constant region which are hidden in intact immunoglobulins; therefore, only light chains which are unbound to a heavy chain are quantified. The reference range supplied by The Binding Site (Birmingham, UK) for FLCr is 0.26–1.65 (kappa concentration: 3.30–19.40 mg/L, lambda concentration: 5.71–26.30 mg/L using the 95th percentile). These data were obtained from a limited number of samples (282 normal subjects aged 20 to 90 years) and was intended for guidance purpose only. 7 The FLCr range supplied by The Binding Site is used in the IMWG diagnostic criteria for light-chain MGUS and therefore has an impact on both the diagnosis and monitoring of this disorder. 8
The aim of this study was to generate age-adjusted reference ranges for FLC and FLCr. As serum FLC concentrations are known to be affected by GFR, we also took the estimated glomerular filtration rate (eGFR) values of our cohort under consideration. By retrospectively applying the novel reference ranges to the overall cohort, we demonstrate our approach has significant implications for demand management, both in respect to further laboratory testing and referrals for secondary care.
Methods
A service evaluation of laboratory diagnostics at the Immunology Laboratory, Oxford, was undertaken to evaluate the clinical utility and cost-effectiveness of screening for plasma cell dyscrasias in 4544 consecutive serum samples sent for serum protein electrophoresis from individuals seen in primary care across Oxfordshire, UK in 2014–2016.
Patients enrolled in this study were >20 years of age with no known history of lymphoproliferative disease, confirmed by the Laboratory Information Management System (LIMS). All samples underwent nephelometric immunoglobulin measurement (Architect C4000, Abbott) and SPEP (V8, Helena) within three days of receipt in the laboratory. Measurement of FLC concentrations using the SPAPlus analyser (The Binding Site, UK) and Binding Site reagents was performed within 21 days of receipt in the laboratory. This data-set was used to validate the Freelite reference range provided by the Binding Site and to generate age-specific reference ranges for FLC and FLCr.
The following exclusions were made: 26 samples (0.6%) were excluded because clinical details provided on the request card included chronic kidney disease (CKD); 204 (4.5%) patients were excluded because a monoclonal protein was identified on SPEP; all patients with an FLCr outside of the established Binding Site reference range underwent immunofixation (Hydrasys, Sebia) which identified a monoclonal protein in a further 21 (0.5%) patients who were also excluded.
Results from the remaining 4293 samples were taken forward for further analysis. Samples were stratified by age into four groups: 20–40 (445 patients), 41–60 (1151 patients), 61–80 (1972 patients), 81+ (725 patients). Each age group was subject to normality plotting of kappa and lambda light chain concentrations and FLCr (Analyse-it for Microsoft Excel, Version 2.20, Analyse-it Software, Ltd) to dismiss samples that could represent patients with significant disease. The normally distributed region of each group was then selected, and a 2.5th–97.5th percentile analysis was carried out to define reference ranges for serum free kappa and lambda concentrations and FLCr.
Figure 1 shows an example of the normal Q-Q plot for kappa light chain concentrations in the 20–40 age group. As renal impairment can significantly affect the FLC concentrations, eGFR values were calculated based on serum creatinine assayed within three months of the FLC samples, utilizing the ‘Modification of Diet in Renal Disease (MDRD)’-formula. 9
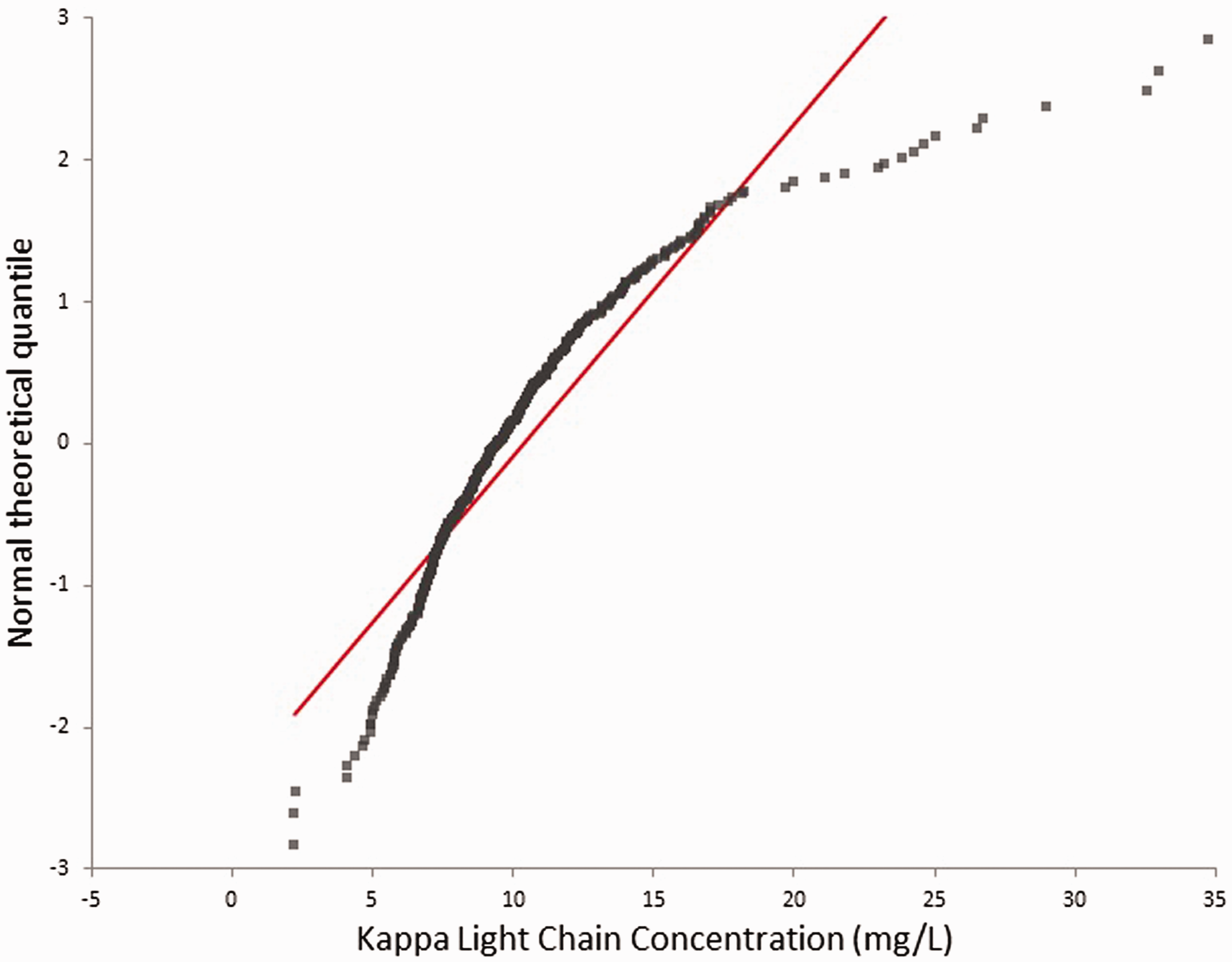
Free kappa light chain Normal Q-Q plot for age range 20–40 years. This normality plotting was performed for free kappa concentrations, free lambda concentrations and FLCr for the different age range categories.
One-way ANOVA analysis was carried out for the four variables (kappa concentration, lambda concentration, FLCr and eGFR) between the four age groups. A P-value of <0.05 was considered significant.
Results
The median age within the cohort was 67 years (range 20–102), with 59% of the samples originating from females. When modelling the data, both age vs. FLCr (r = 0.29, P < 0.001, 95% CI [0.27, 0.32]) and eGFR vs. FLCr (r = −0.24, P < 0.001, 95% CI [−0.27, −0.22]) relationships were found to be linear.
Table 1 shows the range of free kappa concentration, free lambda concentration, FLCr and eGFR generated from the entire cohort with 2.5th–97.5th percentile analysis performed prior to normality plotting.
Free light chain concentration and ratio by age range for the entire cohort prior to normality plotting.
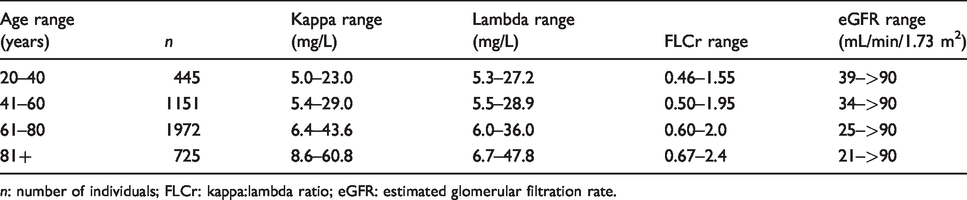
n: number of individuals; FLCr: kappa:lambda ratio; eGFR: estimated glomerular filtration rate.
Table 2 shows the range of free kappa concentration, free lambda concentration, FLCr and eGFR generated from the normally distributed cohort, following normality plotting with the 2.5th–97.5th percentile analysis performed. The data presented in Table 2 represent the reference ranges we consider to be useful and have adopted in clinical practice.
Free light chain concentrations, free light chain ratio and eGFR by age range for the normally distributed 2.5th–97.5th percentile cohort.
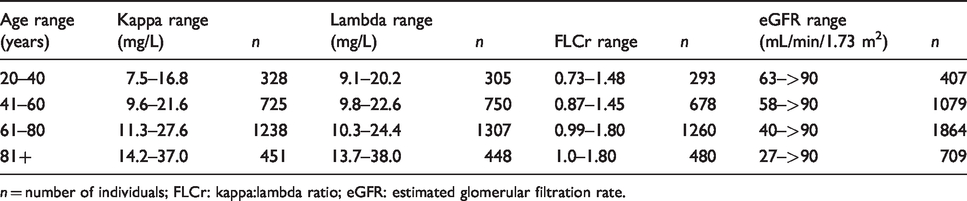
n = number of individuals; FLCr: kappa:lambda ratio; eGFR: estimated glomerular filtration rate.
Using the normally distributed data in Table 2, one-way ANOVA analysis of the different age groups reveals significant differences between each age group (P < 0.001) for all variables (kappa concentration, lambda concentration, FLCr and eGFR). No statistically significant relationship was observed between gender and any of the variables.
Figure 2 shows the prevalence data for eGFR ranges within each age group after normality plotting and 2.5th–97.5th percentile analysis. A normal eGFR is considered to be ≥60 mL/min/1.73 m2. The prevalence of eGFRs within CKD classifications 3–4 (which are classified by progressively worsening renal impairment starting as eGFR <60 mL/min/1.73 m2) increased with age; however, no patients in the cohort had an eGFR within the CKD 5 range (<15 mL/min/1.73 m2). This is likely to reflect the fact that these patients are principally managed in secondary, not primary care. None of the patients with eGFR <60 mL/min/1.73 m2 can be classified as having CKD without other markers of kidney disease being present. The eGFR prevalence by age results from our analysis are concordant with those found by a large retrospective study calculating eGFR in primary care patients from Oxfordshire. 10
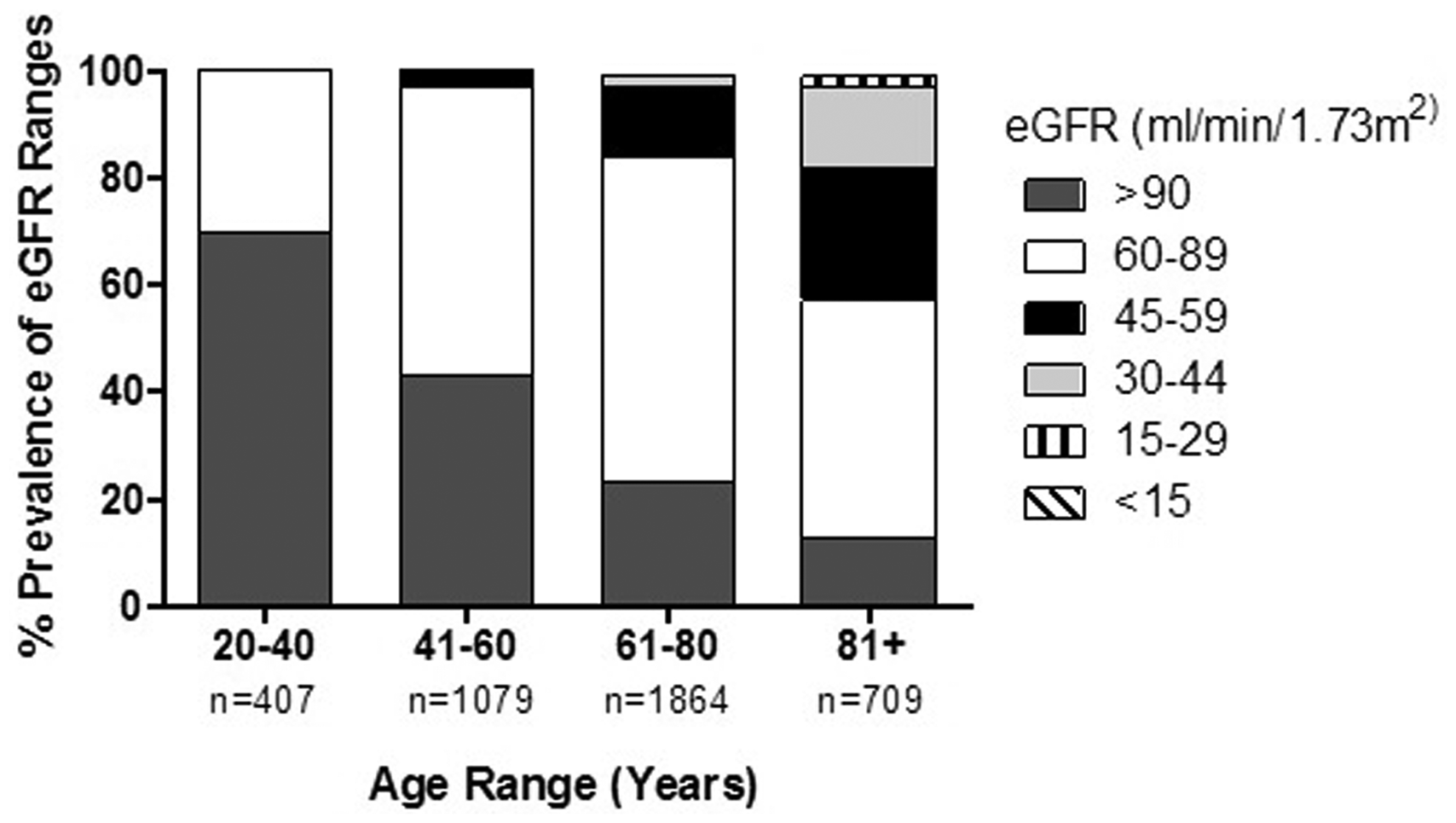
Prevalence of eGFR for each age group.
The 2016 NICE guidelines recommend performing serum IFE on any patients with an abnormal SPEP or FLCr. 5 We retrospectively applied the new normally distributed FLCr and eGFR ranges to the data. Based on the Binding Site FLCr ranges, 410 patients underwent serum IFE. Using our new reference ranges, 254 patients would have undergone serum IFE, representing a 38% reduction. The new reference ranges would have failed to identify four patients with small paraproteins only identified by serum IFE. Two-year follow-up of these patients shows no evidence of a persistent monoclonal gammopathy, suggesting that these paraproteins were transient, reactive phenomena.
Conclusion
The establishment of reference ranges is essential to allow the meaningful interpretation of laboratory investigations. We measured FLC in over 4000 primary care patients sent for immunoglobulin testing using the Binding Site Freelite platform. We demonstrate significantly different reference ranges for serum free kappa concentration, serum-free lambda concentration and the kappa/lambda ratio based on an individual’s age. This contrasts with previous smaller studies that found age was not an independent variable when considering serum FLC concentrations.3,11 Both of these studies enrolled less than 150 patients and were likely underpowered to identify such differences.
In our population, renal impairment consistent with CKD stages 3–5 increased with age, as previously show. 12 The eGFR age-specific ranges produced by our data concur with age-specific values produced from over 3500 non-diseased Caucasian participants in the Netherlands. 12 As accurate classification of CKD stages 3–5 requires decreased eGFR values over a minimum period of three months, we are unable to determine the true prevalence of CKD within the study population. Nevertheless, we did determine a weak inverse association between renal function as assessed by eGFR and serum FLC ratio. This is in concordance with previous work assessing FLC in patients with CKD but without monoclonal gammopathy. 9 It was found that these patients had higher FLCr when compared with the original healthy volunteer range. From this work on patients in renal failure, a new ‘reference’ FLCr range (0.37–3.1) was proposed for patients with renal impairment, regardless of age, and is currently in use in our laboratory.9,13
The National Kidney Foundation (NKF) recommends a cut-off of 60 mL/min/1.73 m2 or below to categorize a patient as having CKD. 14 However, the CKD classification guidelines produced by the NKF make no distinction based on either age or gender. The MDRD equation used to calculate eGFR was developed using nephrology referral patients with elevated serum creatinine concentrations 15 ; however, it has been found to have a more limited use for the general population, underestimating GFR in healthy subjects. 16
It has been shown a number of times that GFR declines with normal aging,12,17 with a decline of approximately 5–10 mL/min per decade; this compares well with our data. The study in the Netherlands showed that defining a cut-off for CKD without taking age into account can lead to misclassification, with a significant minority of mostly older healthy subjects, having an eGFR below 60 mL/min/1.73 m2. 12 Many of the patients in our cohort who are >60 years of age would meet the NKF criteria for moderate CKD, and our data show that an eGFR of 60 mL/min/1.73 m2 is within the reference range for patients aged 41 years and over.
It has previously been established that eGFR values <60 mL/min/1.73 m2 are associated with a worse prognosis, and that in the general population, overall mortality risk is significantly increased below this cut-off.14,18 A large cohort study, however found that, although present, this association between eGFR of <60 mL/min/1.73 m2 and mortality was far weaker in elderly subjects than in the younger age groups. 19 This study found that an eGFR of 50–59 mL/min/1.73 m2 was associated with increased mortality in subjects aged 18–54 years. This compares well with our lower limit of the eGFR reference range for <60 year olds being 58 mL/min/1.73 m2. From the extensive data, this study suggested that mortality risk stratification should not be based on the same eGFR cut-off points for all ages, and proposed an eGFR cut-off between 30 and 59 mL/min/1.73 m2 for elderly patients. This also compares well with our data for both the 61–80 years and 81+ year age groups and the data produced in the Netherlands study. 12
Within our primary care population, we hypothesize that a decline in renal function and an increase in subclinical non-renal illnesses with age will contribute to the increased FLC ranges seen in this study, and this will not lead to false normal results. To ensure this, we performed a two-year follow-up on all patients through laboratory records and found no patients with FLCr within the new reference ranges had developed a plasma cell dyscrasia.
As we have used a primary care population, rather than a healthy control population to calculate these ranges, it is possible that patients with non-renal illnesses can have raised FLC concentrations. However, these raised concentrations have so far been seen to either not affect FLCr or result in only a borderline increased FLCr.20–22
Our ranges varied from those stated in the Binding Site kit insert and have time and cost implications for the laboratory, as shown by the reduction of serum IFEs needing to be performed. For our data-set, this reduction is exclusively due to the adjustment of the FLCr ranges for our different age groups. Notably, FLC assays have been shown to be platform dependent, 23 and so these ranges can only apply to samples being tested on the SPAPlus analyser using the Binding Site reagents. We generated these data using a primary care population as a substitute for a large healthy control population. We believe that these ranges can also be applied to patients in secondary care being screened for monoclonal gammopathies, with renal impairment being taken into account. A study in tertiary care samples found a high false-positive FLCr rate in those without a monoclonal gammopathy when using the original Binding Site FLC reference ranges. 24 This supports the data we have found in our primary care population and suggests that our alternative ranges can be applied across the different care cohorts. We encourage laboratories to establish their own local reference ranges using large cohorts and their chosen FLC platform.
With our follow-up indicating no missed plasma cell dyscrasia patients, we can be confident in implementing these ranges into our routine practice with the aim to reduce the number of unnecessary follow-up tests and referrals for patients being screened with SPEP and FLC in line with the 2016 NICE guidelines. 5 From both our data analysis and previous data, we feel that age-specific eGFR values should be used when screening patients for monoclonal gammopathy. We feel confident in setting new eGFR cut-off limits, below which to use the previously calculated FLCr renal reference range.9,13 These cut-offs remain at <60 mL/min/1.73 m2 for patients aged 60 years and below, but decrease to <40 mL/min/1.73 m2 for patients aged 61 years and over.
Accordingly, we have developed an algorithm for interpreting FLC results and determining whether further investigation with IFE is warranted in the presence of a normal SPEP. If a patient has significant renal dysfunction as defined by the eGFR cut-off for their age (<60 mL/min/1.73 m2 for patients aged 60 years and below, <40 mL/min/1.73 m2 for patients aged 61 years and over), then the previously generated renal FLCr reference range (0.37–3.1) will be used for interpretation.
If eGFR is >60 mL/min/1.73 m2 for patients aged 60 years and below, or >40 mL/min/1.73 m2 for patients aged 61 years and over, then the age adjusted ranges calculated from patients where significant renal dysfunction had been excluded will be used (Table 2). This should reduce patients inappropriately being labelled as light-chain MGUS, reduce the need for long-term follow-up and monitoring and reduce the burden of further laboratory investigation of ostensibly normal results.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded internally as part of a service evaluation approved by the Oxford University Hospitals NHS Foundation Trust R&D Department.
Ethical approval
Not applicable.
Guarantor
LC.
Contributorship
RS, KR, LC and BF conceived the study. LC and DS analysed samples and compiled data. RS, AS and LC analysed data and drafted the paper. All authors reviewed and edited the article and approved the final version of the article.