
Abstract
Background
Microscopic examination of samples with negative dipstick results is not necessary. The aims of this study were to: (i) assess the risk of excluding urine sediment examination with negative dipstick results and (ii) calculate time savings by introducing this process.
Methods
The risk analysis was done for samples with negative urine dipstick and positive sediment findings. Possible missed elements in sediment were defined as 21 errors. Time saving was calculated as average time for preparation and examination sediments. Data were presented as counts and percentages.
Results
Out of 2997 samples, negative dipstick results were reported for 926 (30.6%) samples, out of which, microscopic examinations were positive for 527 (17.6%) samples. 18/21 errors were detected, with missing <5 squamous epithelial cells (SQEC) and bacteria 1+ as the most frequent ones (22.7% and 22.4%, respectively). Errors with the intermediate risk for patients were missing to report: ≥5 SQEC, ≥5 transitional epithelial cells, ≥10 hyaline casts (11.9%, 0.21%, 0.32%, respectively). Errors associated with high risk were not detected. Estimated total time saving is more than 25 h/month.
Conclusions
Microscopic examination of urine samples with negative dipstick results can be excluded without risk for patients and can result with considerable time savings.
Introduction
Urinalysis is composed of physical, chemical and microscopic examination of urine. Urinalysis is very common in diagnosis of renal diseases and urinary tract infections (UTIs) as a screening test, but it is not recommended in asymptomatic patients. Microscopic examination of urine sediment should be performed only if results for physical and chemical examination are abnormal, if microscopy is requested by the physician or in special occasions defined by each laboratory. 1 According to the European urinalysis guidelines, it is not necessary to examine urine samples microscopically if visual examination has normal results (bright yellow and clear urine) and chemical examination is negative on urine dipstick test for proteins, leukocyte esterase, haemoglobin and nitrite. 2
Even though, according to guidelines, microscopic examination is not necessary for normal and negative chemical test results, several factors can cause false-negative results and consequently some potentially harmful state can be missed. False-negative urine dipstick results could be caused by the vitamin C intake or dilution of urine samples. 3 In spite of that, negative chemical test results have very high negative predictive values for leukocyte esterase and/or nitrite, glucose and haemoglobin (from 70% to even 100%), which is an evidence that it is not necessary to examine sediment microscopically.4,5 The most of the previously published papers deal with false-positive results. The meta-analysis of Devillé et al. has shown that urine chemical test could be used for exclusion of infection in patients with negative nitrite and leukocyte esterase test. On the other hand, positive results of one or both above mentioned test have to be confirmed with gold standard microbiological urine culture, for diagnosis of UTI. 6
In the University Department of Chemistry of Medical School University Hospital Sestre Milosrdnice, it is still practice to microscopically examine all urine sediments regardless of results of physical and chemical examination, in order not to miss any potentially pathological element in the sediment. This practice is time consuming for laboratory personnel and can prolong turn-around time. We hypothesize that exclusion of microscopic examination of negative dipstick urine samples would not harm patients or change their management, diagnosis or treatment.
Therefore, the objectives of this study were to: (i) assess the risk for the patients and (ii) calculate the laboratory personnel time savings associated with exclusion of microscopic examination for samples with negative urine dipstick results.
Materials and methods
Study design
All urine samples with requested urinalysis in September 2015 were included in this retrospective study. Data on urinalysis results and requesting departments were collected from the laboratory information system (LIS) of University Department of Clinical Chemistry in Medical School University Hospital Sestre Milosrdnice, Zagreb, Croatia.
Methods
Physical, chemical and microscopic examination of urine samples were performed by experienced laboratory personnel. Urine samples were delivered in the laboratory in urine cups or tubes (Greiner Bio-One GmbH, Kremsmünster, Austria). Combur-10 Test® strips (Roche Diagnostics, GmbH, Mannheim, Germany) were used for chemical examination of urine. Urine analyzers Cobas u411 and Miditron Junior II (both Roche Diagnostics, GmbH, Mannheim, Germany) were used as semi-automated urinalysis system for test strips scanning. Tests were performed as described in manufacturer’s instruction.
For sediment preparation, 10 mL of urine was centrifuged at 500 × g for 10 min on Hettich Rotofix 32 A benchtop centrifuge (Hettich Lab Technology, Beverly, United States). After discarding supernatant, the sediment was resuspended in 500 µL of urine, dropped on glass slide and covered by coverslip. All microscopic examinations were performed by the bright-field microscopy on native urine sediment. Firstly, examination was done under lower magnification of 100 × and fields were scanned for casts. Afterwards, 400 × magnification was used for examination of other elements in urine on 10 random fields.
Risk analysis
Cut-off values for inclusion of samples in risk analysis.
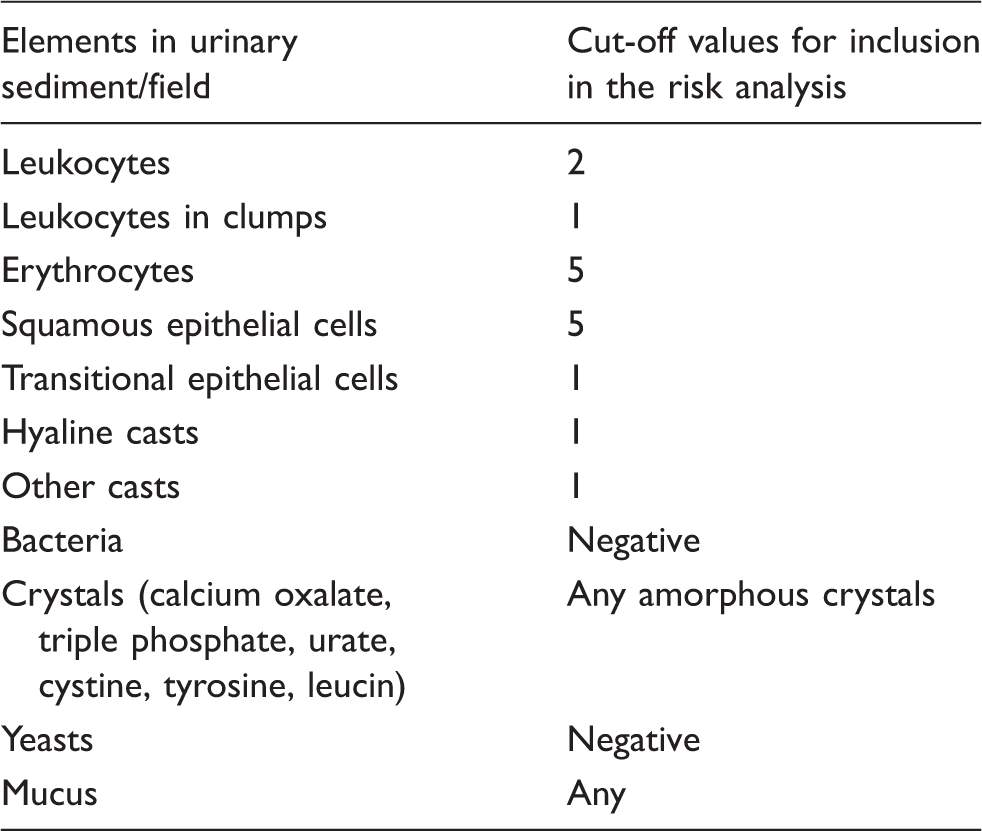
Based on our extensive literature research, there was no universally defined code and error system for classification of microscopy examination errors. Therefore, in order to be able to quantify our results, we have developed our own scoring system according to the clinical relevance of the specific sediment parameter.
Initially, each author provided their own list of errors. The results were then compared and where differences were observed, reevaluation was done. At the end, the list of errors was approved and agreed on by both authors.
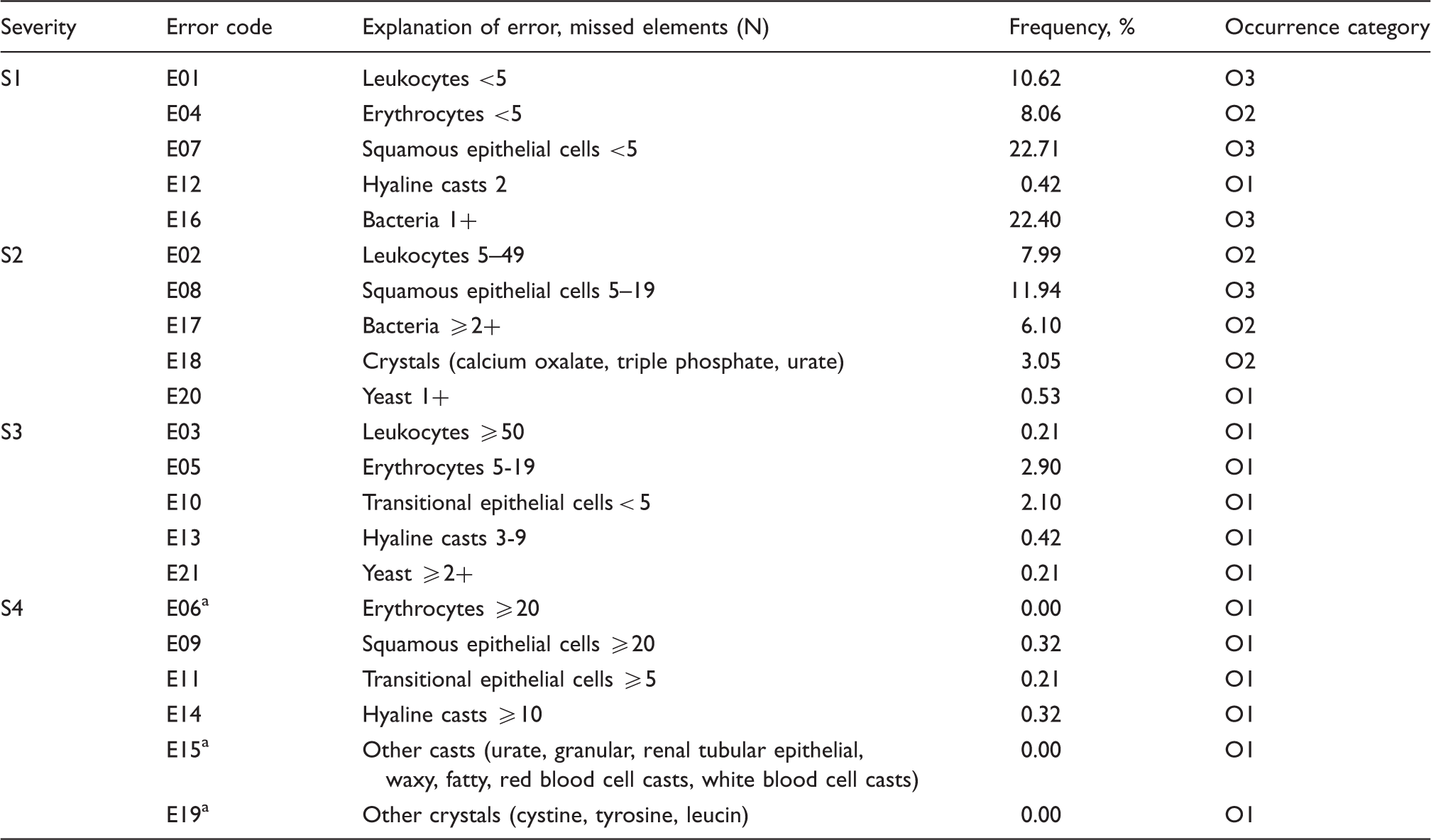
For the risk analysis, 21 potential errors have been identified. Each error was defined as possible missed elements in sediment of negative dipstick urine results on a semi-quantitative scale. Errors from E01 to E03 refer to the missed leukocytes, E04–E06 to the number of erythrocytes, E07–E09 to squamous epithelial cells, E10–E11 to transitional epithelial cells, E12–E15 to casts, E16–E17 to bacteria, E18–E19 to crystals and E20–E21 to the possible missed yeasts. Based on the type and number of missed elements, each of these errors corresponded to certain level of potential harm for the patients. Four different categories of severity for the patients were assessed by the consensus opinion of both authors regarding the clinical significance of elements in urine sediment. The lowest severity level (S1) was defined as minimal harm for patients caused probably by contamination of sample; S2 was defined as necessity for repeated sampling without additional harm for the patient; S3 level as delayed therapy due to missed elements in the urine sediment. Level S4 was defined as the most severe error which corresponds to wrong diagnosis and possible life-threatening state.
Occurrence (O) was classified into five categories according to the observed frequency of each error. O1 category corresponds to the lowest frequency of missed elements (<3%), O2 to the frequency of 3–10%, O3 to >10–25%, O4 to >25–50% and the category of the highest frequency (>50%) of errors was defined as O5.
Risk analysis was done on the basis of ISO 14917 Medical Devices – Application of Risk Management to Medical Devices, 7 by combining the severity (harm) for the patients (S) and probability of errors occurrence (O) in 4 × 5 matrix. Matrix was divided into three types of coloured fields: green, yellow and red. Errors in green area were considered as low risk and in yellow area as intermediate risk for patients. Red area in matrix was considered to be the most hazardous for patients. In our study, errors in red area with the highest risk were considered unacceptable.
Time saving
Total average time for urine sediment examination was calculated according to the following formula

Time saving was calculated as a sum of total average time for urine sediment examination and average time for sediment preparation.
Urine examinations for time saving calculation were done by one experienced laboratory technician. Measurements were done using the stopwatch.
Statistical analysis
Data were presented as count and percentages. Analysis was done in Microsoft Excel (version 2010, Microsoft, USA).
Results
In the studied period (September 2015), 2997 samples with urinalysis requests were admitted to the laboratory. Negative physical and chemical examination results were reported for 926 (30.6%) samples. For 199 (6.6%) Emergency Medicine Department samples with negative dipstick results, urine sediment was not done due to the previous agreement with the Department. Microscopic examination of urine sediment was below predefined cut-off values for 200 (6.7%) samples and those samples were not included in the analysis. For 527 (17.6%) samples, the results of microscopic examination were above cut-off values and risk for patients was assessed for those samples (Figure 1).
Flowchart of urine samples included into risk analysis. Samples included in the risk analysis are marked in red box, samples excluded from the analysis in grey boxes.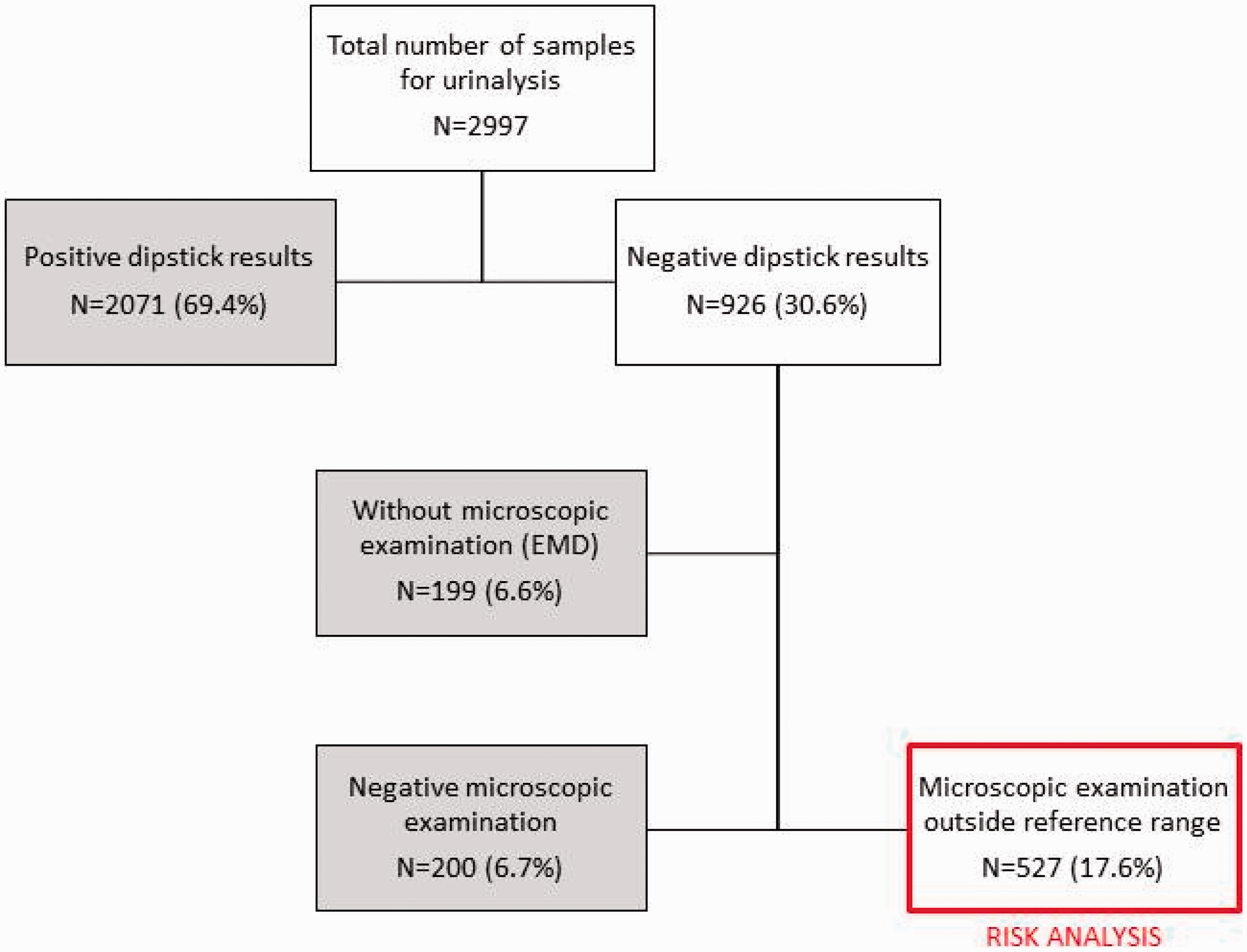
Error codes and explanations for possible missed sediment elements in unexamined negative urine with corresponding categories for occurrence according to the assessed severity.
Errors not found and not included in the risk-occurrence table.
Risk-occurrence table with combination of severity and occurrence of error (N = 18).
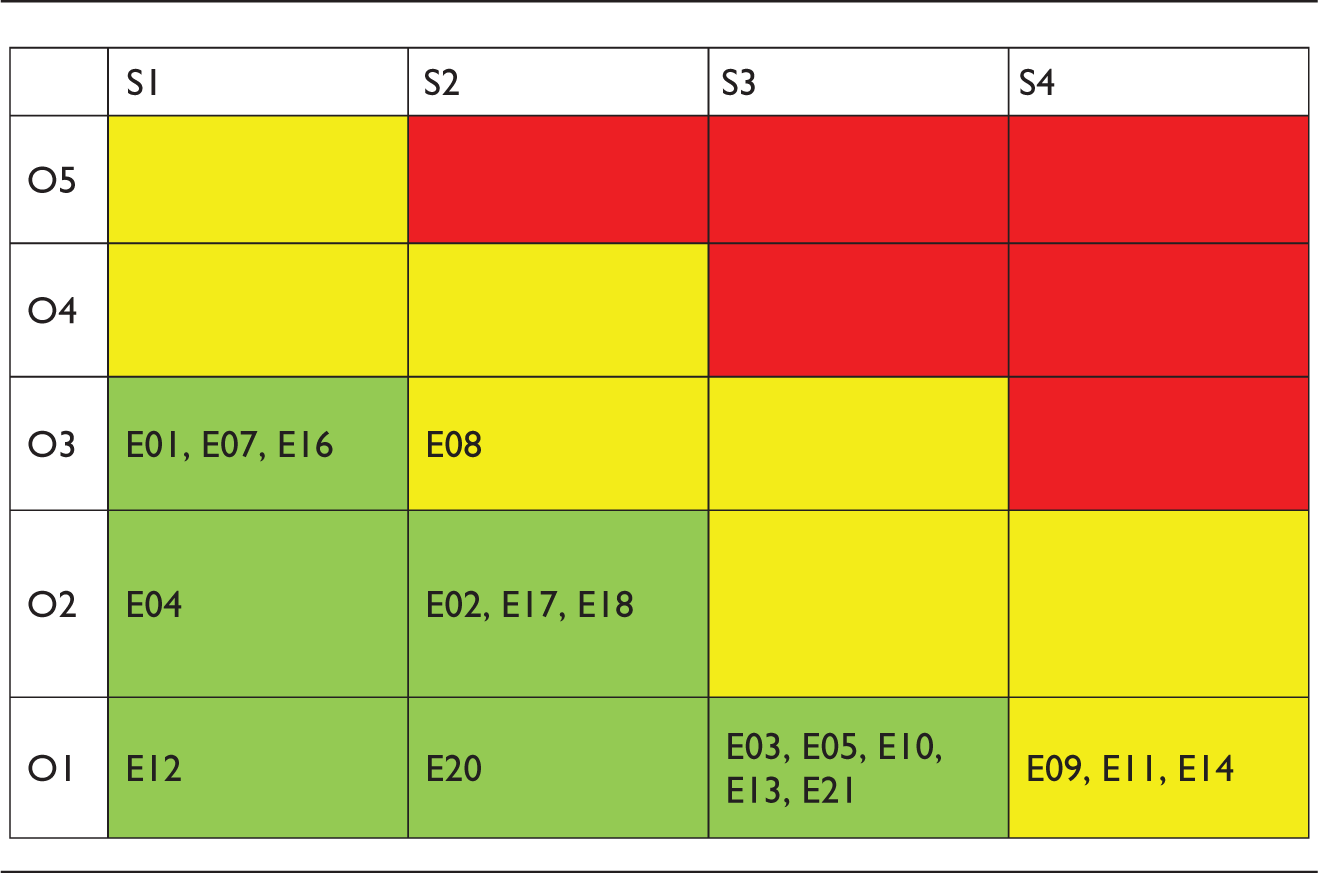
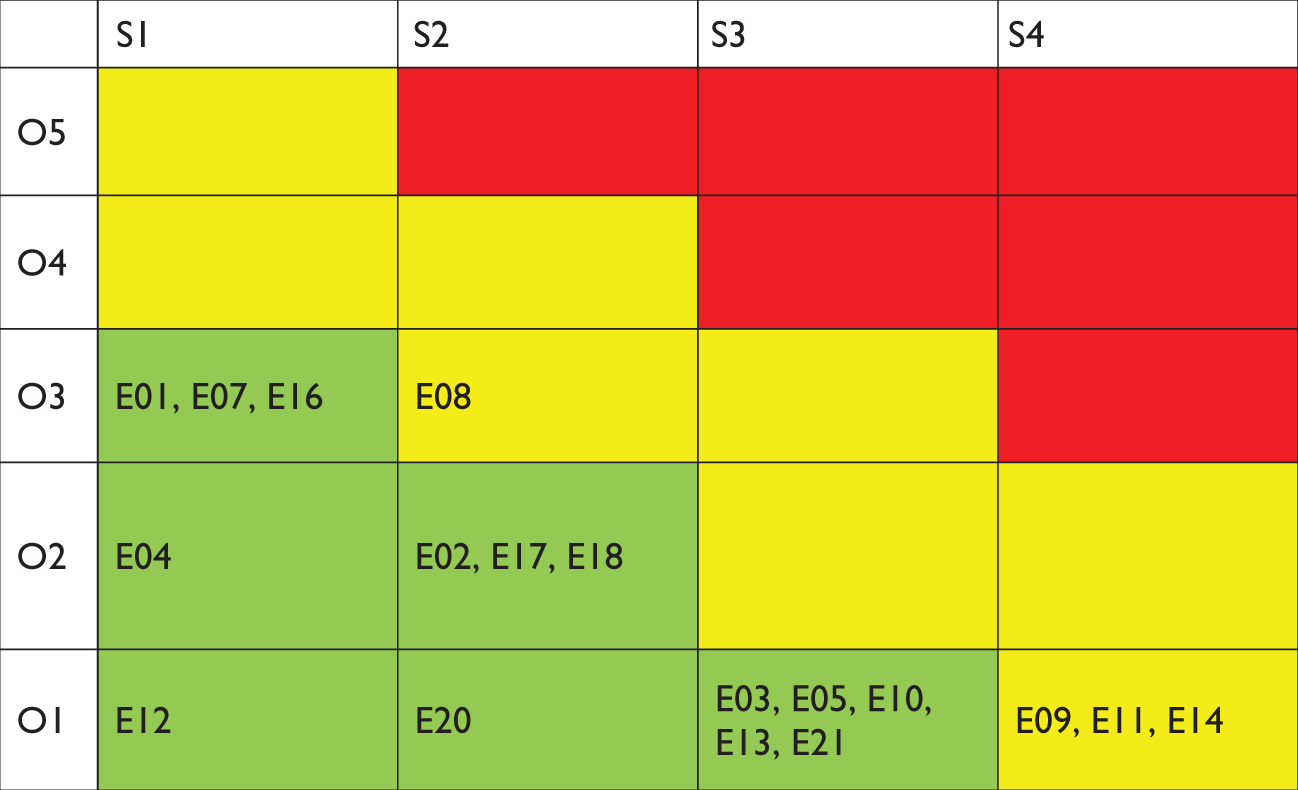
E: error; O: occurrence; S: severity.
The most frequent errors found in urine sediment were missing <5 squamous epithelial cells (O3 = 22.71%) and bacteria 1+ (O3 = 22.4%). Only four errors with the intermediate risk (yellow field of the matrix) were recorded. Out of errors with intermediate risk, three were due to severity level S4 (missing to report ≥20 squamous epithelial cells, ≥5 transitional epithelial cells and ≥10 hyaline casts with frequencies less than 1% (0.32, 0.21% and 0.32%, respectively) and one error (missing to report 5–19 squamous cells) was due to highest combination of occurrence (O3) and severity (S2). Risk analysis did not identify errors in the red field of 4 × 5 matrix.
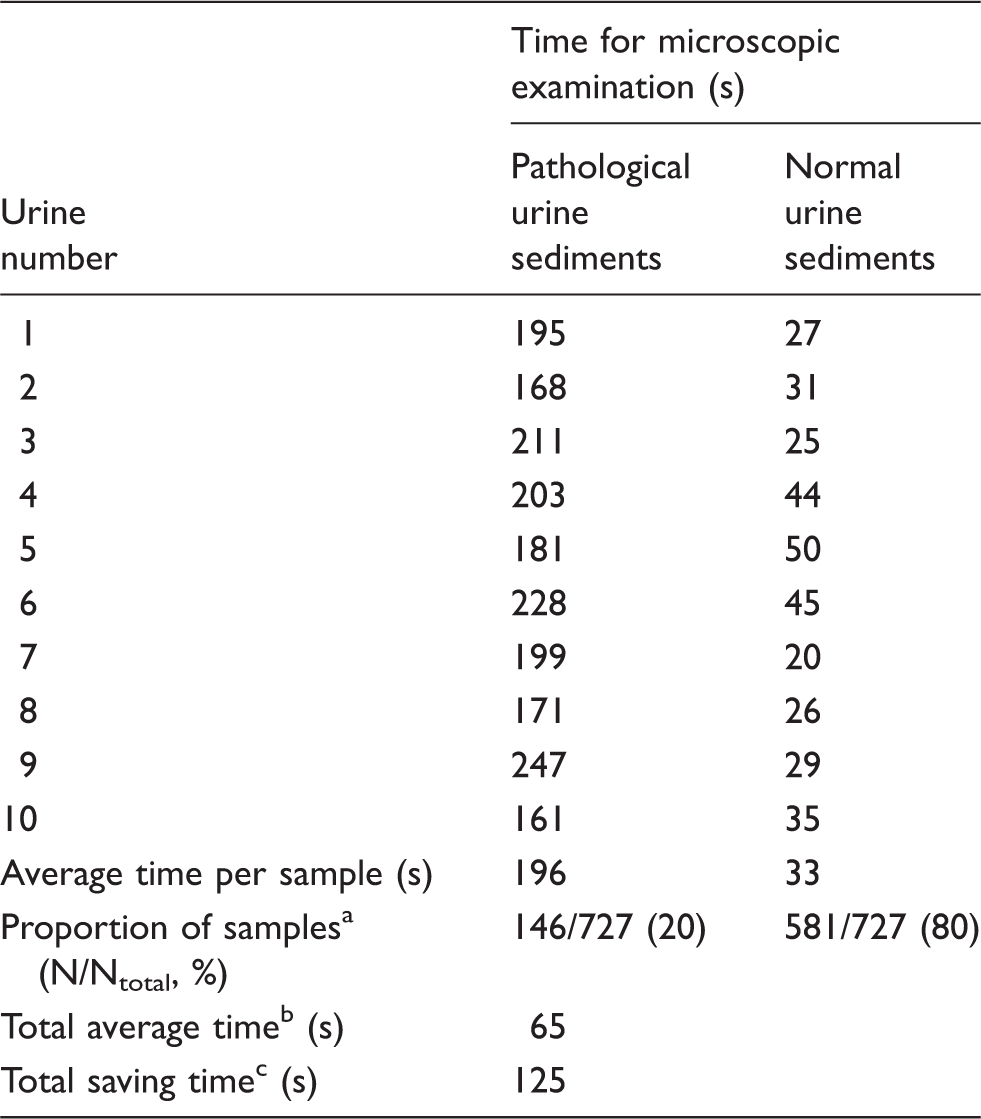
Measured time for microscopic examination of 10 pathological and normal urine samples with calculation of total average time for examination and total saving time (in s).
Distribution of samples with pathological and normal sediment results in the studied period.
Total average time for sediment examination was calculated according to the formula: Taverage = ((Npathological × Tpathological) + (Nnormal × Tnormal))/Ntotal.
Time saving was calculated as sum of average time for sediment examination and time for sediment preparation.
Discussion
This study confirms that examination of urine sediment can be excluded if urine has negative dipstick test results for proteins, leukocytes, nitrite and haemoglobin. We have proved that patients are not at higher risk if this procedure is followed. Although guidelines for urinalysis exist for a long time (more than 15 years), this kind of risk analysis for patients with negative dipstick results was never done. Additionally, this approach provides saving time for laboratory personnel without interfering with the quality of the reported results or increasing the harm for patient safety.
Errors with the highest frequency were bacteria in trace (1+) and few (less than 5) epithelial squamous cells in the sediment. Although those errors had the highest frequencies, both were not exceeding 23%. Findings of bacteria and epithelial squamous cells are usually associated with improper urine collection or prolonged storage and transportation to the laboratory on temperature higher than allowable. For examination of bacteria and epithelial cells, urine samples are stable for maximum of 3 h. 3 If samples are not transported to the laboratory immediately after collection, commensal bacteria present in urine and urinary tract can grow in samples and false positive results can appear. Moreover, it has been previously published that patients usually do not adhere to instructions for proper urine collection. 8 which could contribute to the contamination of sample. Patients are usually not informed about all preanalytical requirements (adequate container, delayed delivery to the laboratory and proper genital cleaning for spot urine collection). 9 Therefore, the most frequently missed elements are probably the result of inadequate preanalytical procedures and are not associated with the UTI. Accordingly, the severity of those errors was defined as the lowest possible (S1), and patient’s health is certainly not at risk if those elements are not reported.
In our study four errors of intermediate risk for patients were found. Out of those four, only one (5–19 epithelial cells) had frequency around 12% and other three (more than 5 transitional epithelial cells, more than 20 squamous epithelial cells and more than 10 hyaline casts) were defined as errors with the highest severity but were found in only eight samples (with frequency of each less than 0.4%). Hyaline casts found in urine sediment can be associated with urine concentration in after-night sample or may be present after strenuous physical activity. Small number of casts in urine usually has no clinical significance. However, finding of hyaline casts may be associated with some renal diseases and special attention has to be dedicated for such results. Cellular casts composed of erythrocytes, leukocytes or epithelial cells could be associated with glomerular or tubular diseases such as glomerulonephritis and pyelonephritis or even with states of higher risk for patients as acute tubular necrosis and even intoxication with nephrotoxic elements. 10 The importance of hyaline and other casts for the diagnosis of renal diseases is the reason why we have chosen such a rigid categorization of estimated risk for patients.
On the other hand, false-positive epithelial cells in urine sediment may be found commonly, especially in women, even without UTI. 11 UTI diagnosis may be set after positive nitrite on urine dipstick and/or with confirmation of bacterial culture in urine. 12 We may presume that high number of epithelial cells in our study may be related to poor collection technique without previous cleaning of urogenital area. If symptoms of UTI are present in those patients, physicians would probably ask for repeated urinalysis and patients would be treated appropriately.
Haematuria in the urine could have high clinical significance in diagnosing of primary and secondary glomerulonephritis and also some tubulointerstitial kidney diseases or malignant conditions. 4 Haematuria can usually be detected with positive dipstick results, and the most important findings are dysmorphic erythrocytes in urine sediment, which imply that glomerular damage is occurring. Although few guidelines exist for managing the patients with microhaematuria, there is no published study with research of negative chemical test results and positive microscopic examination. The most frequent result for erythrocytes found in our study is less than 5 cells per field (E04), which is still within the normal values. Also, no more than 19 missed erythrocytes per examined field under the bright-field microscope were observed in this study. Therefore, we conclude that the risk that severe haematuria is missed, if sediment examination was excluded, is very low.
According to the ISO 15189 standard, all processes in the laboratory should be evaluated for potential risk for the patient safety. If some of laboratory processes are found to be of high risk for patients, they should be changed immediately in order to reduce harm. 13 The main objective for all laboratory professionals is providing the highest level of patient care, with the lowest error rate and personnel utilization. In order to obtain these goals, laboratory personnel needs to ensure the optimal quality of the preanalytical, analytical and postanalytical phase as well as optimize the entire procedure.14,15 Errors in process could harm, not only patients, but also laboratory personnel, due to unnecessary waste of time for unproductive processes. 16 Therefore, the analysis of risk for the patients combined with the productivity analysis of the work process is the optimum way of gaining the benefit for the laboratory.
In our laboratory, all urine samples were examined microscopically, except for less than 7% of samples received from Emergency Department. Preparation and examination of urine sediments are very time consuming. 17 The average time spent for microscopic examination of negative dipstick urines was around 2 min, but with large number of samples in daily practice, laboratory personnel can save more than three working days per month. Laboratory personnel included in this part of study has a lot of experience in the microscopic examination of urine and calculated time saving may be even higher if we have included more than one laboratory technician in this estimation. However, time saving with the new procedure is not negligible.
This study has few limitations. Since our results were collected retrospectively, we do not have information about the time of sample collection, storage and transportation prior to urinalysis. Information about the first or later stream of urine was also not available. Furthermore, it is not possible to check if samples of studied patients were contaminated with some other interfering substances such as vitamin C. 18
Conclusions
This risk analysis on exclusion of unnecessary sediment microscopy confirmed that the quality of reported results is not compromised; physicians have access to almost the same clinical information, patients are not at risk of diagnostic errors and productivity within laboratory is increased.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval (including reference number)
Not applicable. Study is retrospective, without info on patient data.
Guarantor
MM.
Contributorship
MM and NN researched literature and conceived the study. MM was involved in data collection. MM and NN have done data analysis. MM wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.