
Abstract
Background
Mycophenolate mofetil has recently been reported to be effective against systemic lupus erythematosus. The influence of the pharmacokinetics of mycophenolic acid, the active form of mycophenolate mofetil and the major inactive mycophenolic acid phenolic glucuronide on the activity of the target enzyme inosine 5′-monophosphate dehydrogenase, is expected to be revealed. The aim of this study was to identify the factors associated with inosine 5′-monophosphate dehydrogenase activity in systemic lupus erythematosus patients.
Methods
Fifty systemic lupus erythematosus patients in remission maintenance phase (29 received mycophenolate mofetil [MMF+] and 21 did not [MMF−]) were enrolled. Median and interquartile range of dose of mycophenolate mofetil were 1500 and 1000–1500 mg/day, respectively. Stepwise multiple linear regression analysis was performed to assess the dependence between inosine 5′-monophosphate dehydrogenase activity and 25 predictor values including predose plasma concentrations of free mycophenolic acid and mycophenolic acid phenolic glucuronide.
Results
Median and interquartile range of predose total plasma concentrations of mycophenolic acid and mycophenolic acid phenolic glucuronide were 2.73 and 1.43–5.73 and 25.5 and 13.1–54.7 µg/mL, respectively. Predose inosine 5′-monophosphate dehydrogenase activity was significantly higher in MMF+ than MMF− patients (median 38.3 and 20.6 nmoL xanthosine 5′-monophosphate/g haemoglobin/h, P<0.01). The plasma concentration of free mycophenolic acid phenolic glucuronide, complement fraction C3 and body weight were significant predictors accounting for interindividual variability in the inosine 5′-monophosphate dehydrogenase activity (adjusted R2 = 0.52, P < 0.01) in a multivariate analysis.
Conclusions
Predose inosine 5′-monophosphate dehydrogenase activity was higher in systemic lupus erythematosus patients receiving mycophenolate mofetil therapy. Inosine 5′-monophosphate dehydrogenase activity may be determined by mycophenolic acid exposure and complement fraction C3 in systemic lupus erythematosus patients.
Keywords
Introduction
Mycophenolate mofetil (MMF) has been recently regarded to be effective in the treatment of systemic lupus erythematosus (SLE).1–4 MMF is rapidly converted to its active form mycophenolic acid (MPA). MPA is metabolized to its major inactive phenolic glucuronide (MPAG), and MPA shows enterohepatic recirculation. 5 MPA inhibits inosine 5′-monophosphate dehydrogenase (IMPDH) activity, which is the rate-limiting enzyme in de novo synthesis of DNA. IMPDH activity in peripheral monocytes and IMPDH1 gene expression was associated with frequency of acute rejection in kidney transplant recipients receiving MMF or MPA. 6 Genotypes of IMPDH1 and IMPDH2 were correlated with acute rejection and a decrease of IMPDH activity. 7 IMPDH activity in peripheral monocytes was found to be closely related to activity markers in lymphocytes in heart transplant recipients. 8 IMPDH activity was recognized as a pharmacodynamic indicator of MPA in solid organ transplant recipients. However, this still needs to be verified in SLE patients.
IMPDH activity is not available in SLE patients, although the studies below in solid organ transplant recipients remain controversial. IMPDH activity was reported to be decreased in the first four days and increased on the 40th day after transplantation using whole blood in kidney transplant recipients, and a negative correlation between IMPDH activity and MPA blood concentration was observed. 9 However, IMPDH activity was comparable between kidney transplant recipients first and continuously treated with MMF despite the pharmacokinetic difference in MPA. 10 We previously reported that short-term inhibition of IMPDH activity was dependent on the plasma concentration of MPA, and long-term induction of IMPDH activity was dependent on the above inhibition in kidney transplant recipients. 11
The relationships between the alteration of IMPDH activity and pharmacokinetics of MPA and MPAG still need to be clarified, especially in SLE patients. IMPDH directly reflects the degree of immune suppression; however, the usefulness of IMPDH activity and factors associated with IMPDH activity in SLE patients is unknown. We have previously described the factors that affect the pharmacokinetics of MPA and MPAG in SLE patients.4,12 The pharmacokinetics of MPA and MPAG in SLE patients as well as in kidney transplant recipients varies. The influence of the pharmacokinetics of MPA and MPAG on the activity of IMPDH is expected. The aim of this study was to identify the factors associated with IMPDH activity in SLE patients.
Material and methods
Subjects
Patient demographics.
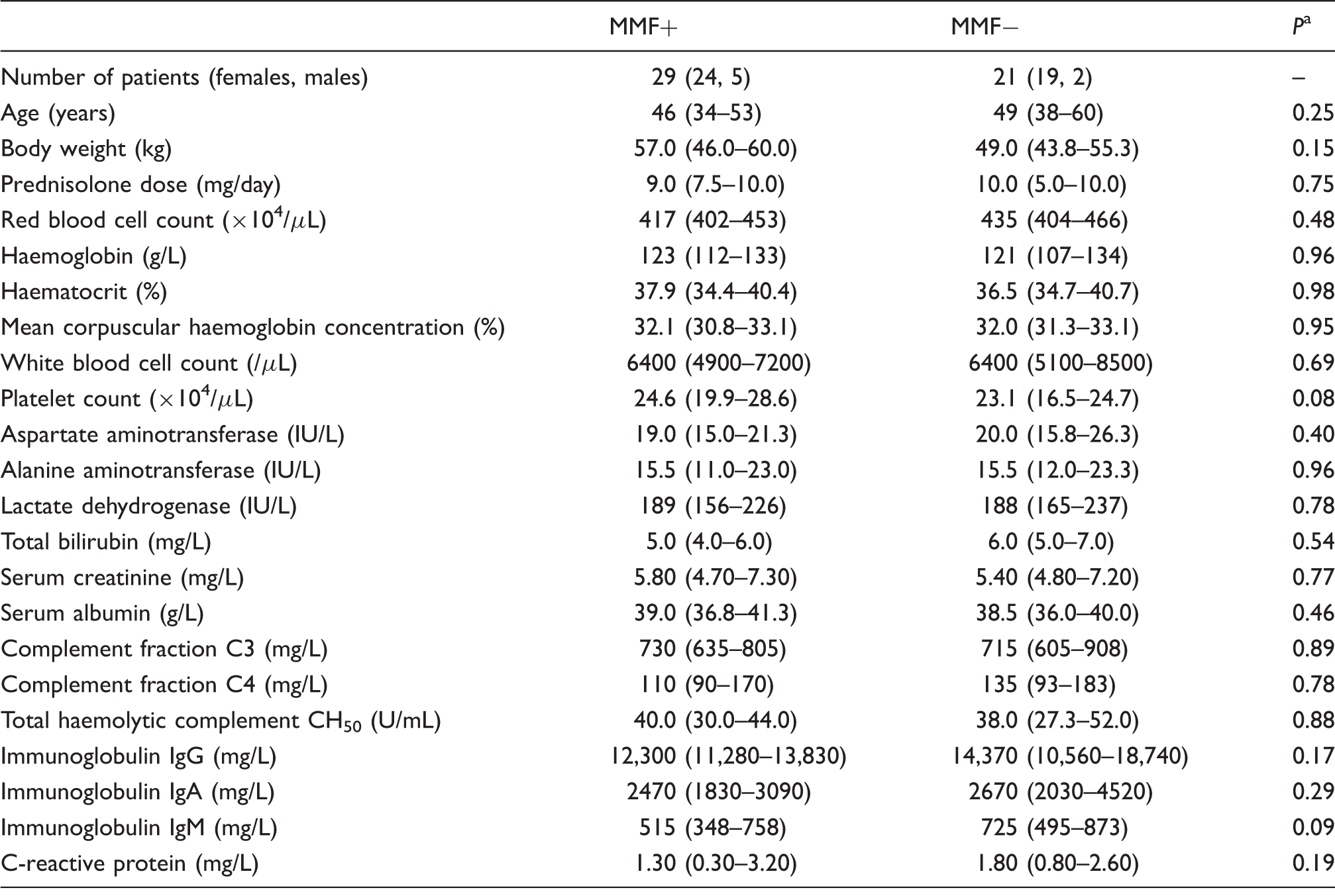
Note: Data are median and interquartile range unless otherwise stated.
Mann–Whitney U test.
Determination of plasma concentrations of MPA and MPAG and IMPDH activity
Blood specimens were drawn into tubes containing EDTA 12 h after an evening oral dose of MMF. Erythrocytes and plasma were obtained from EDTA blood by centrifugation at 1670 g at 4℃ for 10 min. IMPDH activity in erythrocytes was determined as previously described using high-performance liquid chromatography-ultraviolet (HPLC-UV). 11 The intra- and inter-assay precisions were 1.73–4.65% and 0.48–6.29%, respectively. The plasma concentrations of total and free MPA and MPAG were determined as previously described using HPLC-UV and HPLC-fluorescence.13,14 The intra- and inter-assay precisions were 0.47–2.57% and 1.55–3.51% for free MPA and 0.82–2.19% and 0.80–5.50% for free MPAG, respectively. The plasma concentration of mizoribine was determined as previously described using HPLC-UV. 15 The intra- and inter-assay precisions of mizoribine were 0.92–1.87% and 1.96–5.41%, respectively.
Statistical analysis
All statistical analyses were performed using IBM SPSS statistics version 21 (IBM Japan Ltd, Tokyo). A P < 0.05 was considered to indicate statistical significance. Differences in the IMPDH activity and patient background between the MMF+ and MMF− patients were analysed by the non-parametric Mann–Whitney U test. Box plots represented the median, 25th, and 75th percentiles. The whiskers indicated the range and extend within 1.5 times the length of the inner quartiles. Outliers, or those that lay more than 1.5 times the length of the inner quartiles, were indicated by the presence of open dots. Simple and stepwise multiple linear regression analyses (P < 0.05 to enter and P > 0.10 to remove) were performed to assess the dependence between IMPDH activity in erythrocytes and predictor values (plasma concentration of free MPA, plasma concentration of free MPAG, plasma concentration of mizoribine, blood concentration of cyclosporine, gender [male: 1 and female: 0], age, body weight, prednisolone dose, red blood cell counts, haemoglobin, haematocrit, mean corpuscular haemoglobin concentration, white blood cell counts, platelet count, aspartate aminotransferase, alanine aminotransferase, lactate dehydrogenase, total bilirubin, serum creatinine, serum albumin, complement fraction C3, complement fraction C4, total haemolytic complement CH50, immunoglobulin IgG, immunoglobulin IgA, immunoglobulin IgM and C-reactive protein).
Results
Patient demographics
No significant differences in patient demographics, including complement fractions C3 and C4, total haemolytic complement CH50, immunoglobulins and prednisolone dose between the MMF+ and MMF− patients were observed (Table 1). Twelve patients were treated with mizoribine, and three were treated with cyclosporine in MMF− patients. No patient received azathioprine or cyclophosphamide.
Plasma concentrations of total and free MPA and MPAG
The median and interquartile range of the predose plasma concentration of total MPA and MPAG were 2.73 and 1.43–5.73 µg/mL and 25.5 and 13.1–54.7 µg/mL, respectively, while those of free MPA and MPAG were 26.7 and 15.9–46.9 ng/mL and 6.72 and 2.42–8.63 µg/mL, respectively.
IMPDH activity between MMF+ and MMF− patients
Figure 1 shows predose IMPDH activity in the MMF+ and MMF− SLE patients. There was a significant difference between the MMF+ and MMF− patients (median 38.3 and 20.6 nmoL xanthosine 5′-monophosphate/g haemoglobin/h, P < 0.01).
IMPDH activity in MMF+ and MMF− SLE patients. Box plots represent the median, 25th, and 75th percentiles. The whiskers indicate the range and extend within 1.5 times the length of the inner quartiles. Outliers, or those which lay more than 1.5 times the length of the inner quartiles, are indicated by the presence of open circles. *P < 0.01, Mann–Whitney U test.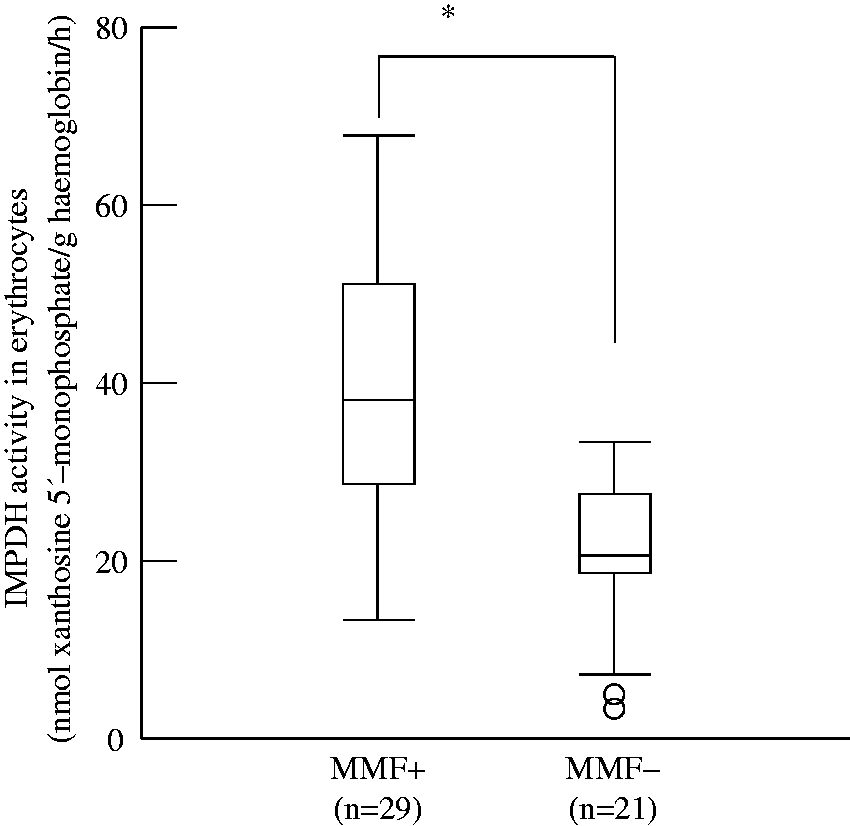
Predictor valuables of IMPDH activity
Factors affecting IMPDH activity in SLE patients with stepwise multiple regression analysis.
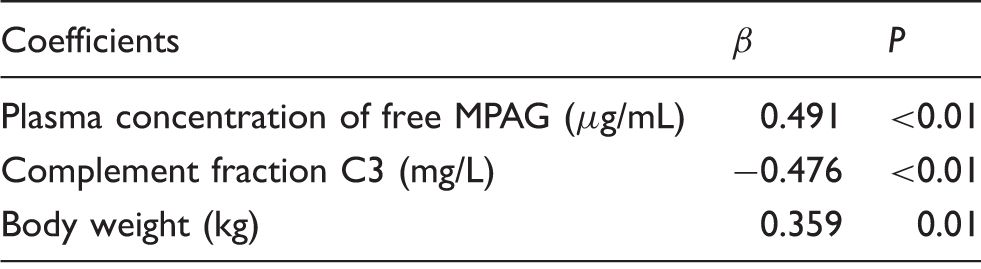
n = 50; adjusted R2 = 0.523; P < 0.01; β; standardized partial regression coefficient.
Discussion
The current study has found relationships between the plasma concentration of free MPAG and complement fraction C3 with IMPDH activity in SLE patients. Few reports are available on the therapeutic range of the plasma concentrations of MPA and MPAG,12,16 and there are no reports on IMPDH activity in SLE patients. The clinical significance of monitoring IMPDH activity in SLE has thus far not been reported.
No significant differences in patient demographics were observed between the MMF+ and MMF− groups (Table 1). We described the therapeutic efficacy of MMF in Japanese SLE patients. 12 MMF therapy improved complement fraction and immunoglobulins and decreased prednisolone dose in a previous study. We expected to observe some differences in patient demographics between the MMF+ and MMF− SLE patients. Need for treatment was reported to be influenced by disease activity. 17 However, no significant differences were observed, most likely because the current study enrolled SLE patients in remission maintenance phase without consideration of disease activity.
The plasma concentration of MPA in the current study was comparable to other reports on MMF effectiveness in SLE patients.4,12,18,19 IMPDH activity in MMF+ SLE patients was higher than that in MMF− patients with the above therapeutic plasma concentration of MPA (Figure 1). IMPDH activity may also be induced during MMF therapy in SLE patients as well as in kidney transplant recipients. 11 IMPDH activity was somewhat variable even in MMF− SLE patients, indicating that some endogenous factors may have influenced IMPDH activity.
Stepwise multiple regression analysis was performed in order to identify valuables affecting IMPDH activity. The present study found three factors associated with IMPDH activity; plasma concentration of free MPAG, complement fraction C3 and body weight. We have previously reported that IMPDH activity in kidney transplant recipients was associated with the plasma concentrations of MPA glucuronides and MPA, serum creatinine, age and lactate dehydrogenase activity in descending order of magnitude. 11 The plasma concentration of MPA metabolite was most impressive in both studies. Serum creatinine may be a therapeutic indicator in kidney transplant recipients in much the same way that complement fraction C3 may be to SLE patients. The present study obtained results similar to those of a previous study. 11
The plasma concentration of free MPAG was positively correlated with IMPDH activity in the current study. MPAG has no inhibitory effect of IMPDH activity. 5 MPAG reflects total exposure of MPA, because it is a main metabolite of MPA. 5 The correlation between IMPDH activity and plasma concentration of free MPAG implied that predose IMPDH activity was increased with MPA exposure.
Complement fraction C3 was negatively correlated with IMPDH activity. Complement fraction is an indicator of SLE disease activity. Complement fraction C3 is consumed and decreases in SLE active phase. We have previously found improvement of complement fraction after MMF treatment in SLE patients. 12 Theoretically, IMPDH activity reflects DNA synthesis in white blood cells and is believed to increase in active phase. Both the lower complement fraction C3 and higher IMPDH activity were caused by the disease itself. This may be the reason for the inverse correlation between IMPDH activity and complement fraction C3, and they would not directly interact.
This study has several limitations. First, the number of patients was too small to clarify the influence of endogenous factors on IMPDH activity. Second, it is a cross-sectional study, and the interday variability of IMPDH activity was not evaluated. Third, we employed single time point sampling and evaluated predose IMPDH activity. We speculated our study results to indicate decreased IMPDH activity at the peak plasma concentration of MPA and increased IMPDH activity at the trough plasma concentration of MPA.11,20 Further study may be needed to elucidate these uncertain factors.
Conclusions
Predose IMPDH activity was higher in SLE patients receiving MMF therapy than MMF− patients. IMPDH activity was dependent on the plasma concentration of MPAG, but not that of MPA. In addition, IMPDH activity was negatively correlated with complement fraction C3. Predose IMPDH activity may be variable by MPA exposure and complement fraction C3 in SLE. Further study will provide stronger conclusion whether IMPDH activity was induced or not in SLE patients using baseline IMPDH activity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by Hamamatsu University School of Medicine.
Ethical approval
The Ethics Committee of Hamamatsu University School of Medicine approved the protocol (18-100).
Guarantor
TN.
Contributorship
YM wrote the first draft of the manuscript and was involved in data analysis. YM, TN and JK researched literature and conceived the study. TN and JK were involved in protocol development and gaining ethical approval. KS and NO were involved in patient recruitment. All authors reviewed and edited the manuscript and approved the final version of the manuscript.