
Abstract
Mycoplasma pneumoniae pneumonia (MPP) is a common disease in infants and young children. MPP can also be a potential cause of healthcare-associated pneumonia. However, it is challenging to make an accurate diagnosis in a timely fashion. Our goal is to determine the assay consistencies of acridinium ester chemiluminescence immunoassay (AECLIA) and gelatin particle agglutination (GPA) test for the detection of Mycoplasma pneumoniae (MP) antibody. In this study, a total of 1404 children with suspected MPP were enrolled. Among them, 130 were diagnosed as MPP positive by mycoplasma culture, and 186 were negative. MP antibodies were detected by AECLIA, enzyme-linked immunosorbent assay (ELISA) and GPA. Consistency rates, differences among assays, and diagnosis performance were compared for the three methods. The independent χ2 test results of AECLIA and ELISA for the detection of MP-IgG and MP-IgM antibodies were χ2 = 29.210, P < 0.001; χ2 = 9.081, P = 0.017, respectively, suggesting that the two detection methods are well correlated. Similar analyses were done for the comparison of AECLIA and GPA as well as the comparison of ELISA and GPA. The positive rates of these methods agree with epidemiology data and have good consistency. Thus, AECLIA with a much shorter assay time could be a better option for the screening of MPP.
Keywords
Introduction
Rapid and accurate test results are often needed for patient care and infection prevention in the setting of healthcare-associated infections (HAIs). Mycoplasma pneumoniae pneumonia (MPP) is a common disease in infants and young children, caused by the infection of Mycoplasma pneumoniae (MP), a very small bacterium in the class Mollicutes. 1 In the early stage of pediatric MP infection, there is a lack of specific symptoms, which leads to high rates of misdiagnosis and missed diagnosis. This makes it extremely difficult for the early treatment of pediatric MPP. MPP can also be a potential cause of healthcare-associated pneumonia. Therefore, it is critical to establish a simple and accurate diagnosis method. 2 Positive culture of mycoplasma is the gold standard for the diagnosis of MP infection, but it can be done only in a well-equipped laboratory and with well-trained biomedical staff. Furthermore, the turnaround time for the culture experiment is so long that infected kids often miss the optimal treatment time window. Therefore, the contribution of the culture results in instructing early therapy is extremely limited. 3 At present, the commonly used MPP detection methods in clinical practice are enzyme-linked immunosorbent assay (ELISA) and gelatin particle agglutination (GPA), but the ELISA method has large standard error, and some studies have suggested that ELISA and GPA methods lack consistency. 4 The GPA method has better diagnostic performance, but lack of automation compatibility and the assay time is long, which is not suitable for the large-scale clinical applications. 5 Chemiluminescence has high sensitivity and specificity, and the assay time is short, and the degree of automation is high. The detection of MP antibody by acridine ester chemiluminescence has been employed for the early diagnosis of MPP. 6 This method has also been used for the analysis and antibiotic resistance of Chlamydia pneumoniae and MP in healthy volunteers. 4 However, acridine ester chemiluminescence assay has not been compared to ELISA and PA extensively, and there is no research on the diagnostic efficacy of acridine ester chemiluminescence method for MPP in China. Therefore, this study mainly explored the efficiency of acridinium ester chemiluminescence on the detection of serum MP antibody in children with suspected Mycoplasma pneumoniae infection and provided a rationale to promote its clinical applications.
Materials and methods
Detection method
Each fasting patient was drawn 10 mL of peripheral blood in the morning at admission, 5 mL of which used acridinium ester chemiluminescence immunoassay (AECLIA) to detect mycoplasma-related antibodies MP-IgG and MP-IgM (Shenzhen YHLO Biotech Co., Ltd., China). 5 Assays were done per manufacturer’s instructions and data were acquired by the iFlash 3000 chemiluminescence immunoassay analyzer (Shenzhen YHLO Biotech Co., Ltd). The inter-assay precision and intra-assay precision were tested according to the CLSI EP15-A2 document and the CLSI EP5A2 file, and the linear index of the MP-IgG antibody was detected using a fully automated chemiluminescence immunoassay analyzer with reference to the CLSI EP6-A document. Positivity determination: considered as positive if five times greater than blank group, considered as MP positive if both MP-IgG and MP-IgM were positive, and MP positivity was analyzed. The other 5 mL samples were tested for MP-IgG and MP-IgM levels by ELISA: anti-Mycoplasma pneumoniae ELISA IgG (EUROIMMUN, Germany) and anti-IgM assay kit (Anti-Mycoplasma pneumoniae ELISA IgM; EUROIMMUN, Germany). Positivity is determined according to the standard curve as per manufacturer’s instruction. The MP antibody test kit (International Note 20173406811) is used for the GPA method, and a positive result is considered if the M antibody titer was ⩾1:160.
Statistical analysis
SPSS 19.0 software was used for data processing. The data were represented as (mean ± standard error), and student t-test was used for comparison between groups; the count data rate (%) was expressed by independent χ2 test; the consistency of the two methods was compared using the pair χ2 test. The kappa analysis was used to test the consistency with the GPA method. Kappa ⩾ 0.8 is considered as good consistency; 0.8 > kappa ⩾ 0.4 indicates consistency; kappa < 0.4 indicates poor consistency, and P < 0.05 indicates significant difference.
Results
A total of 1404 children with suspected MPP who were treated in our hospitals were enrolled from November 2016 to May 2018. The age ranged from 0 to 14 years, including 712 males and 692 females. Among them, 130 children were diagnosed as MPP by mycoplasma culture, 70 males and 60 females, with an average age of (6.14 ± 2.23) years; 186 were non-MPP children, 94 males and 92 females, with an average age of (6.61 ± 2.34) years; there was no significant age difference between the two groups (P > 0.05). The inclusion criteria of the observation group were (1) age 0–14 years, (2) diagnostic criteria for children with pneumonia, 7 (3) MP positive for culture, (4) complete patient information, and (5) children’s immediate family member or guardian signs the informed consent form. The exclusion criteria of the control group and the observation group were (1) using other anti-infective drugs such as glucocorticosteroid within 3 months, (2) incomplete information or unable to determine whether it was MP infection, and (3) withdrawal.
We first did comparison of the consistency between AECLIA and ELISA methods. The independent χ2 test results of AECLIA and ELISA for detection of MP-IgG and MP-IgM antibodies were χ2 = 29.210, P < 0.001; χ2 = 9.081, P = 0.017, suggesting that the two methods are significantly correlated. However, significant differences in the test results between the two methods are observed (see Table 1).
Comparison of AECLIA (case) and ELISA (case).

AECLIA: acridinium ester chemiluminescence immunoassay; ELISA: enzyme-linked immunosorbent assay.
A second comparison between AECLIA and GPA has been carried out. The acridine ester chemiluminescence method and the GPA detection of MP antibody were χ2 = 49.782, P < 0.001, suggesting that the two methods are significantly correlated. However, significant differences in the test results between the two methods are observed (Table 2). The kappa value is 0.626 and suggests consistency between the two methods.
Consistency ratio between AECLIA (case) and GPA (case).

AECLIA: acridinium ester chemiluminescence immunoassay; GPA: gelatin particle agglutination.
Finally, we compared ELISA and GPA methods. The ELISA method and PA test MP antibody χ2 = 93.341, P < 0.001, suggest that the two methods are significantly correlated. However, significant differences in the test results between the two methods are observed (see Table 3). The kappa value is 0.496 and suggests consistency between the two methods.
Consistency ratio between ELISA (case) and GPA (case).
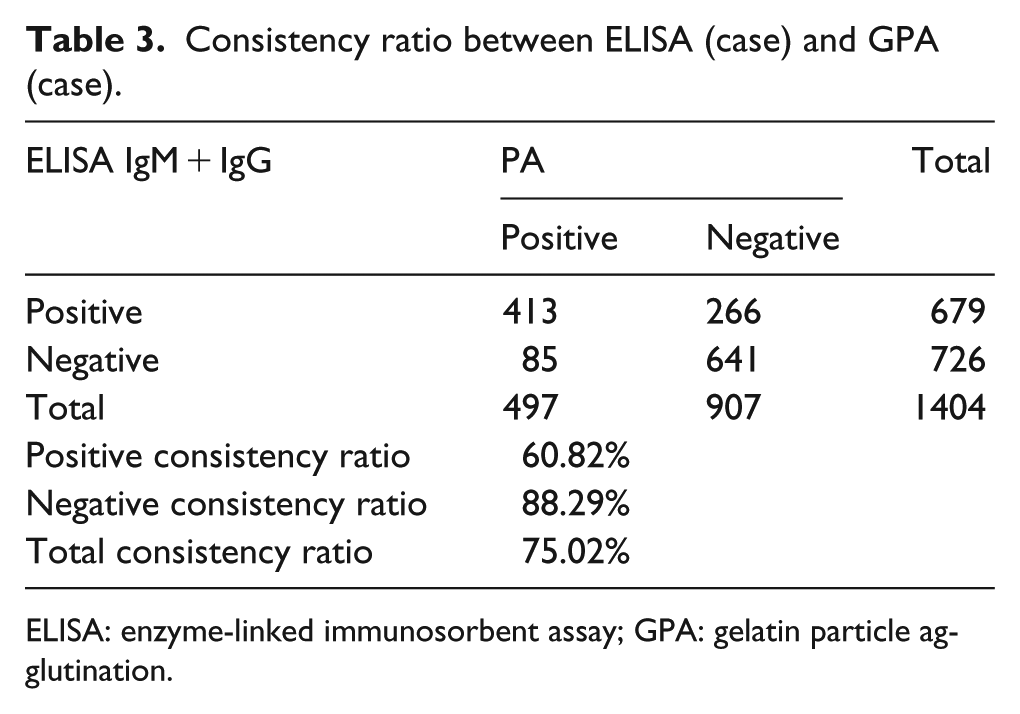
ELISA: enzyme-linked immunosorbent assay; GPA: gelatin particle agglutination.
Discussion
Pneumonia is one of the most common diseases in children. MPP caused by MP infection is one of the most serious pneumonia. If not treated in a timely fashion, MPP infection can be life threatening. 8 The diagnosis and treatment of pediatric MPP have always been clinically challenging. It is especially important to establish a simple and effective method to discriminate MPP and other bacterial pneumonia. 9 Chemiluminescence immunoassay combines high-sensitivity chemiluminescence assays with highly specific immunoassays to detect a variety of antigens, antibodies, hormones, enzymes, and pharmaceutical preparations. 10 The acridine ester chemiluminescence method has been applied clinically for the detection of MP antibody. The diagnostic kit for MP by chemiluminescence method has been produced in recent years. 11
At this stage, the culture of pathogens for serum or secretions is still the gold standard for diagnosing MP infection, but to perform this assay, high maintenance equipment and specific skillsets of the biomedical staff are required. The extra-long waiting period to get the culture results makes it less efficient to provide the early medication guidance of treating MPP infection. GPA method is one of the most commonly used methods for clinical detection of MP infection, 12 which has a good diagnostic performance. However, the degree of automation of the PA method is low, and it is largely dependent on manual operations, which limits this assay for the large-scale clinical applications. The ELISA has a high degree of automation and is relatively simple and less expensive, but there are more false-positive results, and the diagnostic accuracy is low. AECLIA assay is compatible with large-scale automation, and assay time is also greatly shortened. Compared to the GPA method with more than 3 h assay time, the assay time of AECLIA is only 30 min. This can effectively reduce the overall test report turnaround time and provide patients with a better experience.
In summary, the positive rates of AECLIA, ELISA and GPA assay for the detection of MP antibody are consistent with current epidemiology data and have good consistency. Among them, the AECLIA and the GPA methods have higher similarity. AECLIA is both efficient and accurate and therefore serve as a better option for MPP screening.
Footnotes
Acknowledgements
Y.W. and G.D. contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The studies were approved by the local ethics committee or institutional review boards and in accordance with the Declaration of Helsinki and are consistent with the International Conference on Harmonization-Good Clinical Practices and applicable amendments. All subjects were given informed, signed consent to participate in the study, or in the case of children or deceased, informed written consent was given by the family or guardian.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Shenzhen People’s Hospital, Shenzhen, Guangdong Province, China.