
Abstract
Background
The aspartate aminotransferase (AST)/alanine aminotransferase (ALT) ratio (AST/ALT) is an independent predictor of hepatic disease.
Objectives
To evaluate the association between preoperative AST/ALT and postoperative acute kidney injury in hepatocellular carcinoma patients.
Methods
A total of 422 hepatitis B- or C- virus-associated hepatocellular carcinoma patients, who underwent hepatectomy between September 2012 and April 2018, were enrolled this retrospective study. From all patients, aspartate aminotransferase and alanine aminotransferase parameters were collected, and the AST/ALT ratio was calculated. For diagnostic criteria of postoperative acute kidney injury, the Kidney Disease Improving Global Outcomes (KDIGO) criteria guidelines were used.
Results
In 48 patients (11.4%), postoperative acute kidney injury was confirmed. In patients with postoperative acute kidney injury, the mean preoperative serum AST/ALT was significantly higher when compared with patients without postoperative acute kidney injury. After multivariate logistic regression analysis, AST/ALT, haemoglobin, age, hypertension, Child-Turcotte-Pugh classification and the Milan criteria were all confirmed as predictive factors of postsurgical acute kidney injury. We found that an AST/ALT of 1.29 was the best cut-off point for predicting postoperative acute kidney injury. The positive predictive value (23.9%) of the cut-off is actually poor. After matching the propensity score, AST/ALT ≥1.29 was still confirmed as an independent predictor of postoperative acute kidney injury by multivariate analysis.
Conclusion
Preoperative elevated serum AST/ALT may be a potential independent predictor of postoperative acute kidney injury in hepatocellular carcinoma patients who have undergone hepatectomy. This needs to be tested in further prospective studies.
Keywords
Introduction
Acute kidney injury (AKI) is an increasingly common clinical challenge, and a major complication following abdominal surgery.1,2 Previous studies have reported that AKI occurred in approximately 15% of hepatectomy cases. 1 AKI is closely correlated to increased mortality, length of hospital stay, increased medical expenses and lower rates of long-term survival.3–7 Several studies have indicated that AKI is also associated with a 10-fold increase in hospital mortality, a decreased survival for up to 15 years after surgery and an increased risk of developing chronic kidney disease (CKD).4,6,8,9 The scale and AKI’s burden are particularly distinct in developing countries, including China, which has the most patients with hepatitis B in the world. 2 Given that infection with the hepatitis B virus is closely correlated with the occurrence and development of hepatocellular carcinoma (HCC), 10 it is of utmost importance to establish novel approaches to preoperatively identify patients with HCC who are at high risk for postoperative AKI in order to customize treatment.
Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are circulating enzymes that are predominantly synthesized by the liver. Some studies indicate that high concentrations of AST and ALT serve as indicators of HBV infection,11,12 which in turn is connected to nephropathy.13 Additionally, both AST and ALT have served as inflammatory biomarkers. 14 In cirrhotic patients, an increased AST/ALT significantly correlated with the progression of liver dysfunction, the cirrhosis stage and offered prognostic information similar to established scoring systems, such as the Model for End-stage Liver Disease or Child-Pugh score. 15 Moreover, it has been shown that AST/ALT is a predictive factor of liver fibrosis as well as cirrhosis in patients with chronic HCV infection. 16 Inflammation-associated components, such as serum AST and ALT, are also related with oxidative stress and systemic inflammation. Oxidative stress in turn, is related to AKI.
Studies that focus on the association between preoperative serum AST/ALT and the incidence of postoperative AKI in patients with HCC are limited. Therefore, the predictive value of preoperative AST/ALT in patients with postsurgical AKI remains to be elucidated. In the study, we performed a large-scale retrospective cohort analysis to investigate the association between AST/ALT and postoperative AKI in HCC patients who have undergone hepatectomy.
Materials and methods
Patients
A total of 647 patients, who were clinically diagnosed with HCC by liver magnetic resonance imaging (MRI) and/or dynamic computed tomography (CT) at the Wuhan Union Hospital between September 2012 and April 2018, were enrolled in this retrospective study. The American Association for the Study of Liver Diseases criteria was used for the diagnostic evaluation of HCC. 17 Prior to diagnosis, none of the participants received treatment for HCC.
Exclusion criteria were as follows: (1) no history of hepatitis virus infection; (2) tumour rupture; (3) no Barcelona Clinic Liver Cancer (BCLC) 0- or A-staged HCC and (4) no hepatectomy (Figure 1). In addition, patients who already participated in a previous study regarding AST/ALT ratio diagnostics were not enrolled in this study. Finally, a total of 422 patients were enrolled in the current retrospective study. HCC was histologically confirmed in all participants. Clinical parameters of all patients were collected from the respective patients’ records. Prior to analysis, the patient's information was anonymized and de-identified. Prior to surgery, the risks and benefits of the surgery were explained to all patients. All patients signed an informed consent before surgery. This retrospective study was approved by the Tongji Medical College research ethics committee, Wuhan, China.
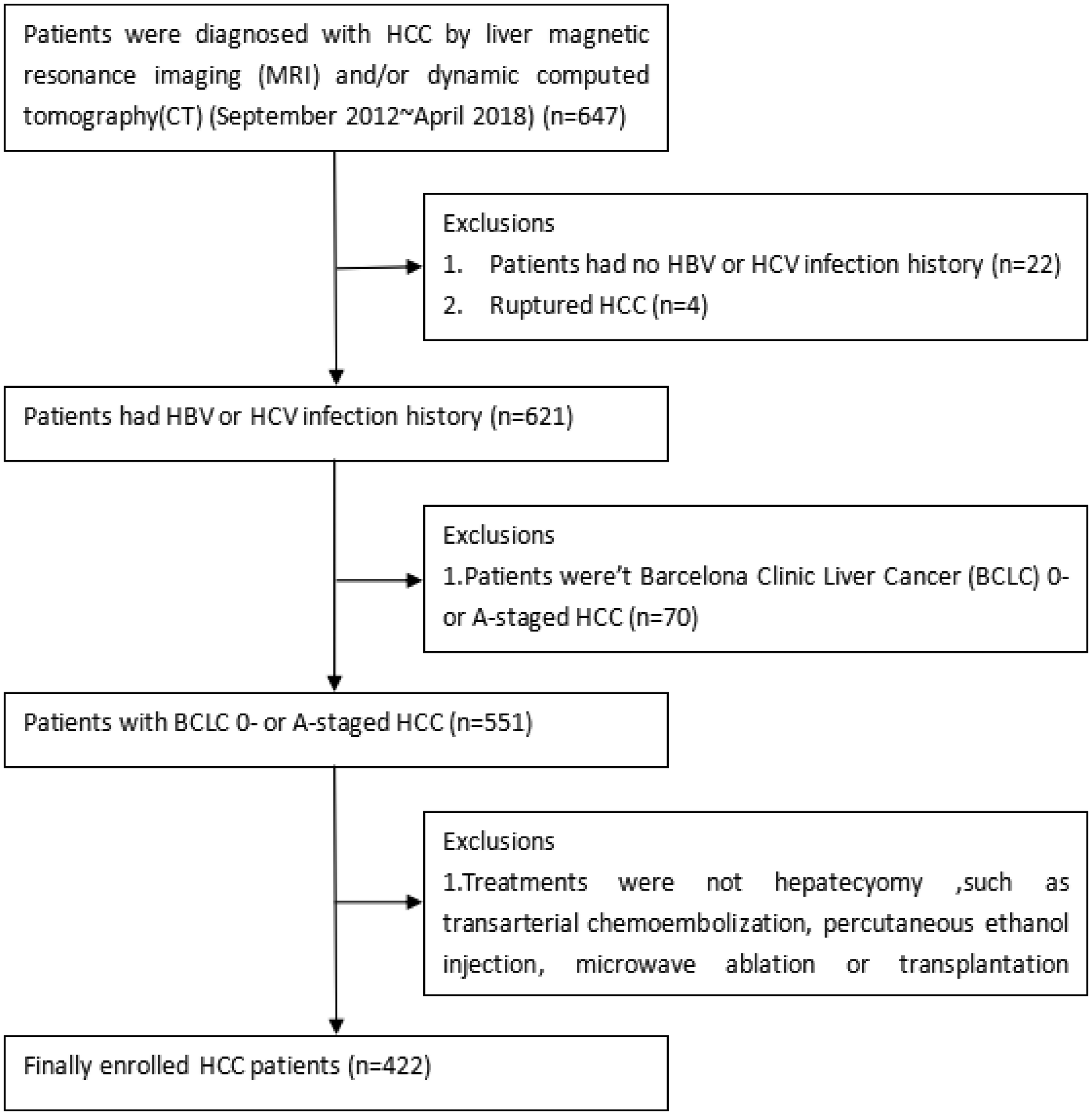
A total of 422 HCC patients were enrolled in this study.
Preoperative assessment of patients
Laboratory assessment
Prior to surgery, the following clinical data were collected and recorded: sex, age, diabetes, hypertension, aetiology of HCC, haemoglobin (Hb), platelet (PLT), serum AST, ALT, γ-glutamyl transferase (GGT), albumin, total bilirubin (TB), creatinine (Cr), prothrombin time-international normalized ratio (INR), α-fetoprotein (AFP), HBV DNA concentrations, Child-Turcotte-Pugh (CTP) classification and the Cancer of the Liver Italian Group Score (CLIP). The AST/ALT of all patients was calculated and was based on preoperative serum biochemical examination results.
An automatic biochemical analyser, AU5800 (Beckman Coulter, USA), was used to measure the concentrations of AST, ALT, GGT, albumin, TB and Cr. Nicotinamide adenine dinucleotide (NADH) methods were used to detect AST and ALT with the biochemical analyser. Liquid Assayed Multiqual was used in QC procedures. An automated blood analyser, XE-2100 (Sysmex, Japan), was used to measure the concentrations of white blood cells (WBCs), Hb and PLT. The coagulometer from Compact (STAGO, France) was used to test the concentrations of PT and INR. Chemiluminescence immunoanalysis with model I2000 (Architect, USA) was used to measure the concentration of AFP. Fluorescence quantitative PCR was used to measure the concentration of HBV DNA.
Image assessment
Prior to surgery, enhanced CT and/or MRI were performed to evaluate the number of tumours, tumour size and vascular invasion. None of the HCC patients showed signs of extrahepatic metastases. The carcinoma size was defined based on the longest diameter of the largest tumour seen in the image. Small HCC was defined based on the Milan criteria (solitary tumour ≤5 cm or up to three nodules ≤3 cm). 10 Thereafter, the stage of HCC was determined by the BCLC staging system. 18
Surgical treatment
All patients underwent hepatectomy within two weeks after their CT or MRI scan. Hepatectomy was considered minor when <3 liver segments were resected and major when ≥3 segments were resected. Surgical specimens were routinely sent for pathological examination. The differentiation of HCC was defined by the Edmondson grading system. 19
Postoperative assessment and management of patients
Patients who showed unstable vital signs after surgery received postoperative treatment and care in an intensive care unit. Patients whose vital signs were in the reference range were taken to general wards. Blood samples were collected from each patient on days 1, 4 and 7 postsurgery and were tested for the concentrations of Hb, WBC, PLT, AST, ALT, GGT, albumin, TB, Cr, INR and AFP. Most patients, who did not present complications, were discharged approximately two weeks after surgery. Patients reported back to the clinic for follow-up assessments about one month after being discharged.
Definition of postoperative AKI
The KDIGO criteria describe that a Cr increase of ≥0.3 mg/dL (26.5 mmol/L) above baseline within 48 h after surgery or an increase of ≥1.5-fold above baseline within seven days after surgery, was used to define postoperative AKI. 2 However, AKI patients who presented with organ failure, such as liver failure, circulatory failure, respiratory failure, or septic shock, were not enrolled in this study.
Propensity score matching
Participants were divided into two groups according to the best cut-off point of AST/ALT, including a high AST/ALT (≥1.29) group and a low AST/ALT (<1.29) group. The propensity score matching was introduced by Rosenbaum and Rubin over 30 years ago and was used to match participants. 20 The process of matching participants was performed by using Empower Stats software. The propensity score of a patient was calculated using a logistic regression model, in which age, gender, aetiology, hypertension, diabetes, cirrhosis, CTP, CLIP score, GGT, INR, albumin, TB, Cr, AFP, Hb, tumour size, BCLC stage, tumour number, differentiation and type of surgery were all considered. To minimize conditional bias, we adopted the nearest matching neighbour. Each patient in the high AST/ALT group was matched to a patient in the low AST/ALT group who showed the closest propensity score. Subsequently, both patients were eliminated from the next propensity score matching. However, for several patients in the high AST/ALT group, a matching control was not found in the low AST/ALT group. The inclusion criteria for variables included a propensity score difference less than 0.05.
Statistical analyses
Continuous and categorical variables were presented as the mean (range) and frequency, respectively. A Student’s t-test was performed to compare continuous variables when the population variance of the two groups was the same. Separate variance estimation t-tests were performed to compare continuous variables when the population variance of the two groups varied. The χ2 test or Fisher’s exact test was used to compare categorical variables. The logistic regression model was used in univariate and multivariate analyses to evaluate independent predictors of postoperative AKI. Variables in univariate analyses with a value of P < 0.05 were subjected to multivariate logistic regression analyses. The odds ratio (OR) and 95% confidence interval (CI) were obtained. Sensitivity of the AUCs for prediction of postoperative AKI based on KDIGO criteria was calculated using the DeLong’s method. The best cut-off point of AST/ALT and Hb was obtained using the Youden index. P < 0.05 was considered statistically significant, based on two-tailed tests. Statistical analyses were performed by SPSS software version 24.0 (SPSS, Chicago, IL, USA).
Results
Patient characteristics
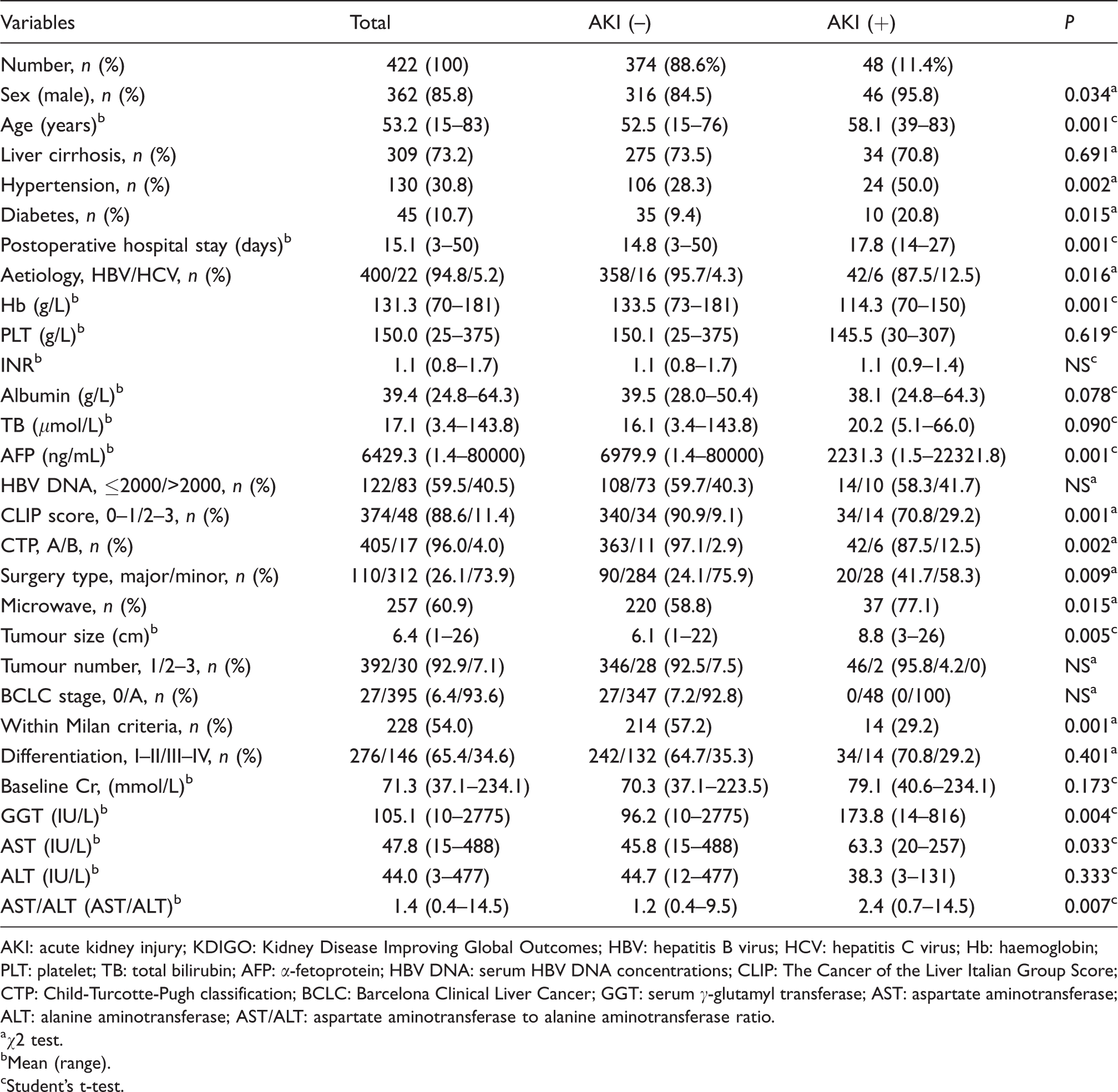
A total of 422 HCC patients with HBV or HCV infection were included in this retrospective study (Figure 1). The characteristics of patients are presented in Table 1. Among the patients, there were 362 (85.8%) males, and the mean age was 53.2 years (15–83 years). A total of 309 (73.2%) patients were diagnosed with cirrhosis, 45 (10.7%) participants had diabetes mellitus and 130 (30.8%) patients had a history of hypertension. After surgery, the mean length of hospital stay was 15.1 days (3–50 days). HBV infection was confirmed in 400 (94.8%) patients and demonstrated the most common HCC aetiology. The mean concentrations of Hb, PLT, INR, albumin, TB and AFP concentrations were 131.3 (70–181) g/L, 150.0 (25–375) g/L, 1.1 (0.8–1.7), 39.4 (24.8–64.3) g/L, 17.1 (3.4–143.8) μmol/L and 6429.3 (1.4–80,000) ng/mL, respectively. A total of 374 (88.6%) patients were considered as having a low CLIP score 0–1 and 405 (96.0%) patients had CTP class A liver function. Three hundred and twelve (73.9%) patients underwent minor resection, 110 (26.1%) patients underwent major resection and 257 (60.9%) patients underwent microwave ablation at the resection margin. A total of 392 (92.9%) HCC patients had one lesion, and the mean tumour size was 6.4 cm (1 cm–26 cm). Three hundred and ninety-five (93.6%) patients were considered BCLC stage A HCC, 27 (6.4%) patients were considered BCLC stage 0 and 228 (54.0%) patients suffered from HCC as defined by the Milan criteria. HCC differentiation I–II and III–IV were confirmed in 276 (65.4%) and 146 (34.6%) patients, respectively. The mean concentrations of Cr, GGT, AST, ALT and AST/ALT were 71.3 (37.1–234.1) mmol/L, 105.1 (10–2775) IU/L, 47.8 (15–488) IU/L, 44.0 (3–477) IU/L and 1.4 (0.4–14.5), respectively.
Distribution of patients according to AKI based on the ‘KDIGO’ criteria.
AKI: acute kidney injury; KDIGO: Kidney Disease Improving Global Outcomes; HBV: hepatitis B virus; HCV: hepatitis C virus; Hb: haemoglobin; PLT: platelet; TB: total bilirubin; AFP: α-fetoprotein; HBV DNA: serum HBV DNA concentrations; CLIP: The Cancer of the Liver Italian Group Score; CTP: Child-Turcotte-Pugh classification; BCLC: Barcelona Clinical Liver Cancer; GGT: serum γ-glutamyl transferase; AST: aspartate aminotransferase; ALT: alanine aminotransferase; AST/ALT: aspartate aminotransferase to alanine aminotransferase ratio.
aχ2 test.
bMean (range).
cStudent’s t-test.
Comparison of clinical parameters according to AKI
Postsurgical AKI was confirmed in 48 (11.4%) patients (Table 1). Table 1 shows that patients without postoperative AKI were roughly 5.6 years younger compared with patients with AKI (52.5 vs. 58.1 years, P = 0.001). More patients with postoperative AKI had a history of hypertension (50% vs. 28.3%, P = 0.002). In addition, postoperative hospital stays were longer in patients who developed postoperative AKI when compared with patients without AKI (17.8 vs. 14.8 days, P = 0.001). In addition, patients with postoperative AKI had lower concentrations of Hb compared with patients without AKI (114.3 vs. 133.5 g/L, P = 0.001). Preoperative AFP concentrations were higher in patients without AKI (6979.9 vs. 2231.3 ng/mL, P = 0.001). Postoperative AKI patients demonstrated a higher CLIP score (29.2% vs. 9.1%, P = 0.001) and an increased CTP class B liver function (12.5% vs. 2.9%, P = 0.002). HCC patients with postoperative AKI demonstrated a higher rate of major liver resection (41.7% vs. 24.1%, P = 0.025).
Tumour size was increased (8.8 vs. 6.1 cm, P = 0.005), and the Milan criteria (29.2% vs. 57.2%, P = 0.001) was lower in patients with AKI compared with those without AKI. In addition, preoperative serum AST concentrations were higher in patients with postsurgical AKI (63.3 vs. 45.8 IU/L,P = 0.033).
Preoperative AST/ALT of patients with or without postoperative AKI
The mean preoperative serum AST/ALT in patients with postoperative AKI was significantly higher compared with that in patients without postoperative AKI (2.4 vs. 1.2, P = 0.007).
Predictive factors of postoperative AKI
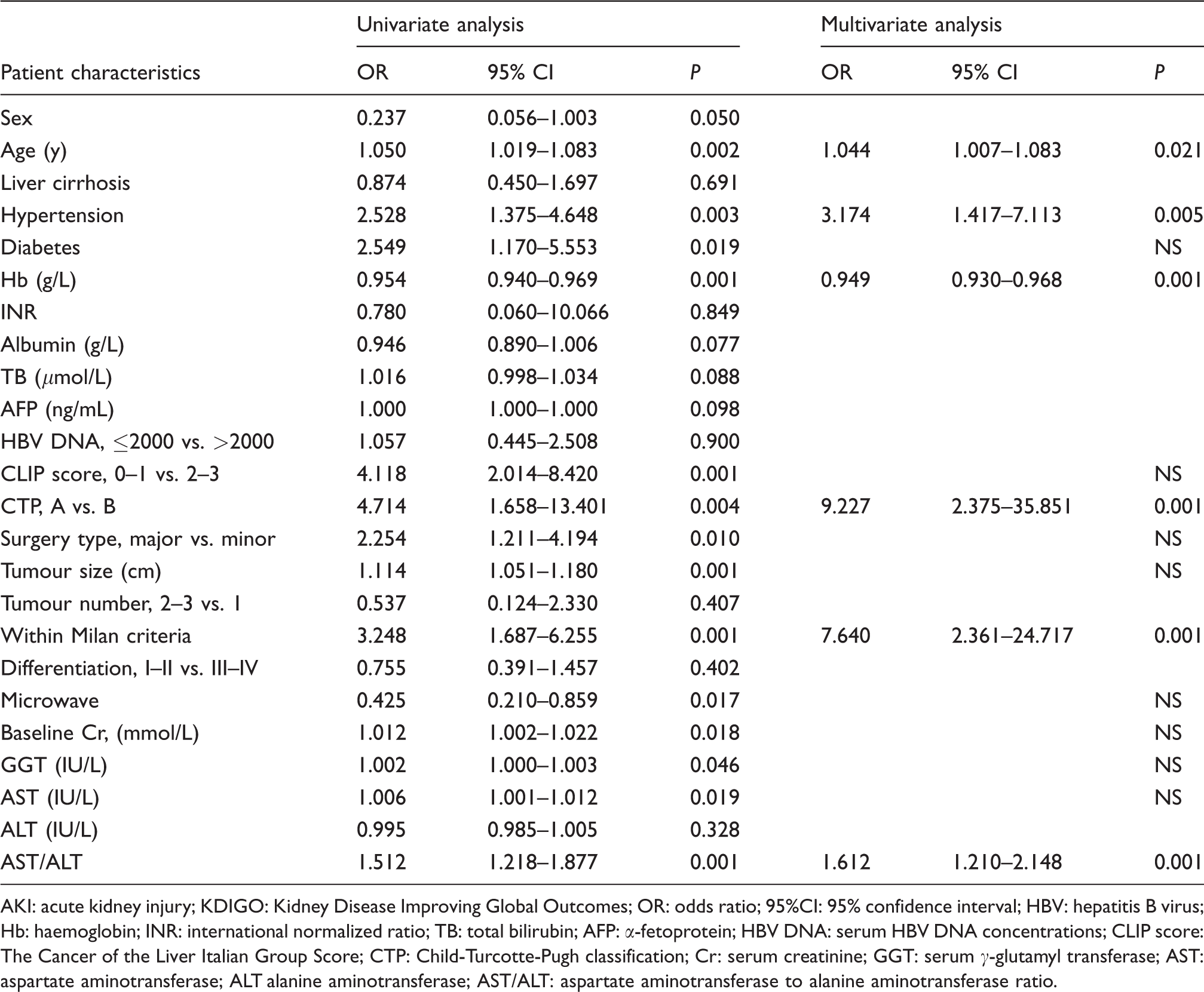
To identify the significant predictors of postoperative AKI, the AST/ALT and other clinical parameters were evaluated by univariate analyses using a logistic regression model (Table 2). After univariate analysis, age (OR 1.050, P = 0.002), hypertension (OR 2.528, P = 0.003), diabetes (OR 2.549, P = 0.019), Hb (OR 0.959, P = 0.001), CLIP score (OR 4.118, P = 0.001), CTP (OR 4.714, P = 0.004), type of surgery (OR 2.254, P = 0.010), tumour size (OR 1.114, P = 0.001), Milan criteria (OR 3.248, P = 0.001), microwave (OR 0.425, P = 0.017), baseline Cr (OR 1.012, P = 0.018), GGT (OR 1.002, P = 0.046), AST concentrations (OR 1.006, P = 0.019) and AST/ALT ratios (OR 1.512, P = 0.001) were subjected to the multivariate logistic regression analysis. In conclusion, multivariate analyses indicated that age, hypertension, Hb, CTP, Milan criteria and AST/ALT were independent predictors of postsurgical AKI in patients with HCC.
Univariate and multivariate analyses of postoperative AKI based on the ‘KDIGO’ criteria.
AKI: acute kidney injury; KDIGO: Kidney Disease Improving Global Outcomes; OR: odds ratio; 95%CI: 95% confidence interval; HBV: hepatitis B virus; Hb: haemoglobin; INR: international normalized ratio; TB: total bilirubin; AFP: α-fetoprotein; HBV DNA: serum HBV DNA concentrations; CLIP score: The Cancer of the Liver Italian Group Score; CTP: Child-Turcotte-Pugh classification; Cr: serum creatinine; GGT: serum γ-glutamyl transferase; AST: aspartate aminotransferase; ALT alanine aminotransferase; AST/ALT: aspartate aminotransferase to alanine aminotransferase ratio.
In this study, we demonstrate that an AST/ALT of 1.29 is the best cut-off point for predicting postoperative AKI in patients with HCC by ROC curve analysis. The AUC (95%CI) was 0.728 (0.648–0.808) (Figure 2). Specificity, sensitivity, negative predictive value (NPV) and positive predictive value (PPV) (95% CI) were 0.711 (0.662–0.756), 0.708 (0.557–0.826), 0.950 (0.916–0.971) and 0.239 (0.174–0.320), respectively. The ROC curve analysis revealed that an Hb cut-off point of 131.5 g/L showed the biggest Youden index (Figure 3). The AUC (95% CI) was 0.781 (0.723–0.840). Furthermore, we estimated whether an AST/ALT cut-off of 1.29 combined with an Hb cut-off of 131.5 g/L would improve the accuracy of prediction of postoperative AKI. Table 3 presents sensitivity, specificity, NPV and PPV (95%CI) of these variables either alone or in combination.
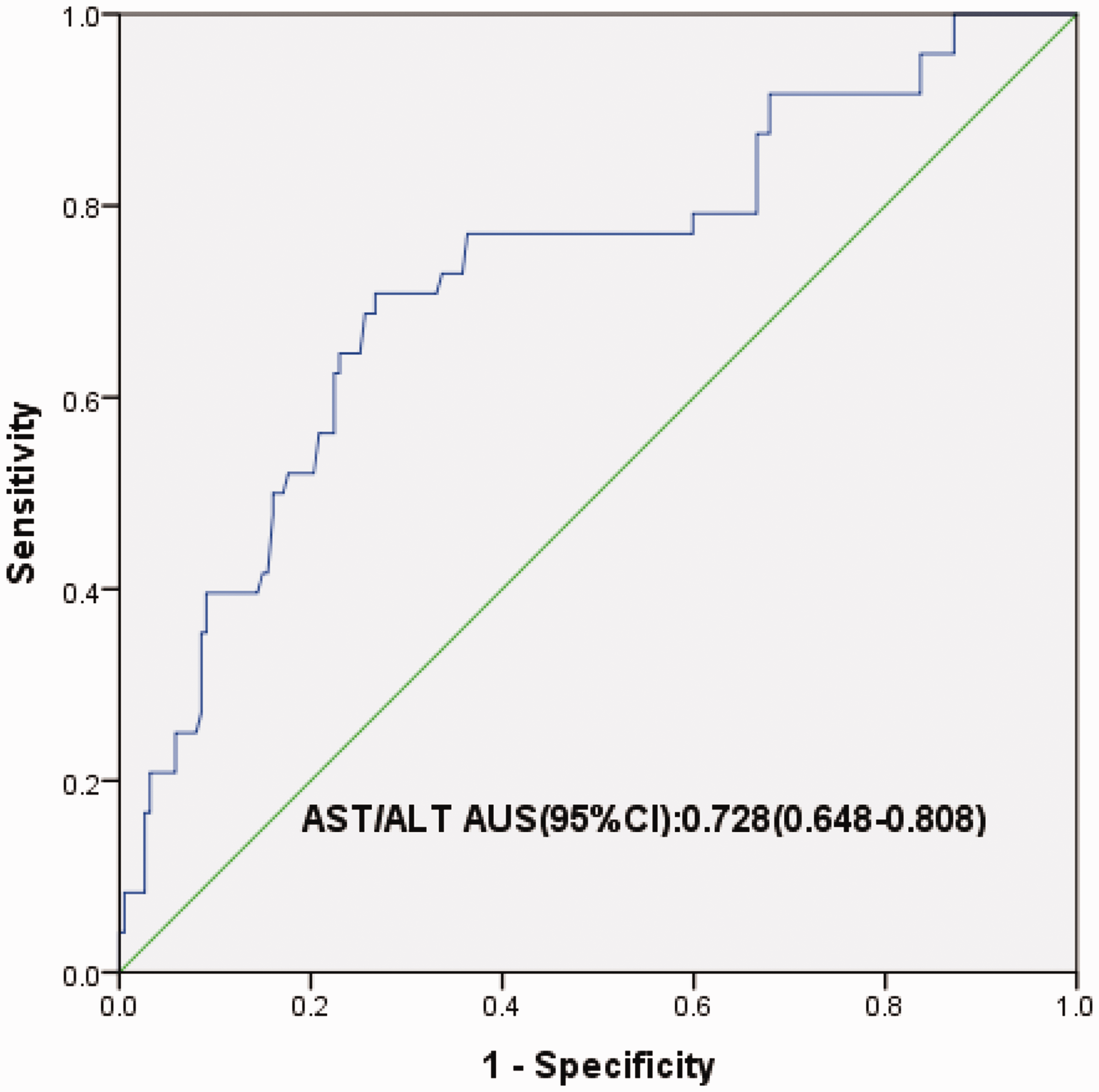
ROC curve of predicting postoperative AKI with AST/ALT.
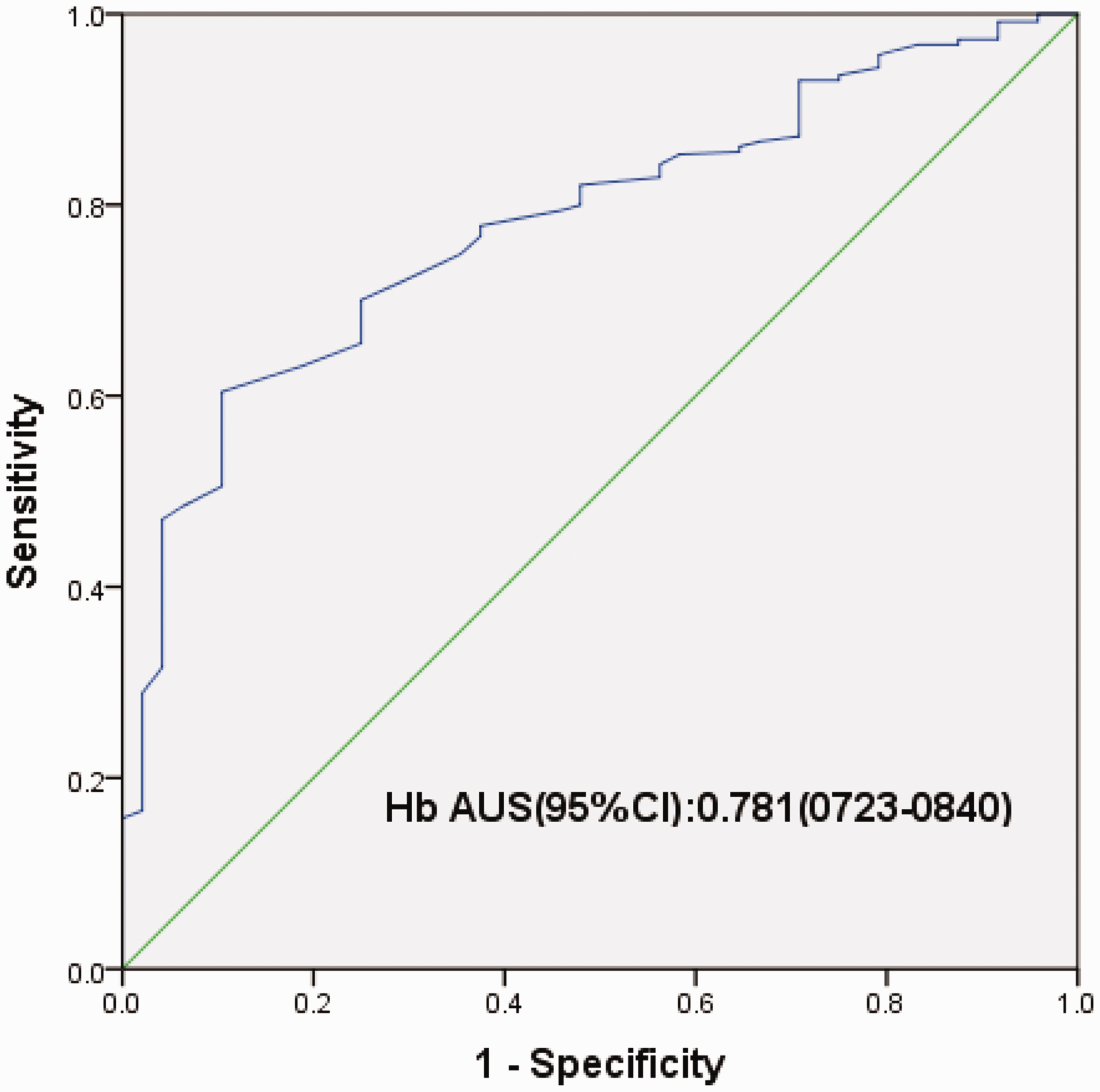
ROC curve of predicting postoperative AKI with Hb.
Sensitivity, specificity and negative and positive predictive values of an AST/ALT of 1.29 and haemoglobin of 131.5 g/L in the prediction of postoperative AKI.
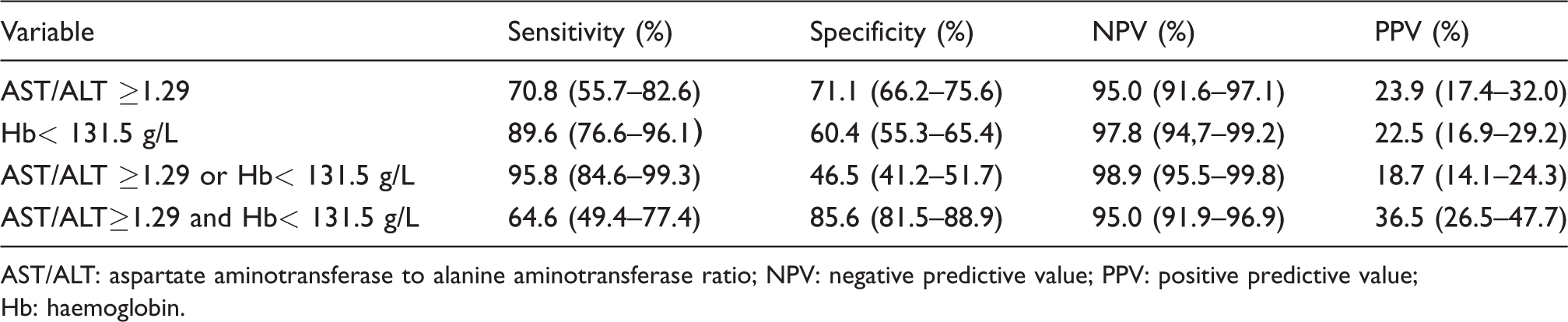
AST/ALT: aspartate aminotransferase to alanine aminotransferase ratio; NPV: negative predictive value; PPV: positive predictive value; Hb: haemoglobin.
Patients were divided into two groups based on the best AST/ALT cut-off point, including a high AST/ALT (≥1.29) group (n = 142) and a low AST/ALT (<1.29) group (n = 280). AST/ALT ≥1.29, as determined by univariate analysis with P < 0.05, was subjected to the multivariate logistic regression analysis. Taken together, AST/ALT values ≥ 1.29 were still independent predictors of postsurgical AKI after multivariate analysis.
Predictive factors of AKI after propensity score matching
After propensity score matching with Empower Stats software, 76 patient pairs with HCC were enrolled in a new analysis. Comparisons of the clinical data of 152 patients between the low and high AST/ALT were summarized, and none of the variables were significantly different between the low and high AST/ALT groups (all P > 0.05). After univariate analysis, variables with P < 0.05 were subjected to the multivariate logistic regression analyses. Moreover, age (OR 1.067, P = 0.020), hypertension (OR 4.294, P = 0.007), diabetes (OR 5.385, P = 0.013), GGT (OR 1.003, P = 0.045), Cr (OR 1.024, P = 0.029) and AST/ALT ≥1.29 (OR 10.947, P = 0.002) were prepared for multivariate analysis. After multivariate analysis, it was found that AST/ALT ≥1.29 (OR 24.281, P = 0.001) was still an independent predictor of postoperative AKI in patients with HCC.
Discussion
In this retrospective study, it was determined that based on the KDIGO criteria, the mean preoperative serum AST/ALT in HCC patients with postoperative AKI was significantly higher when compared with patients without postsurgical AKI. In addition, AST/ALT was also an independent predictor for postsurgical AKI in HCC patients who underwent hepatectomy. After propensity score matching, preoperative AST/ALT was still an independent predictor for postoperative AKI. In this study, an AST/ALT of 1.29 or more predicted 70.8% (95% CI, 55.7%–82.6%) of participants with postsurgical AKI and 71.1% (95% CI, 66.2%–75.6%) of patients without postsurgical AKI. The PPV of the AST/ALT ratio is actually quite poor. An Hb cut-off with the biggest Youden index in predicting HCC patients with postoperative AKI was identified by means of ROC curve and combined with AST/ALT to verify whether the predictive accuracy of AST/ALT could be improved. The combined assessment of these variables predicted 95.8% (95% CI, 84.6%–99.3%) of HCC patients with postsurgical AKI and 85.6% (95%CI, 81.5%–88.9%) of patients without postsurgical AKI. These findings suggested that preoperative AST/ALT might present a simple, low-cost and non-invasive plasma biomarker for postoperative AKI. In HCC patients with hepatitis B- or C-virus-associated infections, AST/ALT might be used as a novel predictive tool to evaluate the risk of postsurgical AKI. Thus, AST/ALT might help identifying HCC patients who are at a high risk for postsurgical AKI. Preventive measures could be performed in a more timely manner, 21 which might improve the outcomes of patients with HCC.
This retrospective study demonstrates an increased postsurgical hospital stay in patients with AKI, which is consistent with the findings presented in a previous study. 1 The finding that increased AST/ALT is related to postsurgical AKI linked to the occurrence of other postsurgical complications 1 might provide a potential explanation for the data presented in a previous study, which demonstrated that increased AST/ALT was associated with poor prognosis of HCC patients who underwent hepatectomy, particularly in patients with hepatitis B- or C- virus-associated HCC. This study also found that univariate regression analysis identified microwave ablation of the intraoperative liver section as an associated factor with postoperative AKI. We speculate that the destruction of red blood cells and other necrotic substances produced by ablation were absorbed by the body and these might play an important role in the occurrence of postoperative AKI. However, further basic research is still needed to confirm this prediction.
The AST/ALT has been extensively applied to assess the progression of functional liver impairment and to predict the degree of liver fibrosis for over a decade.15,16,22–27 Moreover, the AST/ALT is used as a prognostic factor in patients with primary biliary cirrhosis. 28 Several studies have demonstrated that there is an inverse relationship between high serum concentrations of ALT within a reference range and all-cause mortality in middle-aged-to-elderly individuals and cardiovascular disease outcomes.29,30 It has been reported that serum ALT concentrations demonstrated an inverse relationship with age, whereas serum concentrations of AST remained stable. 31 Most studies do not provide a clear explanation for the increased AST/ALT when liver disease and adverse outcomes worsen. Therefore, the reasons behind these finding need to be elucidated.
Both AST and ALT are circulating enzymes that are primarily synthesized by the liver. In addition, high concentrations of AST are present in the heart, skeletal muscles, kidneys and red blood cells. ALT is localized solely in cellular cytoplasm, whereas AST is found in both cytoplasm and mitochondria. The half-life of total AST is roughly 17 h, the average half-life of mitochondrial AST is 87 h, and the half-life of ALT is roughly 47 h. 15 Changes of synthesized ALT and stored AST concentrations have been used as diagnostic tools and markers for assessing liver function. As mentioned before, AST/ALT is closely linked with liver dysfunction and cirrhosis. 15 Furthermore, cirrhosis and liver dysfunction might cause visceral vasodilatation, causing hormonal imbalances that ultimately result in renal vasoconstriction and impaired renal function. This might present a potential mechanism of hepatorenal syndrome, one of the aetiologies of AKI.32,33 Both AST and ALT serve as indicators for HBV infection, 12 which is related to nephropathy. 13 Several studies have confirmed that HBV antigen and HBV DNA are found in epithelial cells of renal tubules.13,34 The extraction of immune complexes in the kidneys indicates that the immune complex might participate in the pathogenesis of hepatitis B virus-correlated nephropathy. 13 In a prior experimental study, it was demonstrated that the replication of HBV might participate in apoptosis of renal tubular cells (RTC), and that HBV-directed infection in RTC results in cellular apoptosis. 35 Furthermore, apoptosis is considered an active mode of cell death and promotes cell loss during both acute and chronic renal damage. 35 It has been reported that serum of patients with HBV infection might promote apoptotic injury in RTC by triggering a pathway that involves Fas up-regulation. 35 The detailed mechanism of hepatitis B virus-associated nephropathy remains to be elucidated and needs further investigation.
Inflammation-associated components, such as serum AST and ALT, are generally accepted as better predictors of liver injury. Moreover, it has been found that ALT is related with oxidative stress and systemic inflammation, which are related to therapeutic reactions. 36 The liver can easily be exposed to internal stimuli, which produce reactive oxygen species (ROS). Inflammation and oxidative stress might participate in RTC-related injury as a result. Some experimental evidence has demonstrated that O2−1 could result in increased intracellular calcium concentrations, leading to vasoconstriction of the kidney, decreased kidney blood flow and glomerular filtration rate, thereby leading to renal injury.37–39 In addition, reports have demonstrated that the majority of hypertension patients with decreased antioxidant ability and increased generation of ROS, had progressive renal damage. 40 Moreover, it has been reported that antioxidant treatment prevents renal injury and improves renal dysfunction. 41 These findings indicate that inflammation and oxidative stress may play a beneficial role in kidney injury. However, large-scale clinical studies and an increasing number of experimental studies will be required to confirm the relationship of AST/ALT with postoperative AKI. Future exploration of the mechanisms involved is critical.
Although promising, our study has some limitations. First, this is a retrospective and unicentral study, and the occurrence rate of postoperative AKI was low (11.4%) and the number of enrolled cases was small. Consequently, large-scale multicentral prospective cohort studies would be required to confirm the result. Second, the inclusion criteria were restricted to patients with BCLC 0, A staged hepatitis B- or C- virus-associated HCC. However, it might represent true clinical situations that not all HCC patients are suitable for hepatectomy. In addition, the applications of preoperative AST/ALT on the prediction of postoperative AKI for other surgical patients still need to be elucidated. Third, experimental studies focusing on the relation between AST or ALT and AKI are limited. Therefore, these study results are not entirely satisfactory. Additional experimental studies will be required to confirm the relationship of AST/ALT with postoperative AKI, and the underlying mechanisms of action would need to be explored. Despite these drawbacks, our study was the first to report potential predictive values of the preoperatively evaluated AST/ALT for postoperative AKI in HCC patients. Furthermore, additional analyses may provide even more evidence to confirm this result.
Conclusions
The mean preoperative serum AST/ALT in HCC patients with postoperative AKI was significantly higher compared with those without postsurgical AKI. In addition, preoperative AST/ALT might be a potential independent predictor of postsurgical AKI in HCC patients who have undergone hepatectomy. An AST/ALT of 1.29 was the best cut-off point for predicting postoperative AKI in patients with HCC. Further studies, ideally in a prospective design, may be warranted to examine the utility of preoperative AST/ALT as a non-invasive predictive tool to evaluate the risk of postsurgical AKI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No. 81372668), Natural Science Foundation of Hubei Province (No. 2017CFB179), Foundation of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (No. 02.03.2017–331).
Ethical approval
This retrospective study was approved by the Tongji Medical College research ethics committee, Wuhan, China (NO: IORG0003571).
Guarantor
QZ.
Contributorship
JX, YX, GW and QZ researched the literature and conceived the study. SL, XC, SH, XZ and YG were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. JX and YX wrote the first draft of the article. All authors reviewed and edited the article and approved the final version of the article.