
Abstract
Background
We investigated the percentage of patients diagnosed with the correct underlying cause of anaemia by general practitioners when using an extensive versus a routine laboratory work-up.
Methods
An online survey was distributed among 836 general practitioners. The survey consisted of six cases, selected from an existing cohort of anaemia patients (n = 3325). In three cases, general practitioners were asked to select the laboratory tests for further diagnostic examination from a list of 14 parameters (i.e. routine work-up). In the other three cases, general practitioners were presented with all 14 laboratory test results available (i.e. extensive work-up). General practitioners were asked to determine the underlying cause of anaemia in all six cases based on the test results, and these answers were compared with the answers of an expert panel.
Results
A total of 139 general practitioners (partly) responded to the survey (17%). The general practitioners were able to determine the underlying cause of anaemia in 53% of cases based on the routine work-up, whereas 62% of cases could be diagnosed using an extensive work-up (P = 0.007). In addition, the probability of a correct diagnosis decreased with the patient’s age and was also affected by the underlying cause itself, with anaemia of chronic disease being hardest to diagnose (P = 0.003).
Conclusion
The use of an extensive laboratory work-up in patients with newly diagnosed anaemia is expected to increase the percentage of correct underlying causes established by general practitioners. Since the underlying cause can still not be established in 31.3% of anaemia patients, further research is necessary.
Introduction
Anaemia (i.e. a lowered concentration of haemoglobin) is a common finding among elderly patients (aged 65 years and older) in general practice. Besides the sign of an underlying condition, it has long been considered a benign consequence of aging. However, during the last decade, many studies have been published detailing the relevance of anaemia, such as the associations between anaemia and increased mortality, physical and cognitive decline, cardiovascular events and reduced quality of life have been found.1,2 The only way to manage anaemia is through treatment of the underlying cause, which requires an additional diagnostic work-up. The most common underlying causes of anaemia in general practice are iron deficiency anaemia (IDA) (16.3%–19.0%), anaemia of chronic disease (ACD) (19.7%–31.4%) and renal anaemia (8.2%–12.9%). In addition, a considerable proportion of anaemia cases have no clear cause and are classified as unknown anaemia (31.3%–44.0%) (see literature,3–6 own data).
Different guidelines are published to help diagnosing the underlying cause of anaemia. In most of them, mean corpuscular volume (MCV) occupies a central position.7,8 However, Oosterhuis et al. 9 demonstrated that when assigning a major role to ferritin concentration instead of MCV, leads to an increase of the percentage of patients diagnosed with an underlying cause from 48% to 71%. In addition, another study has shown that the percentage of patients diagnosed with an underlying cause of anaemia increases from 14% when general practitioners (GPs) personally order laboratory analysis to 53% when a standard set of 14 laboratory parameters was offered. 10
The high prevalence of anaemia, as well as the need for establishing the underlying aetiology prior to initiating treatment, demands an optimized diagnostic approach. We used an online survey among GPs to establish whether a routine or extensive laboratory approach is more effective in diagnosing the underlying cause of anaemia in general practice.
Materials and methods
Study design
The percentage of correct diagnoses of the underlying cause of anaemia when using an extensive versus a routine laboratory work-up was investigated through an online survey using LimeSurvey. 11 The survey was distributed among 836 GPs, operating in different parts of the Netherlands and was available online for a period of one month (January 2016). The cases used in this survey were selected from a large database of GP patients, included between the 1 February 2007 and 1 February 2015 (n = 3325). 12 This prospective cohort study was approved by the internal ethics committee of the Albert Schweitzer Hospital. The database consisted of patients aged 50 years and older (in order to exclude a predominance of iron deficiency due to hypermenorrhoea), newly diagnosed with anaemia (i.e. no established diagnosis of anaemia in the previous two years). Anaemia was defined as haemoglobin below 13.7 g/dL (8.5 mmol/L) for males and below 12.1 g/dL (7.5 mmol/L) for females. An extensive laboratory work-up was performed in all included patients, consisting of haemoglobin (Hb), MCV, C-reactive protein (CRP) and/or erythrocyte sedimentation rate (ESR), vitamin B12, creatinine, ferritin, folic acid, lactate dehydrogenase (LDH), transferrin, reticulocytes, leukocytes, thrombocytes and serum iron. According to the current guidelines about anaemia diagnostics in general practice, these 14 parameters cover all underlying causes of anaemia that can be diagnosed in general practice. 7
Distribution of underlying cause of anaemia.
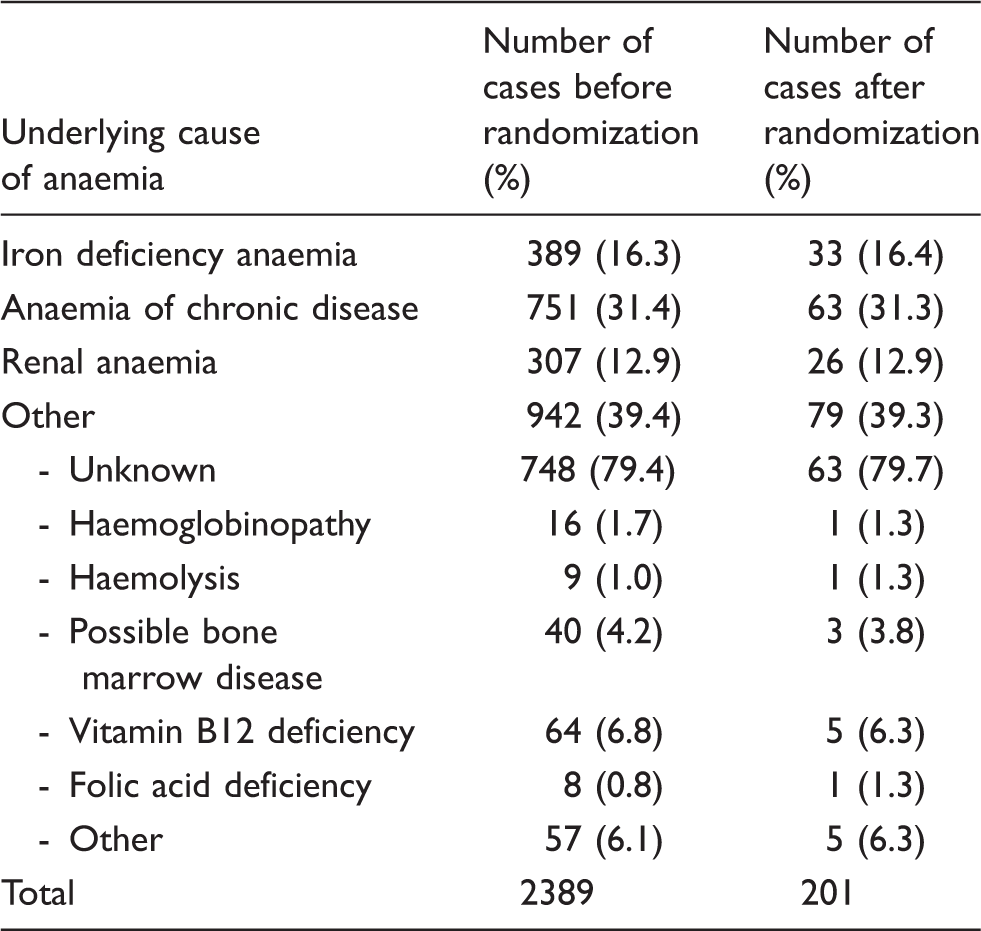
Note: The distribution of the underlying causes of anaemia in the larger data-set of newly diagnosed anaemia patients was used to randomly select 201 cases with a similar distribution.
Structure of online survey
For each participating GP, the survey included six patient cases which were randomly selected by LimeSurvey from the set of 201 available cases. For each case, GPs were provided with the age and gender of the patient and were informed that the patient presented with suspicion of anaemia. While filling in the survey, respondents were invited to use guidelines or other tools they also use in daily practice. For the first three cases, respondents were asked to choose the laboratory tests they considered necessary from the predefined list of 14 parameters. This was referred to as the ‘routine work-up’. The respondents were then presented with the results of the selected laboratory tests and were invited to determine the underlying cause of anaemia when possible. In cases where they responded that additional information was required, they were given one opportunity to request additional tests from the same list of 14 tests. No limit was set on the number of laboratory tests that could be selected per analysis, but the same test could not be ordered twice. For the second set of three cases, respondents were presented with the results of all 14 tests, and they did not have the ability to request additional tests. This was referred to as the ‘extensive work-up’. Again, respondents were asked to determine the underlying cause of anaemia. The survey ended with several personal questions regarding the GPs’ gender, age, years active as GP, zip code, daily use of guidelines for the diagnosis/treatment of anaemia patients and whether the GP had any special affinity with the subject of anaemia. The diagnoses of the respondents were compared with the diagnoses of the expert panel. For the cases with IDA, ACD and renal anaemia as underlying cause, the diagnoses had to be in accordance with the diagnoses of the expert panel. For all other underlying causes (i.e. vitamin B12 deficiency, unknown cause, et cetera), the diagnosis was considered correct if the option IDA, ACD or renal anaemia had not been chosen by the respondent. This classification is a commonly used method in literature and was considered appropriate as diagnosing or excluding of the three most prevalent underlying causes is clinically the most relevant.3–6
A sample of the survey is shown in supplemental data 2. The percentage of correct underlying causes of anaemia as established by GPs was defined as ‘effectiveness’ and is referred to as such throughout this manuscript.
Statistical analysis
The patient population was described by standard descriptive statistics. An additional analysis was performed to confirm that the choice of laboratory test(s) requested by the GP was in accordance with the diagnosis established by the same GP. The effects of the characteristics of both the patient case and the responding GP on the probability of a correct diagnosis were analysed using generalized linear mixed models with a logistic link function and a binomial error distribution (i.e. logistic regression analyses with random effects). 15 These models take into account the correlations between observations due to repeated measurements for both cases and respondents and can handle data with missing observations in the outcome. In the analysis of the effectiveness of the routine versus the extensive laboratory work-up, the dependent variable was a dichotomous variable, indicating whether the case had been diagnosed correctly, and the independent variables were type of work-up (i.e. routine or extensive), age and gender of the case and the cause of anaemia as established by the expert panel. This model was also used for the analysis of the effect of GP characteristics on correct diagnoses, but with the following variables added as independent variables: number of years of working experience as GP, use of guidelines, and whether the respondent had specific affinity with anaemia. GPs with missing information on any of these GP characteristics were excluded from the latter analysis (n = 16 [11.5%]). To take into account correlations due to repeated measurements, the relevance of including random effects of both cases and respondents was determined with the Akaike information criterion. Based on this criterion, only random effects of cases were included in the final model. The data were analysed using IBM SPSS Statistics, version 24 and R version 3.3.1 with the NLME package.16,17 All statistical tests were two-sided, and P-values lower than 0.05 were considered significant.
Results
Respondents’ online survey
A total of 125 respondents (15%) completed the survey, resulting in 375 complete cases for both the routine and extensive work-up. In addition, 14 respondents (1.7%) filled in only part of the survey, resulting in an additional 29 cases in the routine work-up (total 404 cases) and three cases in the extensive work-up (total 378 cases) (Figure 1).
A flow diagram showing the general practitioners who responded to the survey.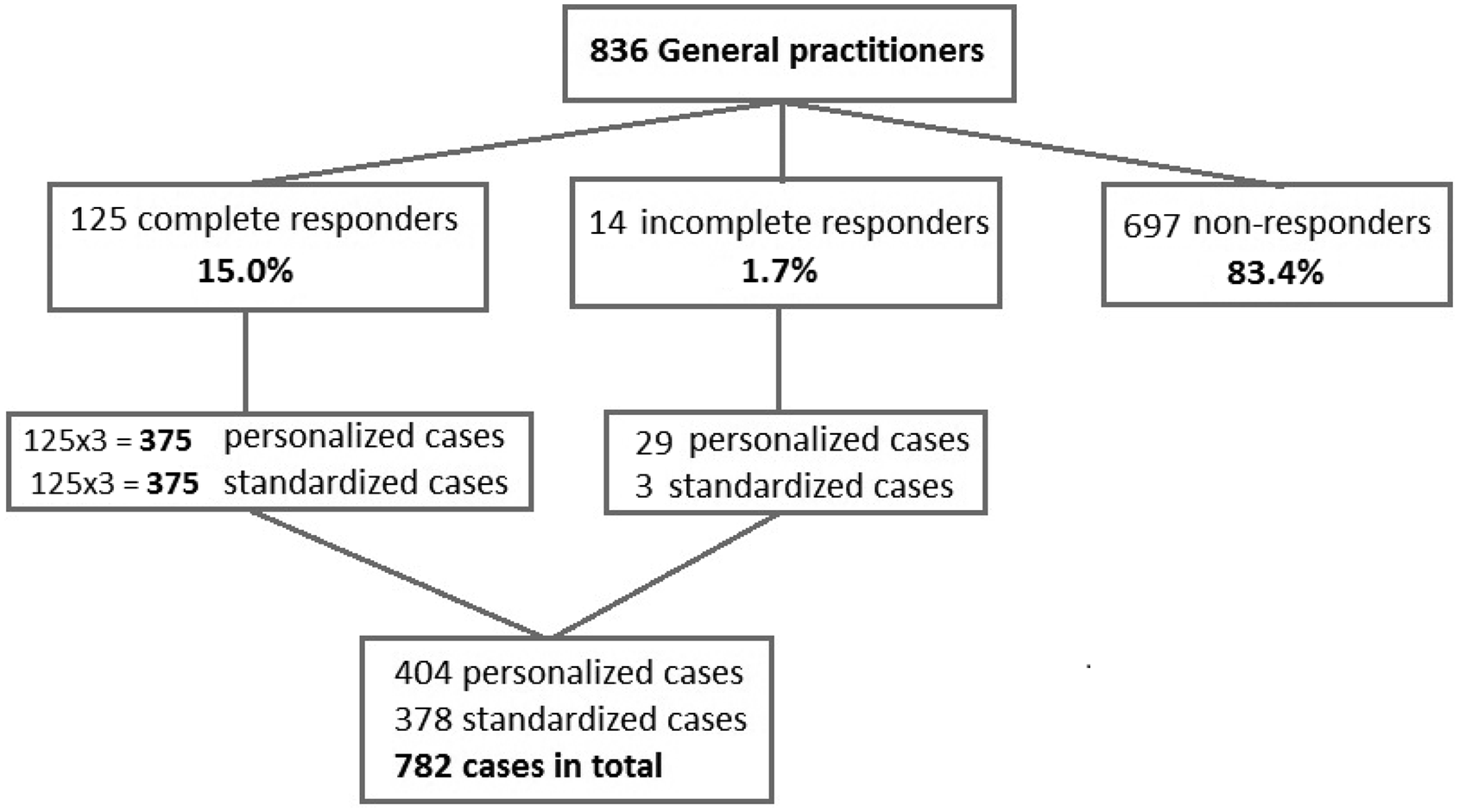
Of all 139 respondents, 123 (89.5%) answered the questions regarding personal characteristics. According to the NIVEL institute (Netherlands Institute for Health Services Research), the proportion of males participating in this survey as compared with the overall population of GPs (55.6% versus 55.0%), as well as the median age (48 years versus a median age category of 45–49 years) did not show major differences, suggesting that the respondents are a representative sample of the overall GP population in the Netherlands. 18
Effect of diagnostic work-up on correctly diagnosing anaemia
Routine requested laboratory analysis of GPs.
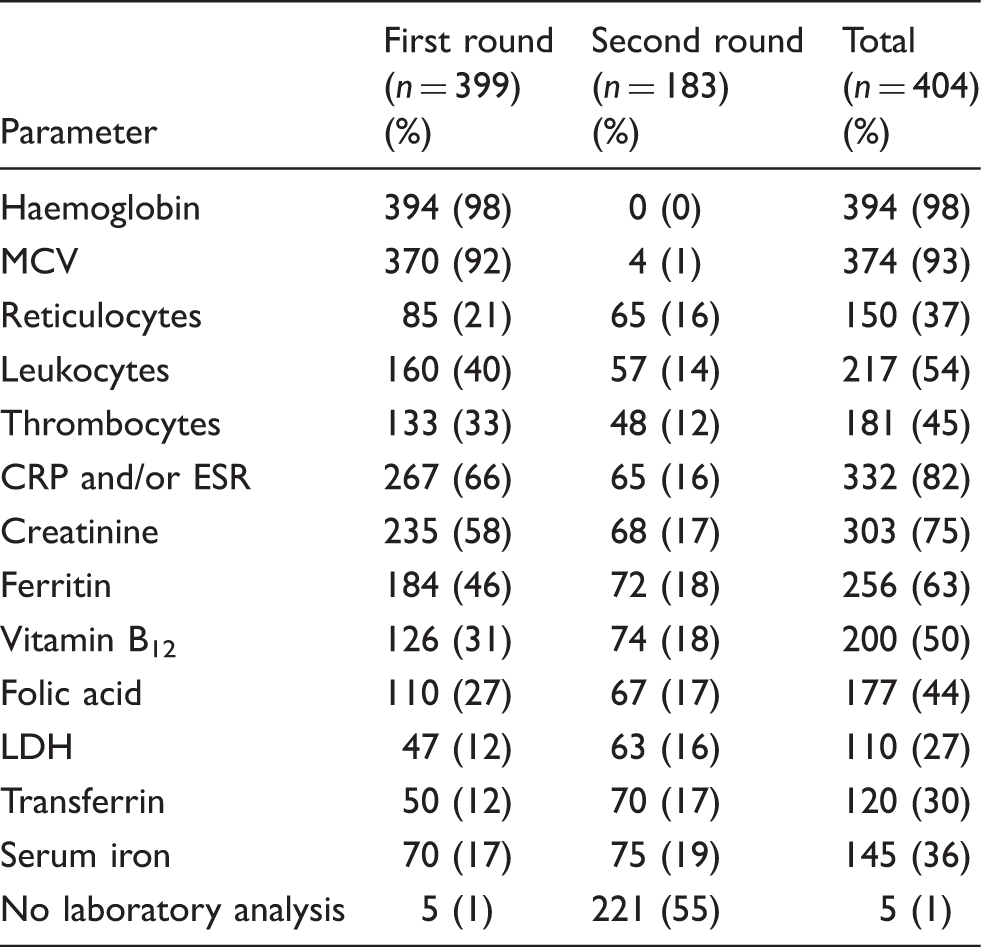
Note: Of the 404 cases assessed with a routine work-up, laboratory tests were ordered once in 216 cases (53.5%) and twice in 183 cases (45.3%). The requested tests are shown as number (percentage).
LDH: lactate dehydrogenase; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; MCV: mean corpuscular volume; GP: general practitioner.
Diagnosis of underlying cause of anaemia using a routine or extensive work-up.
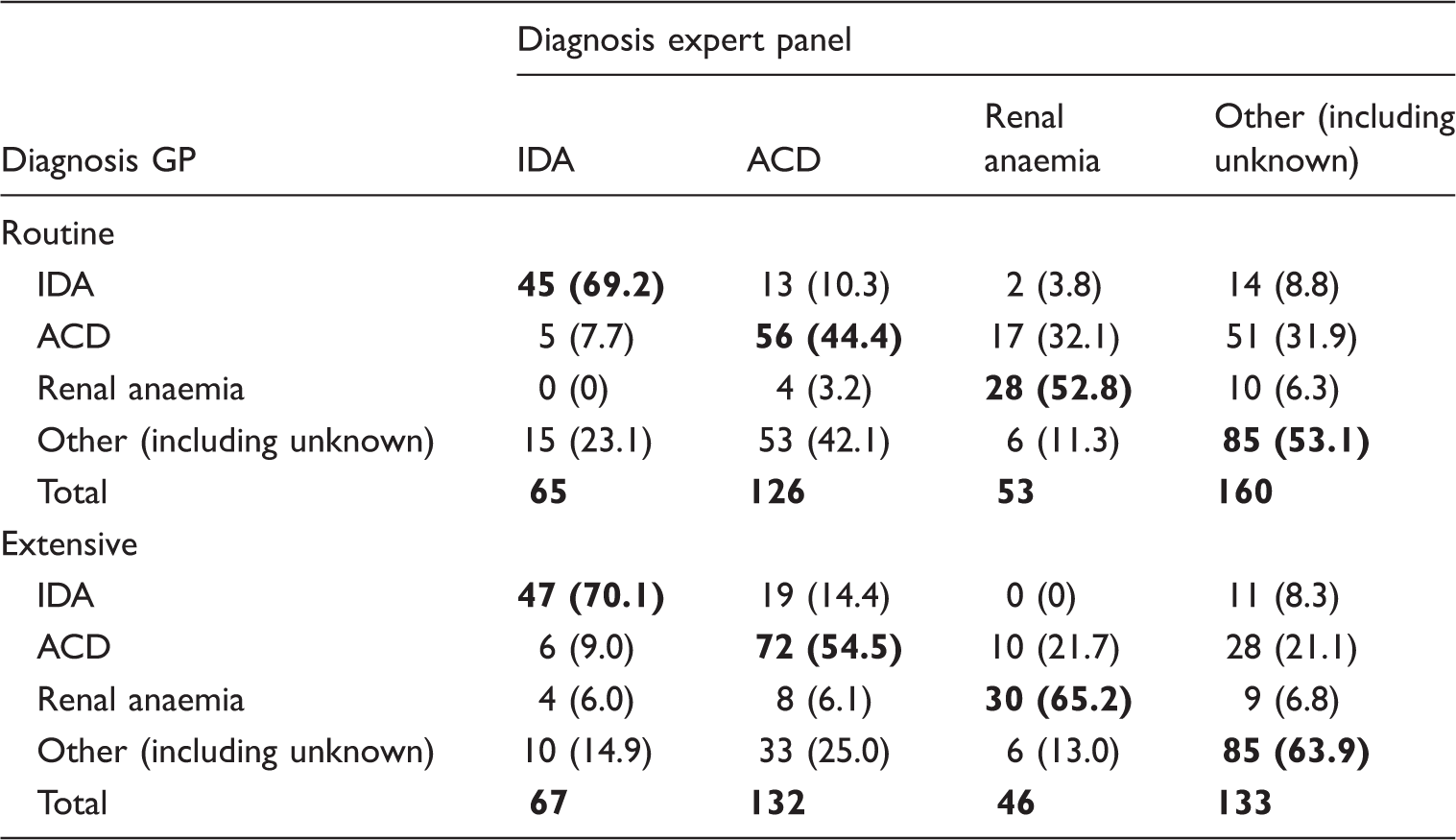
Note: The diagnosis set by the GPs is showed against the diagnosis set by the expert panel for both routine and extensive work-up. The bold values are the correct diagnoses.
GP: general practitioner; ACD: anaemia of chronic disease; IDA: iron deficiency anaemia.
Multivariate analysis of the efficacy of extensive versus routine laboratory work-up.
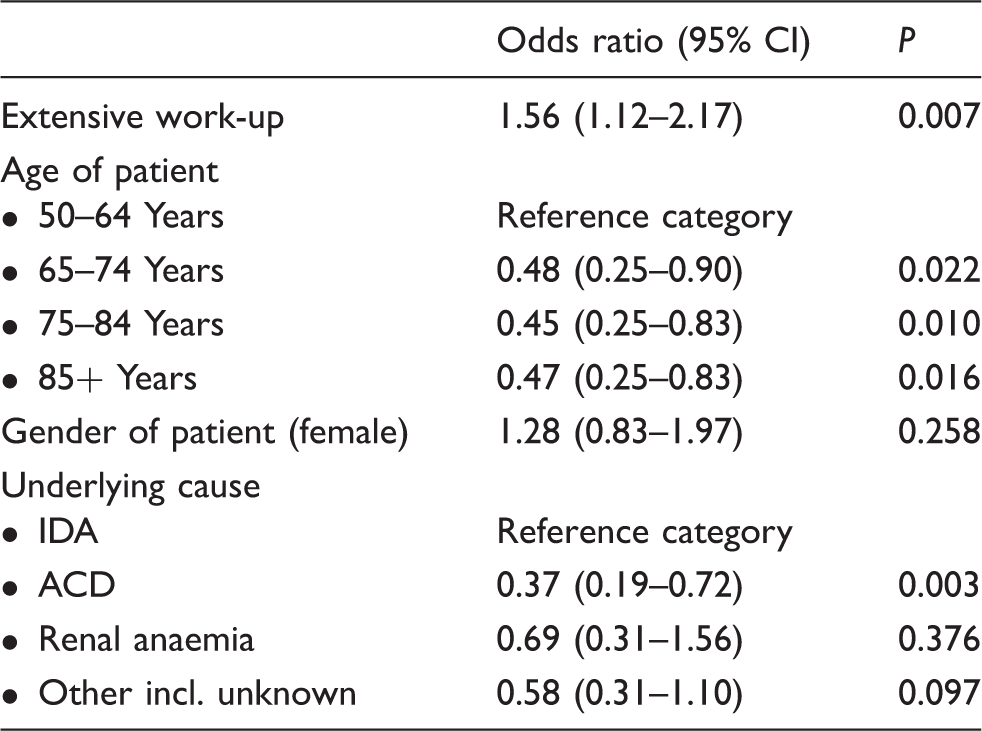
Note: Multivariate analysis using a generalized linear mixed model showed a significant influence of the laboratory work-up, age of patient and the underlying cause of anaemia itself on the correct diagnosis of the underlying cause of anaemia.
Multivariate analysis of the effect of GPs characteristics on the correct diagnosis of the underlying cause of anaemia.
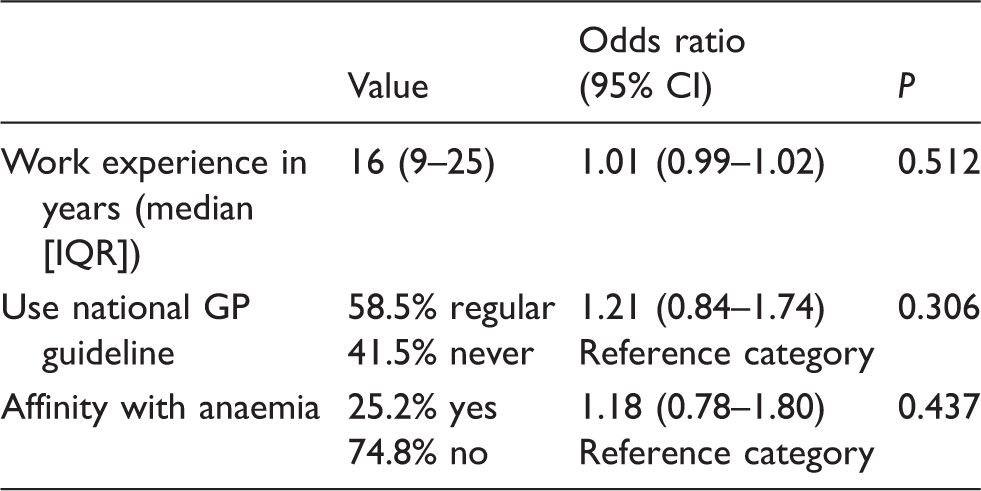
Note: Results based on a generalized linear mixed model that also included work-up type (i.e. routine or extensive), age and gender of the case, and the cause of anaemia as established by the expert panel as independent variables. Of all 139 respondents, 123 (89.5%) answered the questions regarding personal characteristics. None of the analysed characteristics showed a significant effect on the probability of diagnosing the correct underlying cause of anaemia.
Discussion
When diagnosing the underlying aetiology of anaemia, laboratory tests can be selected by the GP (i.e. routine work-up) or a standard set of tests may be offered by the laboratory (i.e. an extensive work-up). To determine which work-up would be more effective in supporting the GP to diagnose the correct underlying cause of anaemia, we compared both approaches using an online survey among GPs. Our study included 14 widely available laboratory tests, which are all recommended by the current Dutch anaemia guideline. This extensive laboratory work-up was shown to be more effective than a routine work-up, in which GPs could order laboratory tests twice (from this predefined set of 14 tests). Patient characteristics (aged 65 years and older) and the underlying cause itself (i.e. ACD) may negatively affect the probability of a correct diagnosis.
For many years, anaemia diagnosis was directed by MCV, which divided cases into microcytic, normocytic and macrocytic, with each category including a set list of causes. In recent years, several studies have shown that MCV should not be granted such a central role. Relevance of mean corpuscular volume for the evaluation of anaemia in general practice. Manuscript submitted for publication).19,20 However, in this study, MCV was still the second most often requested test during the first round of the routine work-up (93%), suggesting that GPs still follow the old classification system. This approach may lead to missed causes since, for example, a microcytic anaemia will lead to the exclusion of vitamin B12 deficiency as a possible cause according to the old classification system, while in fact, this deficiency may still be present and contributing to the anaemia. 19 In addition to MCV, the most requested tests during the first round of the routine work-up are CRP/ESR (67%), creatinine (59%) and ferritin (46%). These three tests allow for the exclusion of the three most common causes of anaemia, namely ACD (CRP and ferritin), renal anaemia (creatinine) and IDA (ferritin). This suggests that GPs, when ordering tests, first aim to diagnose or exclude the three most common causes of anaemia.
This study also demonstrated that increased age (65 years and older), decreases the likelihood of establishing the correct underlying cause of anaemia independently from the laboratory work-up. This may be due to the fact that older patients more often display slightly increased infection parameters.21,22 This abnormality in the laboratory results, in combination with consensus-based definitions of underlying causes, might confuse GPs when determining the underlying cause of anaemia. In addition, it is important to realize that the elderly often have multiple diseases or co-morbidities and each of those may (individually) contribute to anaemia. Especially in these patients, the laboratory results might be of less relevance and the clinical presentation (i.e. health condition) would be the guiding principle for treatment. This may have created complications for GPs while attempting to establish the cause in this study, since the survey relied entirely on laboratory results and did not include health condition or co-morbidities of the patient. However, there was no increase in the percentage of cases that were diagnosed as ‘unknown’ by GPs among the elderly (data not shown). Finally, since the elderly often have multiple diseases or co-morbidities, GPs may be reluctant to commit to an extensive diagnostic process and therefore only perform limited laboratory analyses in this group of patients.
The actual underlying cause of anaemia may also affect the probability of a correct diagnosis by GPs, with ACD being the most difficult to diagnose. The interpretation of laboratory values can be challenging when ACD is present, especially in multiple causes, for example when an ACD co-exists with an iron deficiency. This combination was not present in the cases selected in our study. However, the cases in this study were classified by an expert panel according to pre-determined definitions of underlying causes of anaemia. These definitions were based both on existing guidelines and on the opinion of this expert panel. 23 As a result, we used a strict cut-off value of ferritin (i.e. >100 µg/L) in the diagnosis of ACD. A participating GP may have used a different cut-off value or a different definition of ACD, based on his or her own experience. For the purpose of this study, the answer of these GPs may thus have been classified as incorrect and the number of correct diagnoses would, in fact, be higher. Furthermore, some causes have a very low prevalence in general practice. Being less familiar with these causes and their current definitions may make diagnosing them more challenging.
This study showed that the percentage of correct diagnoses of the underlying cause of anaemia increased from 53.0% when using a routine laboratory work-up to 61.9% when using an extensive laboratory work-up. Taking into consideration that annually 57,000 patients aged ≥50 years present with a new anaemia in Dutch general practice, this modest absolute difference of almost 9% will benefit a large number of patients (approximately 5130 patients) in whom the underlying aetiology of anaemia can be established.24,25 Moreover, the extensive laboratory work-up is also expected to be cost-effective compared with the routine work-up, as is shown by the accompanying article by our group, published elsewhere in this journal.
Strengths and limitations
This study aimed to investigate which type of diagnostic work-up (i.e. extensive versus routine) results in the most correct diagnoses of the underlying cause of anaemia. To achieve this, we used real-life patient data from a large transmural project. The participating GPs showed no differences in age and gender compared with the overall population of GPs in the Netherlands, suggesting that the participating GPs are an appropriate representative sample of the Dutch GP population. A possible limitation of this study is the lack of clinical information in the cases of the survey, besides age, gender and the suspicion of anaemia. This clinical information may be of considerable importance in the diagnosis of the underlying cause of anaemia. Addition of this information may have allowed for a higher percentage of correct diagnosis. However, neither approach (routine and extensive work-up) contained this information and thereby this drawback did not affect the difference in percentage of correct diagnoses between both approaches. In addition, the cases were randomly assigned to the GPs, which mean that there was a small chance that the same cause could have been the result for all six of the cases presented to a GP. This may cause the GP to perform better or worse, as this study has shown that the underlying cause itself has an effect on correctly diagnosing. However, since this scenario is also possible in daily practice, the survey reflects a real-word situation. In addition, five cases in whom the GP requested no laboratory test(s) were included in the final analysis because it was deemed a conscious choice of the GPs. In this study, we excluded anaemia with multiple aetiologies, since this is not addressed in the Dutch anaemia guideline and in order to avoid statistical complexity (i.e. more power would be needed against lower prevalence). In the routine laboratory work-up, multiple aetiologies might be missed if additional laboratory tests are withheld once an underlying cause is established. Therefore, it is to be expected that the extensive laboratory work-up performs better in the diagnosis of multiple aetiologies than the routine work-up, since all additional laboratory are simultaneously performed, making multiple aetiologies immediately apparent. Finally, each survey started with three cases for the routine work-up followed with three cases for the extensive work-up. This might have led to an overestimation of the effectiveness of the extensive work-up, since GPs have practiced and possibly learned from the previous cases and apply this to the following cases. However, to ensure that GPs chose the routine laboratory analysis based on their own experience, it was not possible to first show the cases of the extensive laboratory work-up, as this would have led to a larger bias.
Conclusion
An extensive laboratory work-up in patients with newly diagnosed anaemia is more effective in finding the underlying aetiology than a routine laboratory work-up selected by GPs. Nevertheless, the percentage of incorrect diagnoses remains significant, which should take into account the fact that stand alone laboratory diagnostics is not the gold standard for anaemia diagnostics. Further studies should focus on an extensive laboratory work-up and the added value of multidisciplinary diagnostic approaches in patients with anaemia.
Footnotes
Acknowledgements
We thank the participating general practitioners for their generous contribution. In addition, the authors thank Dr Rebecca Buis for critical reading of the manuscript. This paper was previously presented at the Science day, Albert Schweitzer Hospital, on June 2017.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The database was approved by the internal ethics committee of the Albert Schweitzer Hospital.
Guarantor
MDL
Contributorship
AS and MMAK contributed equally to this article. AS, MMAK, KS, SD, MDL, and RK were involved in the conception and design of the study and performed the data collection. AS, KS, MDL and JVR analysed the data. All authors were involved in interpreting the results. AS drafted the manuscript, and all other authors were major contributors in critically reviewing the manuscript. All authors read and approved the final version of the manuscript.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.