
Abstract
Backgrounds
Effects of myocardial injury on E-selectin remain unclear. Thus, we investigated the diagnostic value of E-selectin for myocardial injury in paediatric patients with mycoplasma pneumoniae pneumonia.
Methods
In this prospective and blinded clinical study, plasma E-selectin, cardiac troponin I, creatine kinase isoenzyme MB, interleukin-6 and tumor necrosis factor alpha concentrations were measured in paediatric patients with mycoplasma pneumoniae pneumonia (MPP group, n = 138). The control group comprised 120 healthy children. The definition of cardiac injury was based on cardiac troponin I or CK-MB (with or possibly without abnormal electrocardiogram evidence). Diagnostic value of E-selectin for myocardial injury was determined by analysing receiver operating characteristic curves.
Results
Among the 138 mycoplasma pneumoniae pneumonia patients, 40 patients were identified with myocardial injury, while 98 patients were identified without myocardial injury. Plasma E-selectin concentrations were: 40.22 ± 4.80 ng/mL, in patients with myocardial injury; 18.55 ± 2.16 ng/mL, in patients without myocardial injury and 12.39 ± 3.27 ng/mL, in healthy children. For the 40 patients identified with myocardial injury, area under the receiver operating characteristic curve value for plasma E-selectin concentrations was 0.945 (95% CI: 0.899–0.991), and optimal diagnostic cut-off value was 29.93 ng/mL (positive likelihood ratio = 72.5).
Conclusion
E-selectin was shown to be an effective index for myocardial injury in paediatric patients with mycoplasma pneumoniae pneumonia, and its role in other causes of myocardial injury warrants further investigation.
Introduction
Myocardial injury is the most common and serious extra-pulmonary damage caused by mycoplasma pneumoniae pneumonia (MPP). However, there are no confirmed diagnostic criteria for myocardial injury in this condition. Currently, the diagnosis of myocardial injury in MPP or other potential aetiologies is mainly based on myocardium-related protein or creatine kinase isoenzyme MB (CK-MB) release.1,2 There are many cardiac injury markers, in which troponins (T and I) and CK-MB are most commonly used. However, the positive expression rate of cTnI and CK-MB is not 100%. Hence, the diagnosis of cardiac damage is difficult.
E-selectin expression increases after myocardial ischaemia/reperfusion injury; and consequently, it appears to be a lasting biomarker of myocardial injury. 3 However, its time course and precise quantity of expression remain unclear.
We investigated the effectiveness of E-selectin for diagnosing myocardial injury in paediatric patients with MPP and identified cut-offs that may be used to confirm the diagnosis.
Materials and methods
Ethical approval
This study was approved by the ethics committee of the Affiliated Shunde Women and Children’s Hospital of Jinan University. All parents provided written informed consent.
Patients
All subjects were recruited from patients treated at the Affiliated Shunde Women and Children’s Hospital of Jinan University between June 2013 and June 2015.
A total of 138 consecutive paediatric patients with MPP were prospectively enrolled based on inclusion and exclusion criteria.
Inclusion criteria: MP-IgM antibodies > 1:160 for MPP in paediatric patients with pneumonia1 and cTnI > 150 ng/L/or CK-MB > 24 IU/L are consistent with myocardial injury.2
Exclusion criteria: Patients treated for myocardial injury prior to hospital admission.
MPP and MPP with myocardial injury were diagnosed by senior physicians, and these physicians only used MP-IgM, cTnI or CK-MB results to make the diagnosis. A total of 138 consecutive patients were recruited in the study including 71 males and 67 females, and average age was 2.6 years (range: 1–7 years). Among the 138 patients, 40 patients were identified with myocardial injury (myocardial injury group), while 98 patients were identified without myocardial injury (non-myocardial injury group). In addition, 120 healthy children (control group) were recruited in the study including 63 males and 57 females, and average age was 2.5 years (range: 1–7 years).
Laboratory assays
All study procedures of E-selectin, IL-6 and TNF-α were carried out under blind conditions: clinicians who treated the patients and laboratory personnel were not aware of both study results and patient’s clinical condition.
The measurement of E-selectin, IL-6, TNF-α, cTnI and CK-MB concentrations was fully automated. Venous blood samples (5 mL) were collected in tubes containing EDTA-K2. Blood samples were drawn from subjects in the experimental group (myocardial injury and non-myocardial injury groups) during hospital admission, while blood samples were drawn from subjects in the control group during routine check-ups.
Plasma E-selectin concentration was assayed by ELISA using a ThermoMK3 Enzyme-linked immunity analyzer (Bender Medsystems Company, Vienna, Austria). Coefficient of variance (CV) within each group was 2.85%, and CV between groups was 3.26%. Currently, there is no defined E-selectin reference range.
Plasma MP-IgM antibodies were analysed by immune agglutination assay using a kit (Fujirebio Inc, Tokyo, Japan).
Plasma cTnI and CK-MB concentrations were analysed by chemiluminescence using an AU680 Beckman full-automatic Chemiluminescence analyzer (Beckman Coulter, Inc., Kraemer, USA) with a cTnI reference range of 0–30 ng/L, where >150 ng/L is consistent with myocardial injury; and a CK-MB reference range of 0–24 IU/L, where a CK-MB value > 24 IU/L is consistent with myocardial injury.
Plasma IL-6 and TNF-α concentrations were assayed by radioimmunoassay using a ThermoMK3 Enzyme-linked immunity analyzer (Bender Medsystems, Vienna, Austria); the reference ranges for IL-6 and TNF-α are ≤5.9 pg/mL and ≤8.1 pg/mL, respectively.
The definition of cardiac injury was based on cTnI or CK-MB (±abnormal electrocardiogram evidence).1,2
Statistical analysis
Statistical analysis was performed using SPSS version 17.0 statistical software (SPSS, Inc., Chicago, IL, USA), and ROC curves were drawn using GraphPad software (GraphPad Software, Inc. La Jolla, USA).
Statistical analysis was used to determine plasma E-selectin cut-off values for myocardial injury in paediatric patients with MPP, which included area under the curve (AUC), 95% CI, sensitivity, specificity and positive likelihood ratio (LR). ROC curve statistical analysis was performed to determine the diagnostic accuracy of E-selectin, IL-6 and TNF-α for diagnosing myocardial injury.
Distributions were tested for normality. For normally distributed data, continuous variables were tested by independent sample t-test, F-test and Mann-Whitney U-test. For non-normally distributed data, continuous variables were tested non-parametrically by Wilcoxon test.
Results
There was no significant statistical difference between the myocardial injury group and control group for age and gender (P > 0.05).
E-selectin, cTnI, IL-6 and TNF-α concentrations were normally distributed (P < 0.001); therefore, mean ± standard deviation
Myocardial injury
Among the 138 patients, 40 patients were identified with myocardial injury, while 98 patients were identified without myocardial injury. The incidence of myocardial injury was 29%. Among the 40 patients with myocardial injury, anomalies cTnI were elevated in 17 patients (42.5%), CK-MB was elevated in 23 patients (57.5%) and 16 patients had elevation of both cTnI and CK-MB.
Biomarker data
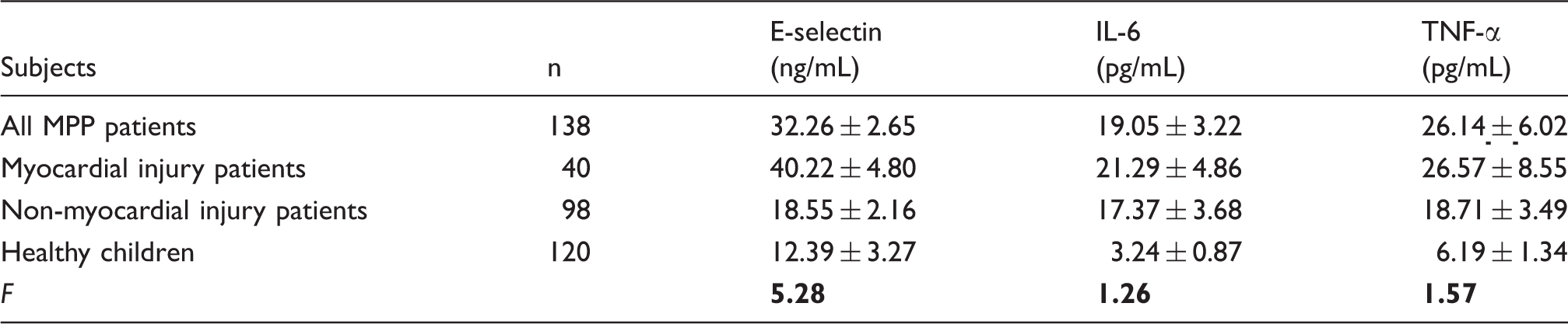
In the overall groups of patients, plasma E-selectin, IL-6 and TNF-α concentrations were 32.26 ± 2.65 ng/mL, 19.05 ± 3.22 pg/mL and 26.14 ± 6.02 pg/mL, respectively. Results for patients with myocardial injury were 40.22 ± 4.80 ng/mL, 21.29 ± 4.86 pg/mL and 26.57 ± 8.55 pg/mL, respectively; results for patients without myocardial injury were 18.55 ± 2.16 ng/ml, 17.37 ± 3.68 pg/mL and 25.71 ± 3.49 pg/mL, respectively; and results for healthy children were 12.39 ± 3.27 ng/mL, 18.36 ± 3.31 pg/mL and 23.22 ± 6.37 pg/mL, respectively. There were significant differences between groups for E-selectin (F = 5.28, P < 0.001), and there were no significant differences between groups for IL-6 and TNF-α (F = 1.37, 1.06; all P > 0.05) (Table 1 and Figure 1).
Comparison of E-selectin concentrations in MPP patients with myocardial injury, without myocardial injury and in healthy children. Comparison of E-selectin, IL-6 and TNF-α concentrations in all MPP patients and healthy children MPP: mycoplasma pneumoniae pneumonia; TNF-α: tumour necrosis factor alpha; IL-6: interleukin-6. Note: E-selectin P < 0.001; IL–6 and TNF-α, all P > 0.05.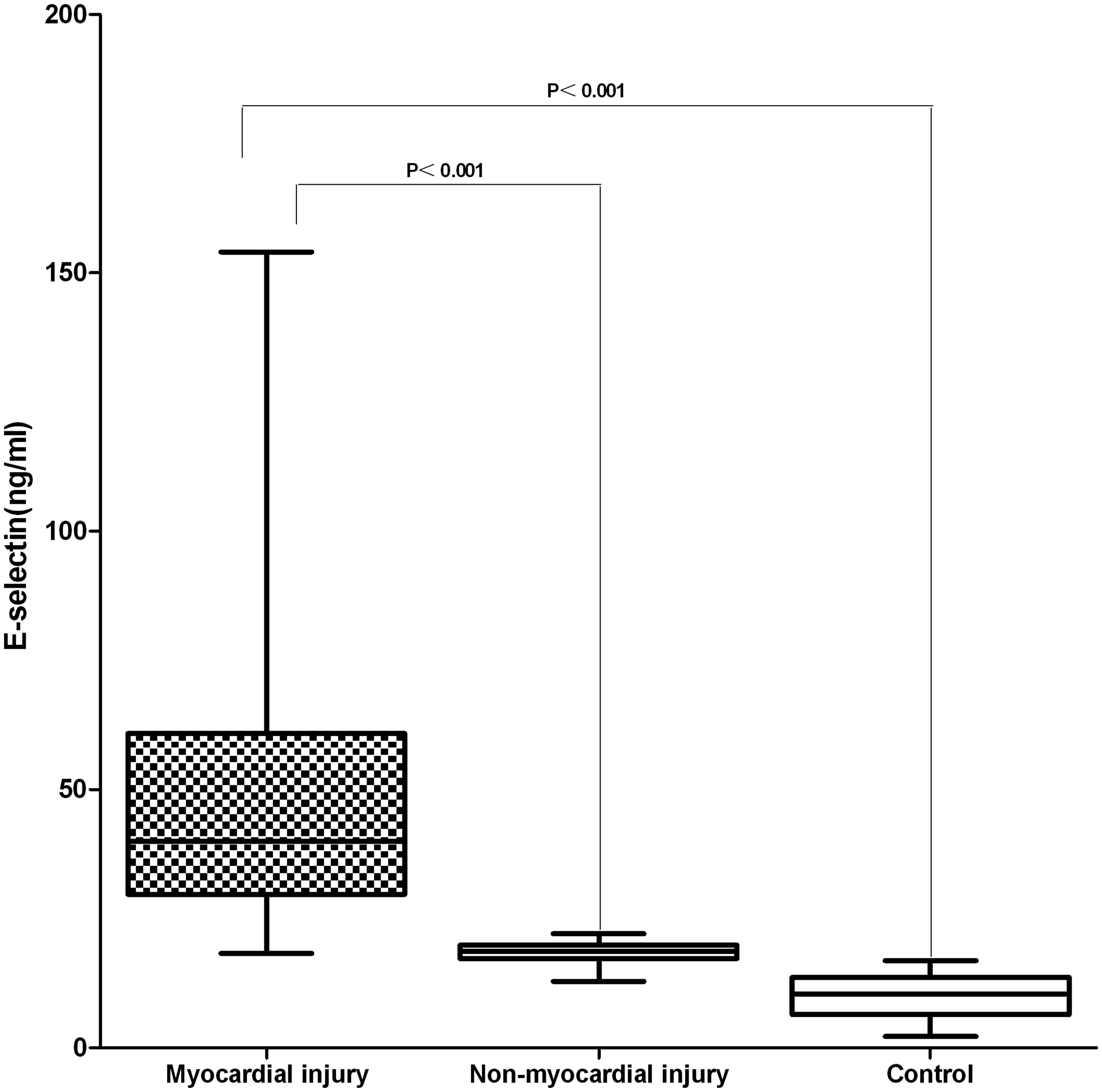
Myocardial injury can be divided into three degrees of severity (diagnosis of cardiac injury depends on the cTnI index or CK-MB, while cardiac injury severity depends on user-definition):
ROC curve analysis
E-selectin
For myocardial injury diagnosis, AUC of E-selectin was 0.945 (95% CI: 0.899–0.991). Further, sensitivity, specificity and Youden index results for diagnosing myocardial injury by E-selectin were 0.801, 0.999 and 0.800, respectively. For myocardial injury diagnosis, optimal cut-off values for E-selectin were 29.67 ng/mL, while positive LRs for E-selectin were 72.5 (LRs > 10 have diagnostic value). These results indicate that analyses were effective for diagnosing myocardial injury (Table 2 and Figure 2). Thus, E-selectin is a better index for myocardial injury. When E-selectin was <25 ng/mL, negative LR was 0.09; thus, myocardial injury can be ruled out.
Comparison of receiver operating characteristic (ROC) curves for E-selectin, IL-6 and TNF-α in all MPP patients and in healthy children. Cut-off values of plasma E-selectin, IL-6 and TNF-α for myocardial injury in paediatric patients with MPP. LR: likelihood ratio; TNF-α: tumour necrosis factor alpha; IL-6: interleukin-6; AUC: area under the curve.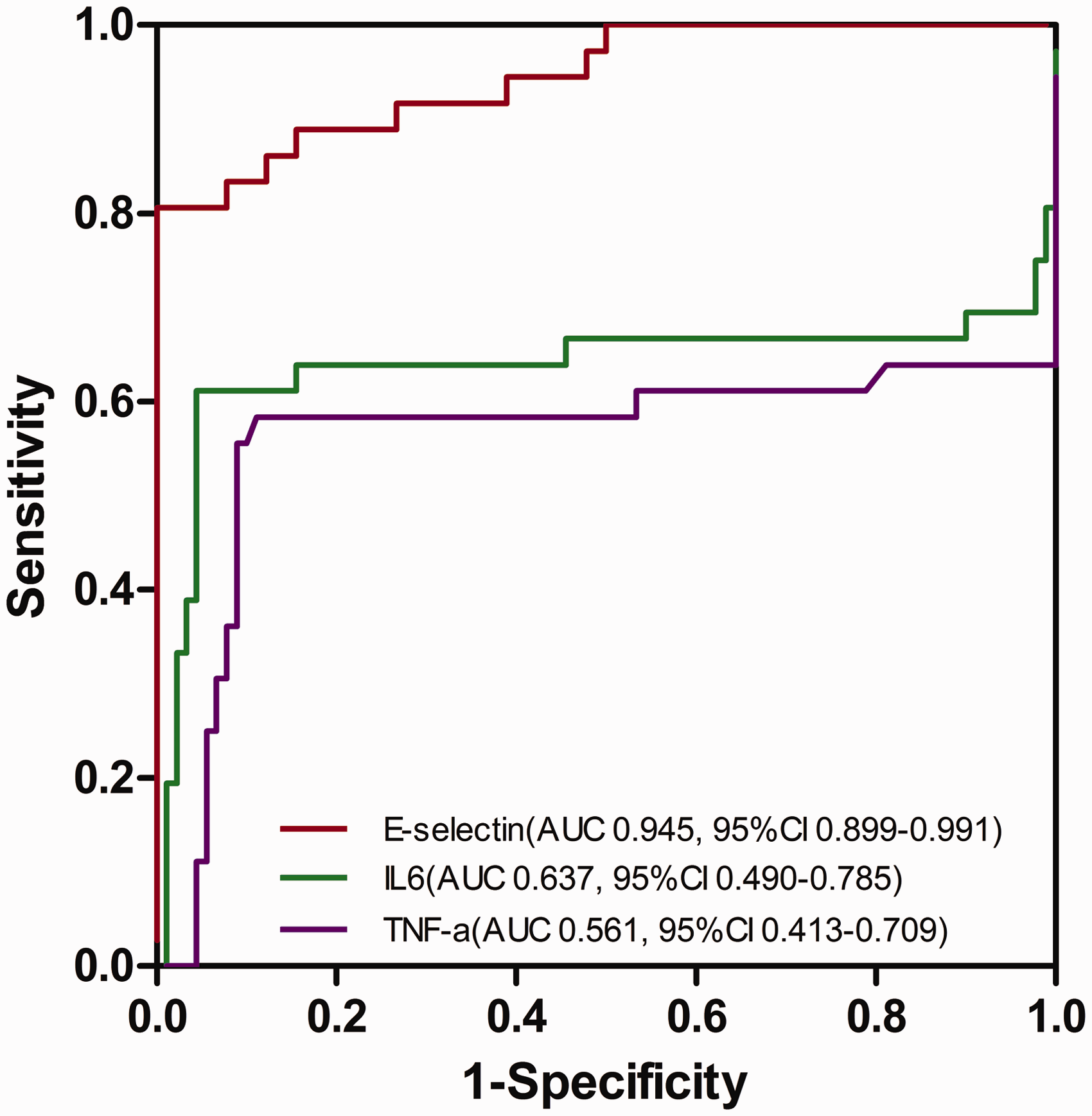

IL–6 and TNF-α
For diagnosing myocardial injury, AUCs for IL-6 and TNF-α were smaller (0.637 and 0.561, respectively) than AUCs for E-selectin. Therefore, diagnostic accuracy for myocardial injury was low for IL-6 and TNF-α. Sensitivity, specificity and Youden index for diagnosing myocardial injury were: 0.611 and 0.556, 0.922 and 0.911 and 0.533 and 0.467, respectively. In all cases, sensitivity and specificity were low, and positive LRs were 7.86 and 6.25, respectively. All LR values were <10, suggesting that these markers have no diagnostic value for myocardial injury (Table 2 and Figure 2).
Cut-off selection
Optimal cut-off value for plasma E-selectin for diagnosing myocardial injury in paediatric patients with MPP was 29.67 ng/mL.
Discussion
Myocardial injury complicates many diseases, particularly paediatric patients with MPP. 4 This occurs as a result of an MP antigen in myocardial cells, leading to autoantibody production and consequent myocardial cell injury.5,6 E-selectin is a member of the selectin family of adhesion molecules and an important inflammatory mediator that affects cellular immune function. It is a cell surface glycoprotein (molecular weight: 107–115 kDa) that binds to active endothelial cell surfaces. When interleukins and TNF-α are released by damaged cells, E-selectin binds to endothelial cells, allowing neutrophil attachment to the vessel wall and consequent aggregation, thus promoting inflammation and immune injury. E-selectin overexpression can then be analysed in plasma.7,8
E-selectin expression remains elevated and can be assayed following myocardial ischaemia/reperfusion injury. This means that E-selectin is a ‘memory’ biomarker for myocardial ischaemia/reperfusion.3,9 The diagnosis of acute coronary syndrome remains challenging especially in patients without clear symptoms or electrocardiographic and/or biomarker features. A hallmark of ischaemia/reperfusion is activation of endothelial cells leading to altered expression of molecular markers, including selectins. 10 Therefore, E-selectin concentrations have been associated with various cardiovascular diseases. 7 This study confirms previous reports,7–10 wherein E-selectin is unusually high in patients with myocardial injury due to MPP.
Plasma E-selectin, IL-6 and TNF-α can be reliably detected from blood drawn with the use of EDTA-K2 as an anticoagulant. E-selectin, IL-6 and TNF-α concentrations are relatively stable in blood samples stored at −80℃ for several months. The detection of E-selectin, IL-6 and TNF-α is fully automated. Thus, user error can generally be avoided or diminished.
Many biomarkers are used in clinical practice to identify myocardial injury; cTnI and CK-MB are the most commonly used biomarkers.11–16 However, the positive expression rate of cTnI and CK-MB is not 100%, and is 25–42% and 35–68%, respectively, 11 which is similar to the results of this study. The diagnosis of myocardial injury has certain limitations, because the expression of cTnI and CK-MB is influenced by many factors, which exist within the myocardium, CK-MB is also expressed in skeletal muscle and brain tissue, cTnI is a specific indicator of myocardial injury and an independent predictor for the severity of myocardial injury; however, sensitivity is low using the standard sensitivity assays. Hence, the diagnosis of myocardial injury can be difficult in certain circumstances.
There is a continuous search for better indices of myocardial injury. Our study revealed that AUC value (0.945) for E-selectin was high for diagnosing myocardial injury. Sensitivity (0.801) and specificity (0.999) of E-Selectin were also higher. Youden index had an AUC value of 0.800, a cut-off value of 29.67 ng/mL for the diagnosis of myocardial injury and a positive LR value of 72.5. These results strongly suggest that E-selectin is an effective index. Although IL-6 and TNF-α were abnormal, sensitivity and specificity were lower and AUC values were smaller and diagnostic effectiveness was correspondingly lower.
The expression of selectins in myocardial ischaemia looks promising as a clinical diagnostic biomarker. 10 In this study, E-selectin was an effective index for myocardial injury, in MPP patients.
Conclusion
E-selectin can remain stable for a long time in blood. ELISA is a simple and low-cost method that could provide relatively rapid results (results are available within 4 h) with high sensitivity and specificity. This study revealed that the optimal diagnostic cut-off value of E-selectin for myocardial injury was 29.67 ng/mL. E-selectin was shown to be an effective index for myocardial injury in paediatric patients with MPP and its role in other causes of myocardial injury warrants further investigation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Bureau of Science and Technology of Foshan City, China [Grant No. 201308230].
Authors’ contribution
M-HD and C-WL contributed equally to this work.
Ethical approval
This study was approved by the ethics committee of the Affiliated Shunde Women and Children’s Hospital of Jinan University. All parents provided written informed consent.
Guarantor
C-WL.
Contributorship
M-HD: design, writing and editorial; C-WL: design, review and editorial; Y-NS, X-LZ, FW: implemented the study and data collection.