
Abstract
Background
Thyroid-stimulating hormone (TSH) receptor (TSHR) autoantibodies (TRAbs) are a heterogeneous group of antibodies (Abs) with different functionalities. Among all TRAbs, only the stimulating ones (S-TRAbs) are considered as the pathogenetic marker of Graves’ disease (GD). To date, the methods available for TRAbs testing are based on immunoassays (IMAs) which detect total serum TRAbs or bioassays which are not suitable in clinical practice, even though they discern Abs functionality. The aim of our work was to evaluate the analytical and clinical performance of a very recent IMA (Immulite TSI method), supposed to test only the serum concentration of S-TRAbs, in comparison with a current method for total TRAbs (Roche/Elecsys IMA).
Methods
We evaluated serum samples of 145 subjects: 46 with untreated (GD), 36 with chronic autoimmune thyroiditis, 3 with atrophic thyroiditis, 10 with multinodular non-toxic goiter and 50 healthy subjects.
Results
The method showed an optimal analytical sensitivity and high precision levels (LoB: 0.04 UI/L, LoD:0.07 UI/L, LoQ:0.14 UI/L, intra-assay CV: 4.2–5.9%, inter-assay: 4.5–7.2%). By receiver operating characteristics curve analysis, we obtained a value of 0.57 (sensitivity: 98.0%, specificity: 99.9%) as the best cut-off to distinguish GD, apart from four cases. Passing Bablok regression and Bland Altman analysis pointed out a good correlation and agreement with Roche method (R2 = 0.98, slope = 1.03, bias = −2.70).
Conclusions
The new method presents very promising analytical characteristics and could be adopted in clinical practice for GD diagnosis. Moreover, the test allows to accurately detect very low values of analyte with a further clinical utility in detecting earlier possible relapses.
Introduction
Graves’ disease (GD) is one of the most common autoimmune pathology with an incidence in people of approximately 14/100,000. GD is the cause of the 70–80% of thyrotoxicosis, even though its predominance can vary among different populations, according to iodine exposure.1,2 Once hyperthyroidism is clinically and biochemically assessed, diagnostic confirmation of GD is possible by testing thyroid-stimulating hormone (TSH) receptor (TSHR) autoantibodies (TRAbs). TRAbs are pathognomonic, correlate with the severity of disease and are present in the serum of approximately 98% of patients with untreated GD. 3 Moreover, TRAb investigation is mandatory in pregnant women previously diagnosed with GD and to predict the disease remission after undergoing a treatment of thyreostatic drugs. 4
Three different kinds of TRAbs have been distinguished: apoptotic (A-TRAbs), blocking (B-TRAbs) and stimulating (S-TRAbs) autoantibodies. 5 Indeed, TRAb assay is complex due to such heterogeneity, and also because of its low serum concentration and the scant knowledge of TSHR immunodominant epitopes.
To date, the methods available for TRAbs testing are based on immunoassays (IMAs) or bioassays (BAs). While IMAs allow to measure only the bond of autoantibodies to the receptor, through BAs it is also possible to discern their functionality and thus single out S-TRAbs and B-TRAbs. Nevertheless, even though TRAbs measured with BAs are highly correlated with GD activity, their use in clinical practice remains restricted to a limited number of specialized laboratories. 6 On the contrary, the third generation of IMAs in a competitive format is suitable in clinical practice and shows high analytical and clinical sensitivity, in addition to providing a good clinical specificity. However, these methods do not allow to distinguish different kinds of TRAbs that are found in patients diagnosed with autoimmune thyroid disease.7,8
In the last year, Siemens has marketed the first IMA method which is supposed to test only the serum concentration of S-TRAbs: the Immulite™ thyroid-stimulating immunoglobulins (TSI) assay. This new quantitative assay is available in an automated commercial platform/instrument (Immulite 2000) and employs a different technology, as it is an assay in a non-competitive sandwich format. 9 The method ideally represents the synthesis of innovations introduced by the third generation of IMAs as well as those led by the latest BAs which employ the chimera receptor. 10 Moreover, its diagnostic performance in GD patients seems promising and suggests a future possibility to include the assay in diagnostic algorithms. 11
The aim of our work was to evaluate the analytical performance and the clinical reliability of the TSI assay. We tested serum samples of patients with thyroid diseases (both autoimmune and non-autoimmune) treated in our hospital in the last year. The Siemens method was compared with Elecsys/Cobas Anti-TSH Receptor electro-chemiluminescence IMA. We also suggested a possible cut-off value in order to correctly distinguish GD from other thyroid pathologies.
Material and methods
Patients
We evaluated the serum samples of 95 consecutive patients (56 females and 39 males) and 50 healthy subjects (HS) (30 females and 20 males) throughout one year.
Among enrolled patients, 10 presented with multinodular non-toxic goiter (MNTG) (6 females and 4 males), 39 with thyroiditis (24 females and 15 males) divided into 36 chronic autoimmune thyroiditis (CAT) and 3 atrophic thyroiditis (AT), and 46 with untreated GD (26 females and 20 males).
All subjects underwent complete physical examination and endocrinological evaluation with thyroid echo-colour Doppler and biochemical testing of thyroid profile: TSH, free thyroxine (FT4), thyroperoxidase antibodies (TPOAb) and thyroglobulin antibodies (TgAb) on chemiluminescent assays (Centaur XL, Siemens Healthcare Diagnostics). Untreated GD patients were diagnosed according to the American Thyroid Association and American Association of Clinical Endocrinology Guidelines. 12 HS were blood donors in ‘Francesco Olgiati’ Association in Gemelli Hospital. They were < 30 years old with a TSH concentration within the reference range and normal thyroid ultrasound. They did not show autoimmune and non-autoimmune thyroid disease, nor other autoimmune disease. 13 All subjects gave informed consent to take part in the study.
Samples treatment
Blood was drawn by venipuncture into two serum tubes according to WHO Guidelines 14 and centrifuged at 4500 r/min for 5 min at room temperature. The two serum samples were employed as follows: the first aliquot was immediately used to test TSH, FT4, TPOAb and TgAb; the second was frozen at −20℃, thawed at the time of testing and briefly mixed before assaying TRAbs.
Immulite™ TSI assay
The Immulite TSI assay (Siemens Healthcare, Llanberis, UK) is an automated sandwich chemiluminescent IMA in which a pair of recombinant human TSHR is used in a bridging format. In this manner, it provides a bridge link between TRAbs and the two receptors (capture and signal antibodies) as described in literature.9,10
The real innovation of the assay is the capture receptor which is characterized by a TSHR chimera in which the binding region for B-TRAbs (261–370 aa) is replaced with a tract (261–329 aa) of the rat luteinizing hormone/chorionic gonadotropin receptor (LH/CG). This means that the capture chimera receptor has epitopes which should be recognized only by S-TRAbs. During incubation, S-TRAb binds such receptor with one arm and the signal receptor with the other arm. A sandwich complex is generated, and TRAbs concentrations are quantified by the secretory alkaline phosphatase (SEAP) activity on a luminescent substrate. Hence, the amount of analyte is directly correlated to the obtained chemiluminescent signal.
Cut-off value suggested by the manufacturer is 0.55 IU/L. The assay is calibrated by using the WHO 2nd International Standard (IS) for thyroid-stimulating antibodies (NIBSC 08/204).
S-TRAb determinations were performed in four analytical runs, following the manufacturer’s instructions.
Analytical and clinical evaluation
Analytical performance of the Immulite™ TSI Assay was evaluated according to CLSI EP17-A protocol 15 for limit of blank (LoB), limit of detection (LoD) and limit of quantification (LoQ) determinations. The evaluation of test reproducibility was performed by following the CLSI EP5-A2 protocol. 16 LoB was obtained by testing a physiological solution for 20 times, whereas LoD and LoQ were quantified by testing a pool of serum samples with very low TRAb concentration (0.07–0.30 UI/L).
Imprecision profile estimation was obtained by analysing two serum samples pool: the first with a low concentration and the second with a high concentration of TRAbs. Both concentrations fall into a work range of 0.25–8.50 UI/L. The intra-assay precision was conducted by repeating TRAb testing 20 times in the same run on the two serum samples pools. The inter-assay precision was run by testing the analyte on the two serum samples pools 20 times in different days. The obtained precision was expressed as coefficient of variation (CV) and reported as percentage (%).
Diagnostic performance was assessed by receiver operating characteristics (ROC) 17 curve analysis in order to distinguish untreated DG patients from HS and other thyroid diseases. We selected the best cut-off value with the highest diagnostic sensitivity and specificity.
Method comparison with Elecsys/Cobas IMA
The Immulite TSI assay was compared with Elecsys/Cobas Anti-TSH Receptor electro-chemiluminescent IMA (Roche Diagnostics, Mannheim, Germany) on Cobas E 8000 platform. Such assay seizes on the competition for the bond to TSHR between the TRAbs and the Fab fragments of the ruthemium-labelled antibodies. Thus, TRAb measurement takes place indirectly by means of the quantification of the bound antibody.
Cut-off value suggested by the manufacturer is 1.75 IU/L. The assay is calibrated by using the 1st IS (NIBSC 90/672).
The comparison study was carried out in a single run on both instruments according to the manufacturer’s instructions. Before each run, quality control was performed by checking if the manufacturer’s controls fall within the expected range.
Statistics
Data were analysed by using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA). The normality distribution of results was assessed by using Shapiro Wilk test. Kruskal-Wallis test was used to compare GD TRAb values to those obtained by testing the other groups of patients. A P-value < 0.05 was considered as significant. Data were expressed as mean (standard deviation).
For comparison study, the Roche/Elecsys method, routinely used in our laboratory, was considered as reference method. Data lower than the LoQ were considered as the LoQ value for statistical analysis.
ROC curve was plotted and analysed to select the best cut-off with the highest clinical sensitivity and specificity. Agreement and correlation between the two assays were obtained by Bland Altman and Passing and Bablok regression analysis. 18
Results
Characteristics of patients and TRAb testing
Classification, clinical characteristics and analytical results for each group enrolled in the study.
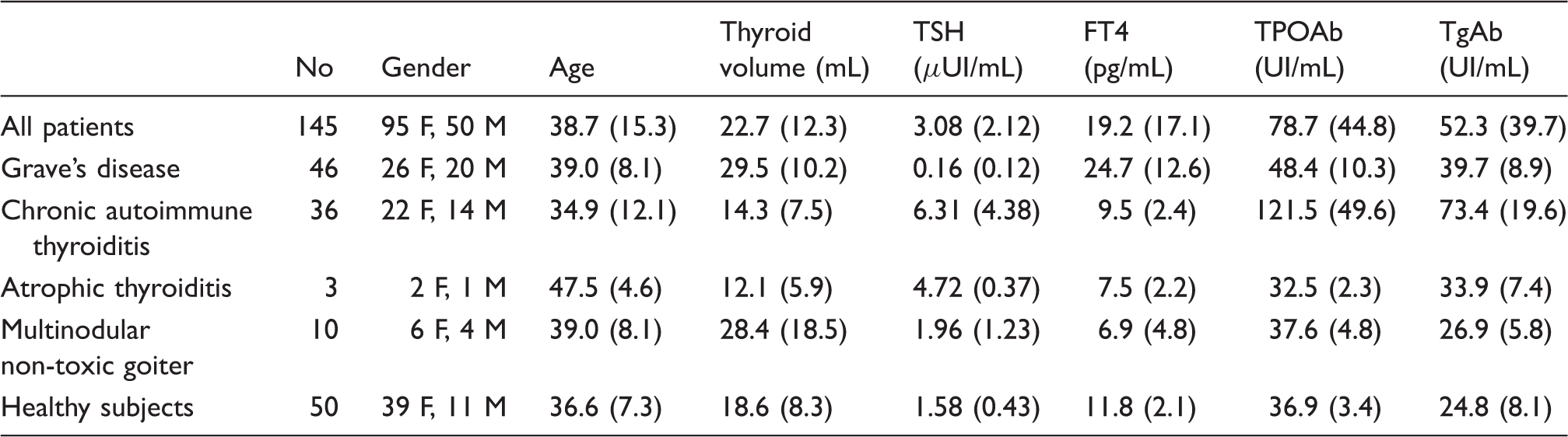
Note: All results are reported as mean (standard deviation).
TSH: Thyroid-stimulating hormone; FT4: free thyroxine; TPOAb: thyroperoxidase antibodies; TgAb: thyroglobulin antibodies.
Analytical and clinical evaluation
Analytical evaluation of Immulite TSI IMA, comparing experimental results with those declared by the manufacturer.
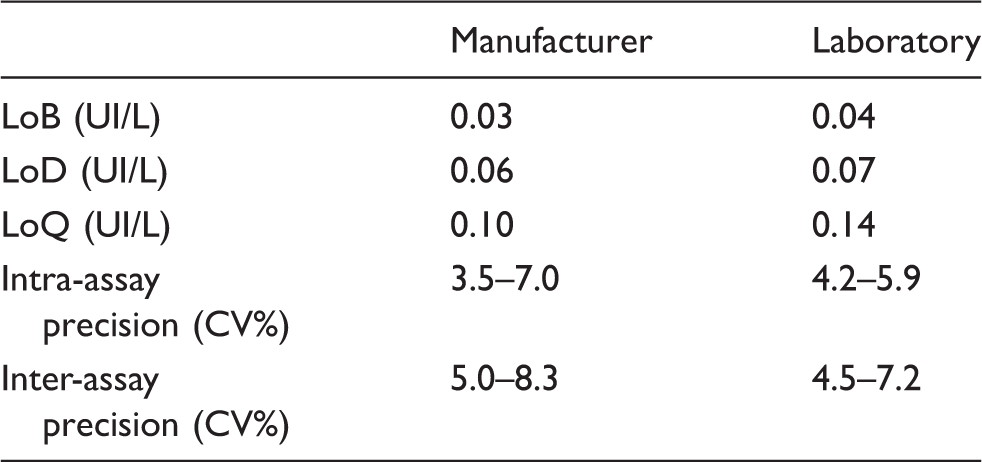
LoB: limit of blank; LoD: limit of detection; LoQ: limit of quantification.
Figure 1 shows the ROC curve analysis in order to diagnose GD, comparing these patients with other thyroid diseases and HS. The area under the curve (AUC) was 0.985. We selected a value of 0.57 UI/L as the best cut-off to discriminate patients with untreated GD (98.0% of sensitivity, 99.9% of specificity). By using this cut-off, we observed only three discordant cases between clinical characteristics and laboratory results in our population (in detail, two false-positive values and one false-negative value).
ROC curve analysis in order to diagnose GD. The area under the curve (AUC) was 0.985. 0.57 UI/L was the best cut-off value (98.0% of sensitivity, 99.9% of specificity).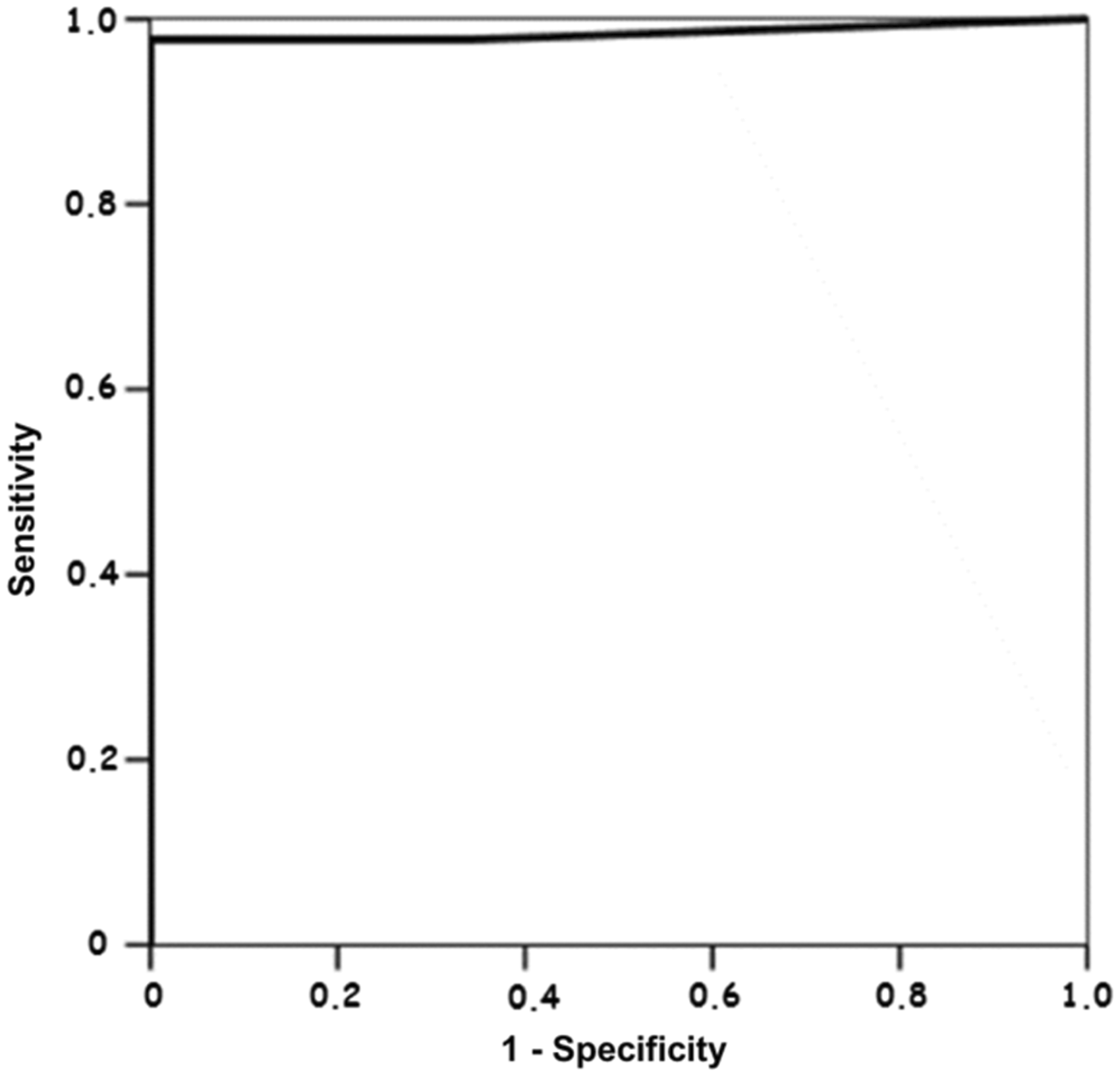
Comparison study
Passing–Bablok regression showed a good correlation between the two methods (Figure 2). The intercept was −1.29 UI/L (95% confidence interval [CI] between −0.26 and −2.12 UI/L), while the slope was 1.03 (95% CI between 0.90 and 1.06). The regression coefficient (R2) was 0.98.
Passing–Bablok regression between the Siemens and Roche methods. Brackets represent the 95% confidence interval (CI). The regression coefficient (R2) was 0.98.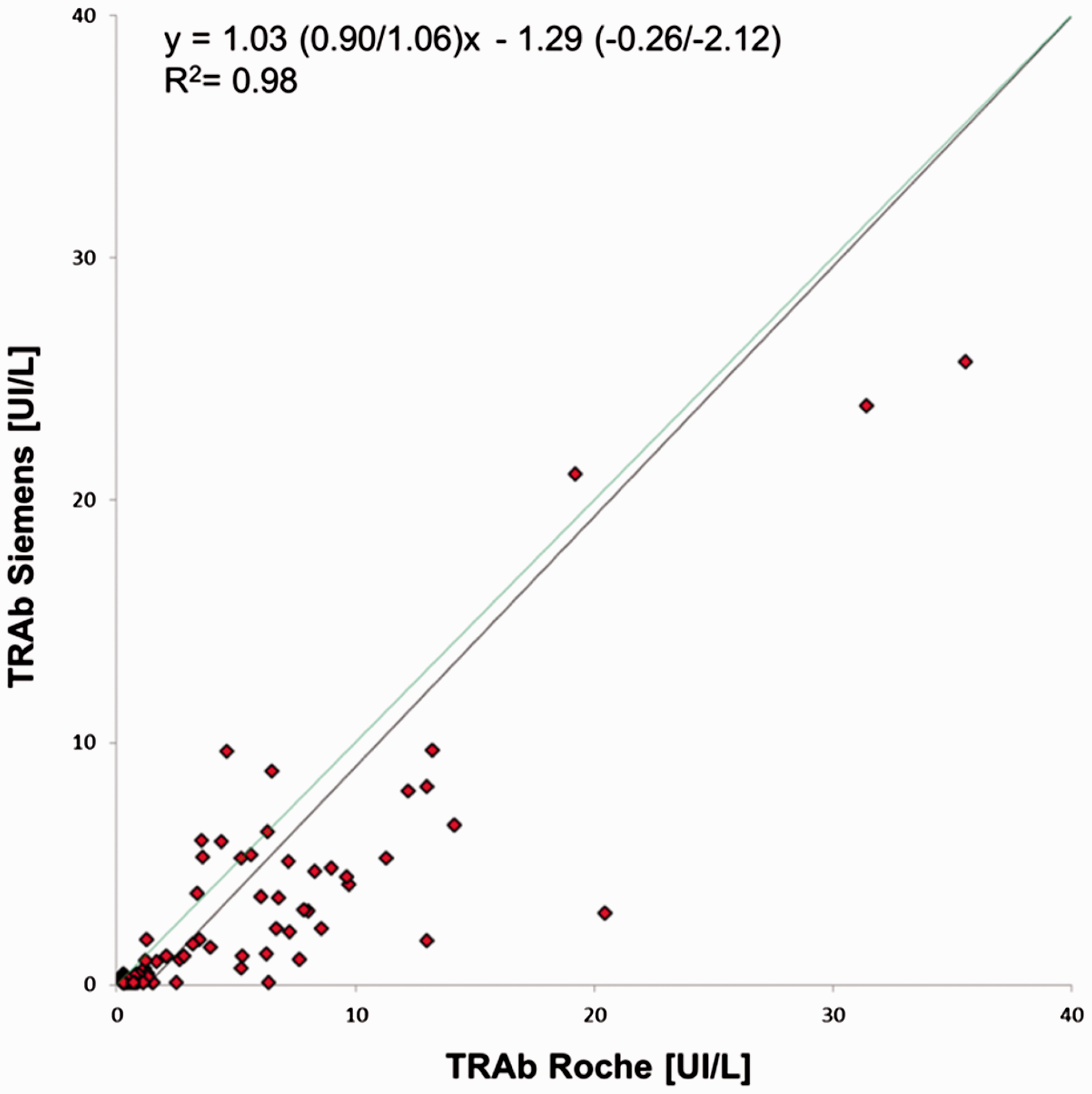
Bland Altman analysis pointed out a bias of −2.70 UI/L (95% CI between 6.28 and −11.68 UI/L) which did not concern TRAb concentrations, but the different technologies used for the comparison study (Figure 3).
Bland Altman analysis of the Siemens and Roche methods. The bias was −2.70 UI/L (95% CI between 6.28 and −11.68 UI/L).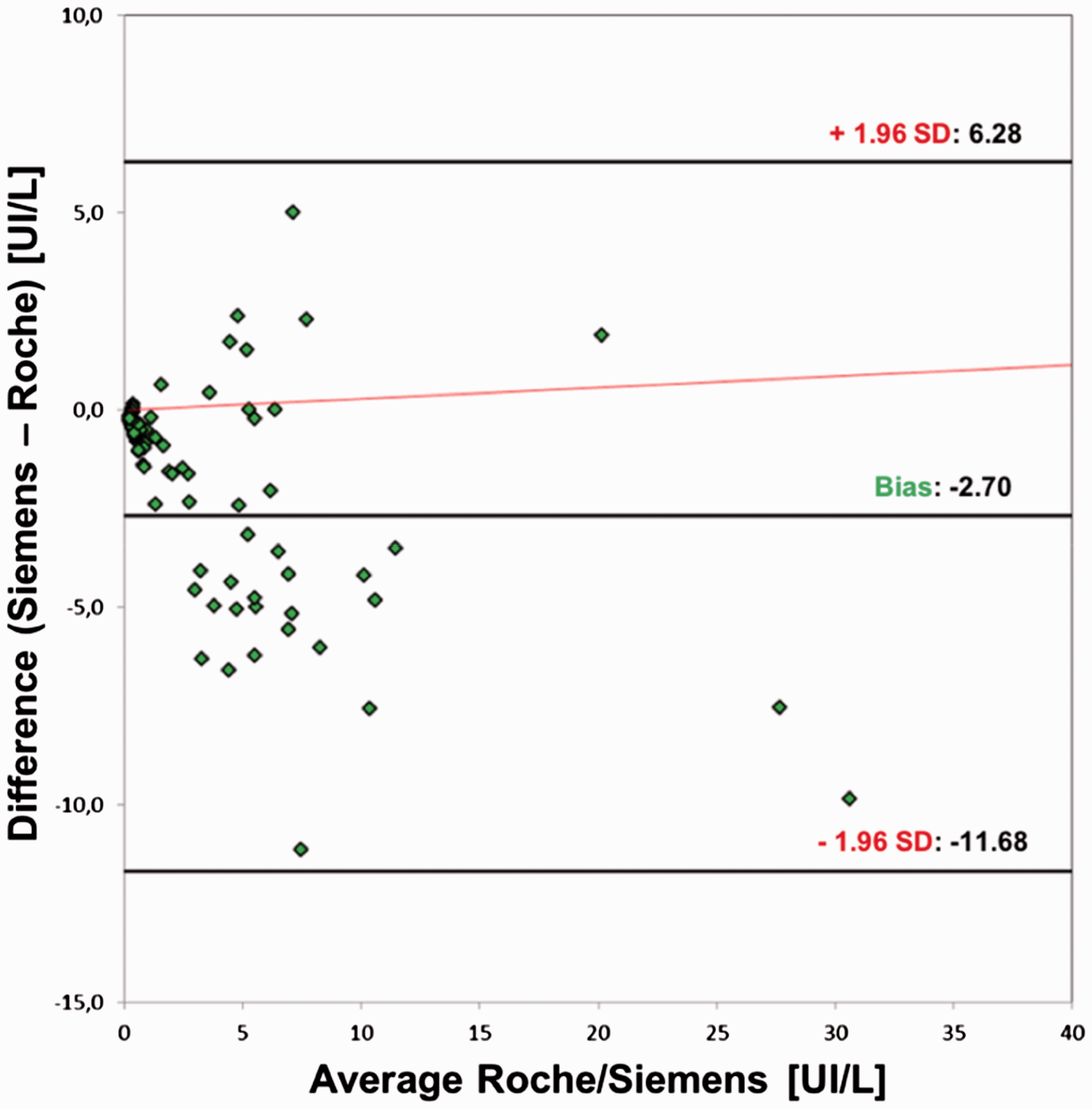
Discussion
We evaluated an automated IMA method which selectively detects S-TRAbs. The study was conducted in order to confirm the high analytical and clinical performance declared by the manufacturer and published recently.9,11 The technology of Immulite TSI IMA is an absolute innovation: the method is based on a sandwich format, completely different from the classical competitive third generation assays used until now to test TRAbs. The specific measurement of S-TRAbs is possible due to a capture receptor which maintains only the binding sites for these autoantibodies at N-terminus of TSHR. 19 Indeed, most TRAbs recognize linear and conformational epitopes in other domains of TSHR.5,11 In addition, the Immulite TSI IMA is calibrated against the second IS (NIBSC 08/240), which refers to the detection of S-TRAbs, different from the first IS (NIBSC 90/672) used by the other TRAb IMAs, which refers to all antibodies.11,20
If we observe the analytical performance in our series (Table 2), the precision values and the analytical sensitivity are completely comparable to those declared by the manufacturer. Moreover, by ROC curve analysis, we chose 0.57 UI/L as the best cut-off to diagnose GD. Such value is very close to that proposed by the manufacturer (0.55 IU/L) and obtained by the authors of two recent papers (0.55 and 0.54, respectively).9,11
By using a cut-off of 0.57 UI/L, the method could distinguish clinical characteristics of all enrolled patients, apart from one false-negative and two false-positive cases. In detail, the false-negative is a value of 0.10 UI/L in a patient with a diagnosis of mild hyperthyroidism, whereas the two positive values (1.69 UI/L and 1.03 UI/L) were observed in two patients with CAT and MNTG, respectively. However, an S-TRAb positivity in CAT serum is consistent with the evidences already described in literature. 21 We also investigated a possible origin of S-TRAb concentration in the sample of the patient with MNTG. In such serum, we observed an antinuclear antibodies’ positivity which may explain an assay positivity linked to the real presence of S-TRAbs in this patient. It is well known that thyroid antibodies are frequently associated with autoimmune disease characterized by a larger number of antibodies as systemic lupus erythematosus. 22
The comparison study pointed out a good correlation (R2 = 0.98, slope = 1.03) and a minimum bias even if the agreement between the two methods were not significant (intercept 95% CI = −0.26/−2.12 UI/L). This result is not surprising: we compared a non-competitive IMA method with a competitive IMA characterized by different epitopes. Moreover, the cut-off value is lower (0.57 UI/L vs. 1.75 UI/L), whereas the analytical sensitivity (LoQ = 0.14 vs. 0.9 UI/L) is higher for the Siemens method, as it reduces the decision cut-off (0.57 UI/L vs. 1.75 UI/L) to diagnose GD.
By using the cut-off value of Roche/Elecsys method, we obtained more clinically discordant test results: three false-negatives which were borderline to the cut-off value (1.17 UI/L, 1.23 UI/L, 1.67 UI/L) and four CAT false-positives. However, these CAT patients could be developing B-TRAbs which, when present in circulation, can cause glandular atrophy associated with AT. We enrolled AT patients exactly with this aim, but unfortunately we got only few cases and all of them negative for TRAbs.
The diagnostic sensitivity and specificity (98.0% and 99.9% respectively) of Immulite TSI IMA were higher than those declared by Roche/Elecsys method (96.0% and 99.0% respectively). The higher diagnostic performance could be explained by the innovative technology used which allows to measure S-TRAbs through a double epitope recognition.
To conclude, the data obtained through Immulite TSI method present very promising analytical and diagnostic characteristics, which confirm what has been proved in literature. 11
The diagnostic performance in GD patients is comparable to, if not better than, that of current TRAb assays. For this reason, such method can be adopted in clinical practice for the differential diagnosis of hyperthyroidism and also to screen neonatal transient hyperthyroidism.
In addition to this, the test allows to accurately detect very low values of analyte, apart from identifying GD patients correctly. The highest analytical sensitivity that has emerged could make this method the elective one during the monitoring of GD patients after the interruption of thyreostatic therapy. In this way, such technology would be the only one that could be useful in detecting earlier possible relapses. Future studies will have to confirm and clarify this aspect.
Furthermore, our results did not underline the specificity of Immulite TSI IMA test for the S-TRAbs only. Further studies are needed also to prove such characteristic, by comparing this assay with BAs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
We performed a retrospective cohort study without the need of an ethical approval.
Guarantor
CC.
Contributorship
CA and RM performed all experiments and wrote the first draft of manuscript. LP was involved in protocol development and clinical setting. PA and ZC performed data analysis. CC supervised all experiments and contributed to the project idea. All authors reviewed and edited the manuscript and approved the final version of the manuscript.