
Abstract
Preanalytical errors have previously been shown to contribute a significant proportion of errors in laboratory processes and contribute to a number of patient safety risks. Accreditation against ISO 15189:2012 requires that laboratory Quality Management Systems consider the impact of preanalytical processes in areas such as the identification and control of non-conformances, continual improvement, internal audit and quality indicators. Previous studies have shown that there is a wide variation in the definition, repertoire and collection methods for preanalytical quality indicators. The International Federation of Clinical Chemistry Working Group on Laboratory Errors and Patient Safety has defined a number of quality indicators for the preanalytical stage, and the adoption of harmonized definitions will support interlaboratory comparisons and continual improvement. There are a variety of data collection methods, including audit, manual recording processes, incident reporting mechanisms and laboratory information systems. Quality management processes such as benchmarking, statistical process control, Pareto analysis and failure mode and effect analysis can be used to review data and should be incorporated into clinical governance mechanisms. In this paper, The Association for Clinical Biochemistry and Laboratory Medicine PreAnalytical Specialist Interest Group review the various data collection methods available. Our recommendation is the use of the laboratory information management systems as a recording mechanism for preanalytical errors as this provides the easiest and most standardized mechanism of data capture.
Introduction
Preanalytical errors (PAEs) are errors which occur prior to the analytical stage in the total testing process (TTP) and can occur both before and after receipt of specimens in the laboratory. They have previously been shown to contribute a significant proportion of errors in laboratory processes (up to 68.2%).1–3 PAEs contribute to a number of patient safety risks, including inappropriate or incorrect therapeutic interventions, unnecessary follow-up investigations and diagnostic delays, each of which impact on the clinical and economical effectiveness of pathology services.4–6
Requirements for accreditation against ISO 15189:2012 (Medical laboratories – Requirements for quality and competence) dictate that laboratories should consider preanalytical processes in a number of areas of the quality management system, including the identification and control of non-conformances, continual improvement, internal audit and quality indicators (QIs). 7 It states that ‘the laboratory shall establish QIs to monitor and evaluate performance throughout critical aspects of pre-examination, examination and postexamination processes’. In the UK, a recent report into the quality assurance frameworks and governance systems highlighted variations in the processes for error reporting, advising that high levels of error reporting with low overall error rates is a good indicator of a quality service. 8
In a previous study by the Association for Clinical Biochemistry and Laboratory Medicine Pre-Analytical Specialist Interest Group (ACB-SIG-PA), we have shown that there is a wide variation in the definition, repertoire and collection methods for preanalytical QIs. 9 Here, we aim to review potential methodologies for the monitoring of PAEs, including recording of errors, data collation and review, follow-up data outputs and integration into a clinical governance framework. It is hoped that consideration of data collection methods will help to standardize data, allow development of key performance indicators (KPIs) and support peer review and continual improvement.
Types of PAEs
Mandatory quality indicators of the pre-analytical phase as suggested by IFCC-WG-LEPS.
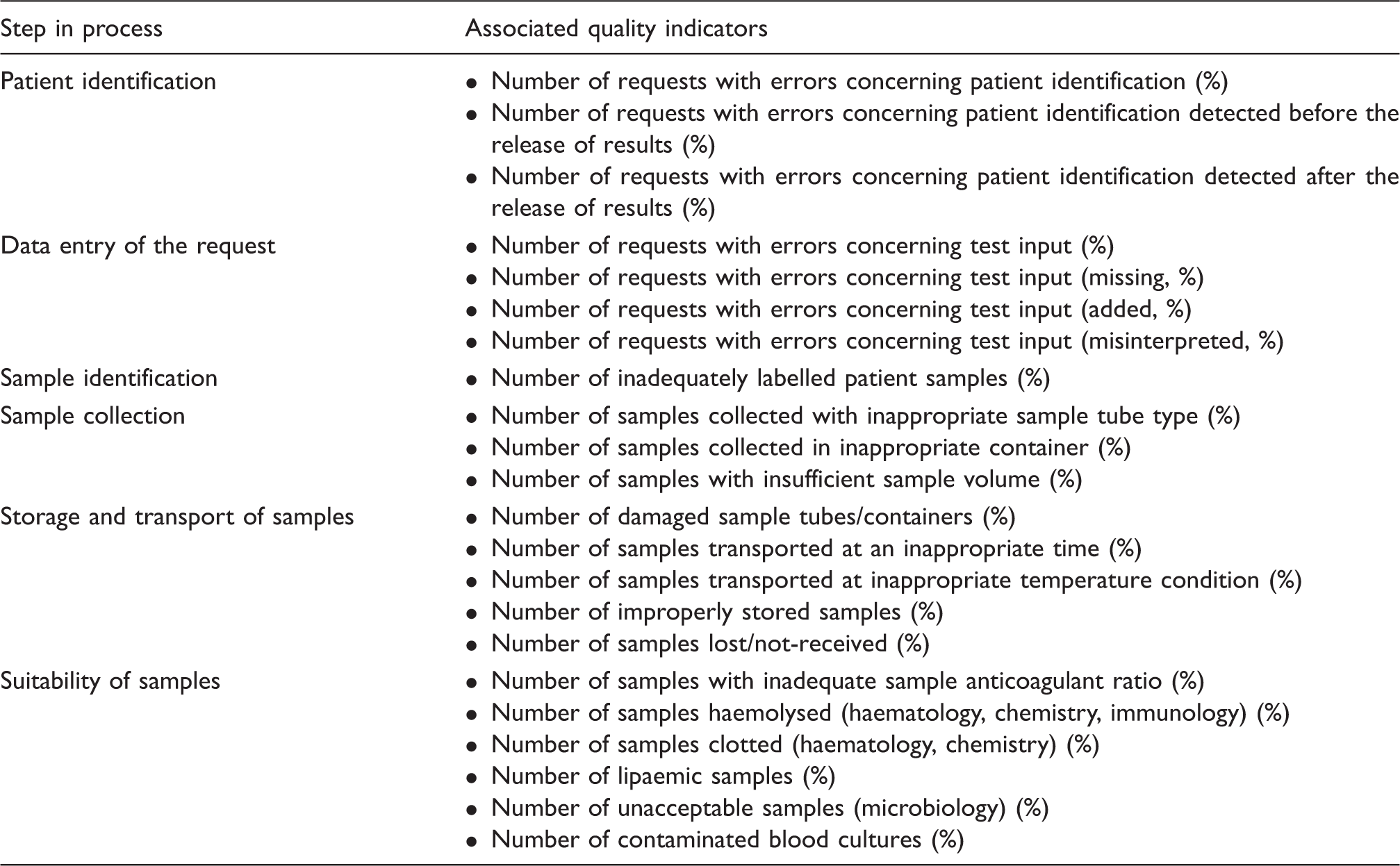
These suggestions outline a number of common areas of the preanalytical laboratory processes where errors can occur, but are not an exhaustive list. Laboratories should consider the risks associated with each step in the TTP for the services they offer, and look to ensure that processes are in place to identify process failures and monitor their rates of incidence. This project has also triggered the development of other country-specific pre- and postanalytical external quality assurance schemes which will further drive the need to standardize collection methods. 12 Further consideration of harmonized definitions of QIs may be required moving forward. For example, the IFCC-WG-LEPS defines the presence of haemolysis in Clinical Chemistry samples as a free haemoglobin concentration of >0.5 g/L, while a variety of laboratory tests are affected by haemolysis at lower and higher concentrations of free haemoglobin and practice regarding the handling of haemolysed specimens may vary between laboratories. Requirements for the labelling of samples will also vary between laboratories, with transfusion laboratories an example where minor errors will result in rejection, and where the IFCC-WG-LEPS definition of an inadequately labelled sample as one which has ‘less than 2 identifiers’ may not be suitable. As laboratories looked to define and standardize their own definitions of laboratory errors, it is hoped that peer comparison schemes will support harmonized approaches to detect and report laboratory errors.
Recording of errors
In order for laboratories to monitor the error rates for their services, a robust continuous mechanism of error collection must be established. When considering the systems used for highlighting quality failures, it is important to ensure that the processes are easy to use and understood by staff in the laboratory tasked with recording errors. Standardization of processes is important to ensure the accuracy of the recording mechanisms and enable effective staff training. To this end, all error collection procedures must be contained in a standardized operating procedure which states not just how to collect data but also collection frequency and what to do when error frequencies are outside predefined action limits. Below we detail a number of options for mechanisms to monitor error rates:
Audit
Laboratory quality audit is an essential element of a laboratory’s quality management system and should include scheduled audits of process effectiveness. ISO 15189: 2012 states that this should incorporate audits of preanalytical areas to collect information on the relative rates of errors. Examples of such audits might be: an audit of request forms to identify the percentage which do not have complete information regarding the requester; an audit of specimens to identify the percentage which do not have complete (or accurate) patient information; an audit of ‘booking-in’ processes to identify the percentage of booking in errors.
While audit forms a crucial part of the laboratory’s quality processes, the use of audit itself as a tool for data collection is limited as it is retrospective. Therefore, audit does not provide a real-time assessment of rates of error incidence, but a survey of error rates at a particular point in time. Further, audit does not immediately alert users to the quality issues with their requests. Finally, audits must be extensive in order to accurately reflect the true error rate of the laboratory, and as such are labour intensive to perform.
Manual recording processes
Systems of recording errors manually by means of ‘quality query reports’ (QQRs) have been described previously. 13 QQRs involve the use of report forms made available at workstations to records errors. The process is, again, labour intensive compared with automated systems of error identification in terms of both error recording and especially in reviewing data, and as such risks lower levels of compliance and under-reporting of errors. Variable frequencies in recorded errors which may be reflective of variations in compliance the recording process have been anecdotally observed and would be expected due to human factors. Such systems also have the disadvantage that they do not alert the user to quality failures.
Incident reporting
Incident reporting, often using risk management software such as Datix (Datix Limited, London, UK), should be part of any healthcare provider’s clinical governance processes. Medical laboratories should have processes of reporting errors using these systems. These systems have the advantage of being subject to host organization governance processes. However, given the in-depth nature of reporting required, such systems are not suited to recording large numbers of lower risk errors.
Use of laboratory information management systems
Laboratory information management systems (LIMS), primarily used to record receipt of specimens and report results, have the potential to be used to record quality errors, report them to users, act as repositories of error data and also gather data on error rates. Subclause 5.8.2 of the ISO 15189: 2012 Standard concerns report attributes, and states that the report should contain ‘comments on sample quality that might compromise examination results’ and ‘comments regarding sample suitability with respect to acceptance/rejection criteria’. 7 Many errors will still require manual identification but the use of the LIMS systems to record quality failures has the advantage that simple and standardized processes can be developed which makes error logging part of the normal sample receipt process and improves compliance. In the automated laboratory, some errors have the potential to be both identified and entered into the LIMS automatically, e.g. delayed transit, underfilled tubes, wrong specimen type, etc. LIMS use is both prospective (as opposed to retrospective methods described above) in alerting users to quality failures and retrospective, when regular data extractions are performed for trend analysis. Setting up such processes is often labour intensive; however once in place, there is minimal staff time associated with collecting and extracting the data.
Suggestions for recording errors via LIMS systems include the following.
Use of ‘Report Comment’ fields to record quality failures and highlight them in the report. For such systems, a balance between the standardization of error codes (which improves information gathering and review) and the flexibility to record errors of a variety of sources is required. Use of a test field in the LIMS system which can be used to record a number of laboratory errors that can then be reported to the user (i.e. book in a test that indicates an error and result this test with a coded comment to indicate the type of error). Use of coded comments in place of results for samples that cannot be analysed, e.g. HAEM for samples that cannot be analysed due to haemolysis. Keyword searches for comments in reports, e.g. ‘haemolysis’.
The configuration of the recording system will depend on the configuration of the LIMS system (and potentially other associated operating systems and middleware) and will have to be adapted to allow the recording of a variety of types of error. Laboratories should consider the merits of their LIMS systems when designing systems of recording errors. An ideal process will allow errors to be easily recorded in the laboratory, clearly reported to users and support the export and review of data for continuous improvement.
Data review
The advantage of using LIMS-based systems for the recording of errors is that it is possible to access real-time and/or retrospective data for review in a simple and effective way. Data export processes such as file transfer protocol or database enquiries enable data to be reviewed quickly and easily. Data should be reviewed and published to laboratory users periodically. Trends and patterns should be investigated in conjunction with the department involved. Data to review include the following.
Types of errors – error types (for example as described in Table 1) can be reviewed for trends and changes. Requesting locations – this can be important in identifying areas with high error rates for a particular indicator, such as specimen collection, transport or haemolysis, which may be a systematic issue relating to a particular service user. In such cases, training in specimen collection and/or improvements in logistics can have a beneficial impact on reducing error rates and therefore reducing repeat venepunctures and costs. Reporting to groups of clinical teams (for example, laboratory service commissioning groups or hospital clinical teams) may also be useful for establishing governance processes using laboratory data. Requesting clinicians – error rates relating to requesting (for example, appropriateness of a request or completion of a request form) Errors by laboratory department – this could indicate an issue with intralab sample processing. Benchmarking – error rates are compared against locally or nationally derived benchmarks or against other laboratories. Statistical process control – in the same way that the laboratory reviews quality control data for outliers, error rates can be compared against a target mean and standard deviations to identify statistically significant changes. Failure mode and effect analysis (FMEA) – FMEA requires a knowledge of the steps involved in the testing process, target areas of high risk and looks at methods of adapting processes to reduce failures.
14
Pareto analysis – Pareto diagrams organize elements in order of frequency of occurrence, enabling the laboratory to target areas of high risk. Errors can be grouped as described above, for example, by error type or location.
There are a number of quality management tools which can be utilized in the investigation of laboratory quality errors, including the following.
Laboratory errors and clinical governance
Once data are established for measuring rates of preanalytical laboratory errors, it is important to incorporate the information into the department’s quality management system and clinical governance processes.
KPIs
KPIs are measurands used by organizations to monitor and assess their effectiveness. In clinical laboratory services, a number of indicators have been suggested,15,11 many of which relate to issues regarding PAEs. In the UK, a recent Pathology Quality Assurance Review 8 describes the use of Pathology quality assurance dashboards (PQAD) to ensure pathology providers comply with service specifications and suggests that the dashboards should be developed with commissioners of Pathology services. There have been previous attempts to develop performance measures for Pathology services 16 and a UK national project is underway to develop a dashboard. PQADs can serve the dual purpose of allowing a laboratory to monitor key areas of its service (which includes elements from the preanalytical phase) and also provide data to users on the effectiveness of its service.
Risk management
Clause 4.14.6 of the ISO 15189: 2012 standard 7 relates to risk management and is a core area of the standard. It advises that the laboratory should ‘evaluate the impact of work processes and potential failures on examination results as they affect patient safety, and shall modify processes to reduce or eliminate the identified risks and document the decisions and actions taken’. Preanalytical steps in examination processes, including those that occur before the sample is received in the laboratory, are a key source of error in the TTP and risk management processes should incorporate such errors.
The ISO Technical Specification 22367:2008 ‘Medical Laboratories – reduction of error through risk management and continual improvement’
17
advises that laboratories should have processes for:
identifying high-risk processes where the potential error could lead to a safety risk for patients; identifying actual incidents associated with deviations from standard procedures; estimating and evaluating the associated risks to patient safety; controlling these risks; monitoring the effectiveness of the control undertaken.
ISO/TS 22367:2008 also recommends assigning actual (A) and potential (P) scores to the risks associated with processes, based on the potential impact of the errors on patient safety. Laboratories that frequently monitor rates of laboratory errors in the preanalytical phase, and use the information to facilitate preventative action to improve processes, are in a good position to monitor the impact of such errors on the results they report and assess the impact on patient safety.
Interventions
Efforts to decrease rates of PAEs have been documented previously but can be difficult. For example, Kemp et al. 18 used posters and screen savers to improve user awareness of testing protocols but showed no statistically significant change in the frequency of errors. Salinas et al., however, combined improvement actions (such as educational programs for nurses, technological interventions to automate manual steps in phlebotomy procedure and communication between the laboratory and peripheral community centres) with monitoring via a balanced scorecard to show an improvement in PAE rates over a 10-year period. 19
If it is assumed that laboratory testing protocols across different clinical areas have a consistent rate of occurrence within a defined variation, an alternative approach is to target interventions to areas which have higher error rates, for example higher rates of sample haemolysis or labelling errors. Here, FMEA with interventions such as training or process changes may be more effective. For example, some of the key causes of sample haemolysis relate to the blood collection step and overly vigorous collection. 20 If areas are identified where haemolysis rates are higher than expected, training and communication can be targeted to reduce this risk.
When targeting interventions to reduce error rates, it is important to approach issues in a ‘system’-based manner, as opposed to taking an ‘individual’ approach. 21 This approach emphasizes looking at the processes that a laboratory puts in place, in this case preanalytical processes such as sample collection and transport, to identify opportunities for improvement.
Conclusions
PAEs continue to represent the largest source of errors in the TTP. Harmonized QIs for PAEs have been suggested, 11 which allow consistent and efficient reporting via the laboratory’s quality monitoring processes. Although it is a challenge to ensure compliance in recording such errors, the use of the LIMS and/or middleware allows consistent recording of errors, alongside manual reporting by laboratory staff, and the end users.
Once data have been effectively gathered by the laboratory, risk analysis using FMEA and reporting of data using PQADs allow judgement about the severity and incidence of PAEs. Interventions can then be planned and prioritized, according to the data reported. Previous studies 9 have shown variation in data collection processes, which will limit the effectiveness of peer comparisons and as such inhibit opportunities for continual improvement. The process of data collection must therefore be standardized to allow comparisons to benchmarked data which will drive improvement in this area. Laboratories should carefully consider their processes to monitor PAEs to ensure that the processes for obtaining data are effective and areas of risk are monitored to enable quality improvement in the TTP.
In conclusion, the ACB-PA-WG recommends the use of the LIMS as a recording mechanism as in the long term, this provides the easiest and most standardized mechanism of data capture. The ACB-SIG-PA also recommends that the ability to provide such data should be a criterion when tendering for new LIMS systems in order to transfer the responsibility for developing mechanisms to the experts and produce standardized data. Other mechanisms are retrospective and have been shown to under report errors. Data from KPIs should be available to users and compared with benchmarked data or against peers.
Footnotes
Acknowledgements
This paper was written by the Association for Clinical Biochemistry and Laboratory Medicine (ACB) Special Interest Group for the pre-analytical phase.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
MC.
Contributorship
All conceived and discussed study. JW wrote the first draft. All edited manuscript.