
Abstract
We describe a case of development of painful periostitis deformans in a 39-year-old woman who was receiving long-term voriconazole treatment for Aspergillus infection as a complication of orthotopic liver transplant. Measurement of fluoride levels strongly supports fluorosis to be the mechanism of the voriconazole-induced periostitis deformans and supports the concept that such measurements might be of use in predicting this complication of long-term voriconazole treatment.
Introduction
Voriconazole is a highly fluorinated antifungal agent used as first-line treatment for invasive aspergillosis, and the catabolism of voriconazole can lead to the release of substantial amounts of fluoride. 1 There have been a number of recent reports of fluorosis and subsequent development of painful periostitis deformans and exostoses in patients treated with long-term voriconazole, and here we report a case in which we provide evidence of fluorosis as the mechanism of voriconazole-induced periostitis deformans, as demonstrated by persistent increased serum fluoride concentrations.
Case report
A 39-year-old woman received an orthotopic liver transplant because of Child’s C cirrhosis secondary to autoimmune hepatitis. The post-operative course was complicated with a prolonged intensive care admission, acute kidney injury, biliary leak, early graft rejection and the development of critical-illness polyneuropathy. Approximately six weeks after the initial transplant surgery, aphasia and right hemiplegia developed, and computed tomography imaging revealed ring enhancing lesions consistent with the presence of multiple intracranial abscesses. Aspiration of the abscesses showed the presence of Aspergillus fumigatus, and long-term voriconazole, 400 mg BD, was subsequently commenced, initially in combination with amphotericin B and caspofungin, which were withdrawn after two weeks and two months, respectively: voriconazole continued. Three months after the commencement of voriconazole, she developed bone pain and reduced shoulder and elbow mobility. This was initially thought to be secondary to the critical-illness polyneuropathy; however, plain film imaging showed features consistent with periostitis deformans, with multiple exostoses adjacent to both radial and humeral shafts and lateral aspects of the scapulae (Figure 1(a)). Whole body bone scan showed diffuse cortically based uptake involving the appendicular skeleton and multiple ribs (Figure 1(b)). Together, these features were considered consistent with periostitis deformans, probably secondary to prolonged use of voriconazole. Voriconazole was ceased and the non-fluorinated antifungal agent itraconazole was commenced. Despite concerns regarding the ability of itraconazole to cross the blood–brain barrier, there has been no recurrence of aspergillosis after 18 months.
(a) X-ray image showing heterotopic calcification along the medial surface of the left humeral shaft (dashed arrow) and lateral aspect of scapula (solid arrows). (b) 99mTc methyl diphosphonate bone-scan images. Delayed planar images show intense uptake along the periosteal margins of the scapula bilaterally with diffuse cortically based uptake involving the appendicular skeleton generally as well as multiple ribs posteriorly. Intense uptake involving the greater trochanters of the femurs and the pubic bones is seen.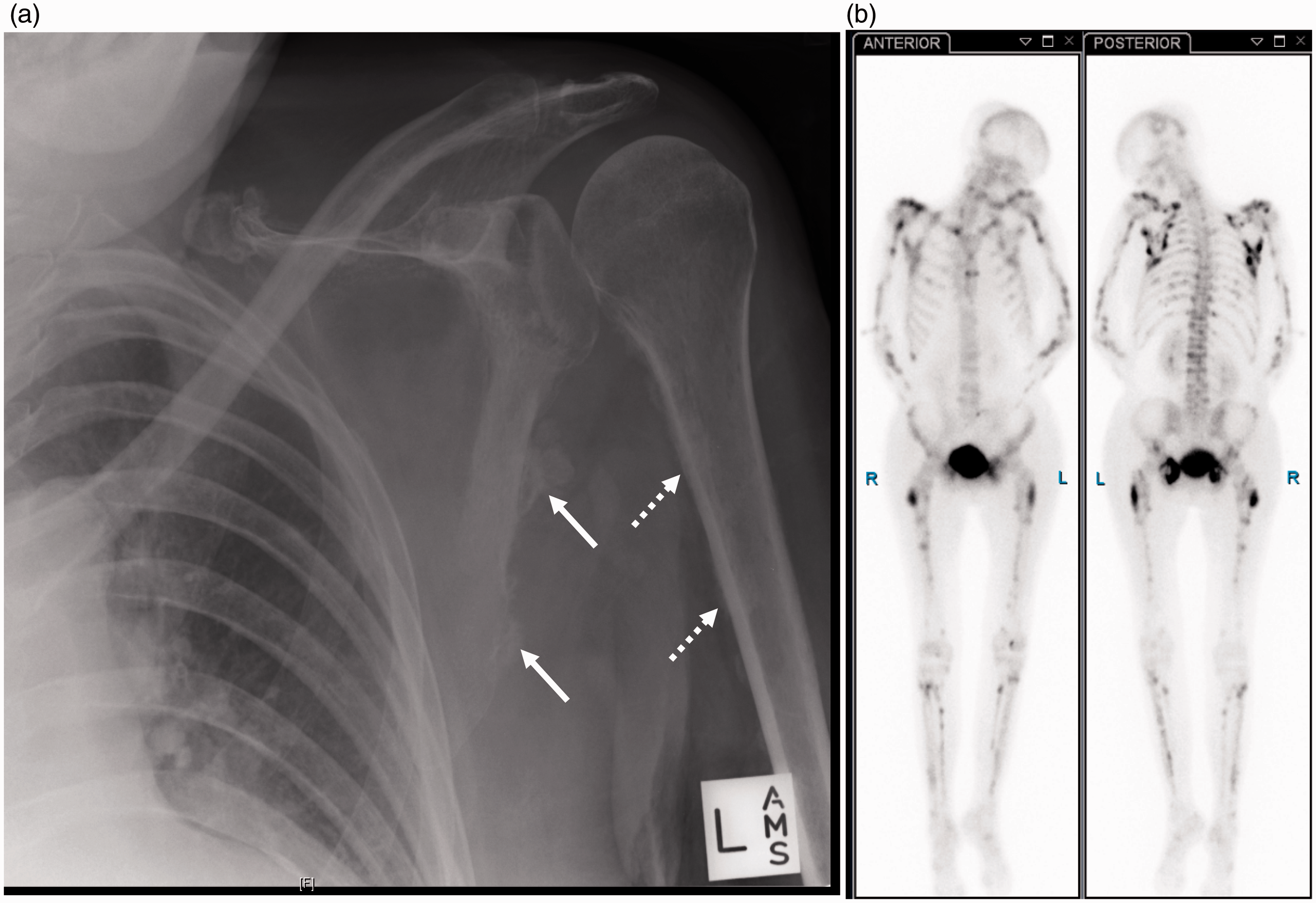
To address the association with voriconazole, serum voriconazole and fluoride concentrations were assayed. Fluoride concentrations were determined using an Orion™ combination fluoride ion-selective electrode attached to a 720A Plus Meter (Thermo Scientific). Serum voriconazole concentrations were measured using a solvent extraction reverse-phase high-performance liquid chromatography method with ultraviolet detection at 260 nm, as modified from the method for the measurement of triazole antifungal agents described by Poirier and Cheymol. 2
Respective fluoride concentrations in samples collected four days before and four, eight and 12 days after ceasing voriconazole were 16.3, 7.9, 8.5 and 6.8 µmol/L (reference interval 0.3–2.2 µmol/L; Figure 2). Voriconazole concentrations were 4.1 and <0.1 mg/L four days before and 10 days after drug cessation (Figure 2). The symptoms of periostitis resolved rapidly after ceasing voriconazole; however, fluoride levels remained elevated at 3.9 µmol/L six months later.
Fluoride and voriconazole levels during and after voriconazole treatment. Voriconazole was ceased on day 0.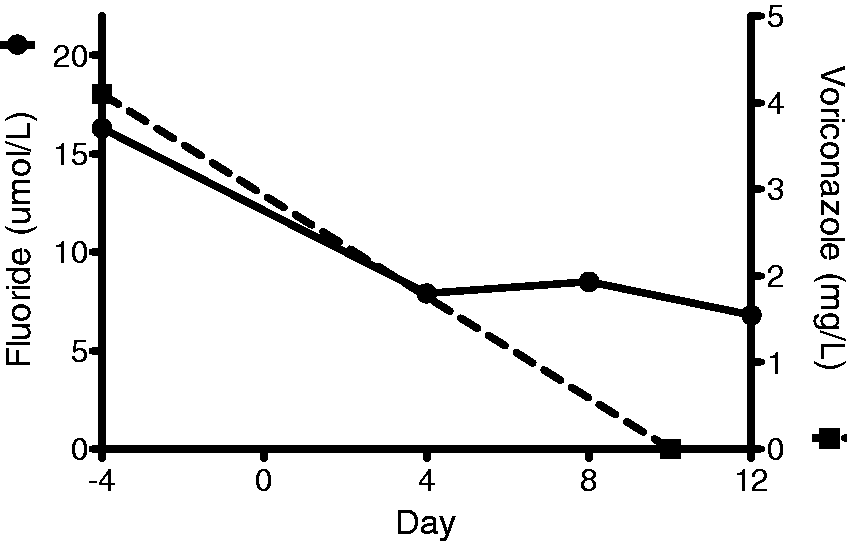
Discussion
Voriconazole is a triazole antifungal agent widely used for prophylaxis of fungal infection in transplant patients and as first-line treatment for invasive aspergillosis. Its structure contains three fluorine atoms, which account for 16.25% of the molecular weight of the drug, and a standard 400 mg dose contains 65 mg of fluorine. The catabolism and excretion of voriconazole involves multiple pathways, and products resulting from oxidative defluorination have been identified. 1
The case described here adds to the record of patients developing skeletal fluorosis and periostitis deformans secondary to voriconazole treatment in the post-transplant setting. Periostitis deformans is a well-described consequence of prolonged exposure to high doses of fluoride, and there have been a number of recent reports of fluorosis and subsequent development of painful periostitis and exostoses in lung,3–5 heart, 3 kidney 3 and bone marrow/stem cell3,6,7 transplant recipients and patients with haematological malignancy5,8 treated with long-term voriconazole. This is the first Australasian case describing this adverse effect of voriconazole and showing a clear clinical effect on cessation of the drug. This case also strongly supports the mechanism of voriconazole-induced periostitis deformans to be due to fluorosis, as evidenced by the increased serum fluoride concentrations.
Fluoride is known to stimulate bone formation, and in periostitis, new periosteal bone growth occurs, which can lead to elevations from baseline in serum alkaline phosphatase (ALP) and other markers of bone remodelling.3,5–10 Regular ALP measurements were performed on this patient throughout the post-transplant period, including during the time of development of bone pain, and ALP activity was elevated throughout and varied widely. However, interpretation of these results was complicated by concurrent elevations in gamma-glutamyl transferase activity along with vitamin D deficiency. ALP isoenzyme fractionation was performed, which showed elevation of both bone and liver fractions, but the vitamin D deficiency made it impossible to attribute the increased bone fraction to the periostitis alone.
In most previously described cases, periostitis and exostoses predominantly developed after six or more months of voriconazole treatment, and the case series described by Moon et al. 9 shows that fluoride levels reflect cumulative voriconazole dose and predict the development of periostitis. However, a case report from Becce et al. 10 describes development of fluorosis and periostitis within six weeks of the introduction of voriconazole. This suggests that all patients receiving voriconazole are at risk, regardless of the duration of treatment.
As seen in this case, and described elsewhere, fluoride levels persist after withdrawal of voriconazole, despite symptom resolution,3,6 which suggests that the fluoride is sequestered in, and slowly released from, the skeleton. It has been suggested that intermittent treatment with recombinant parathyroid hormone (teriparatide) to increase bone turnover might assist with removal of skeletal fluoride 11 ; however, the need for such treatment in the absence of symptoms is unclear.
Interestingly, the difluoronated triazole antifungal agents fluconazole and posaconazole have not been associated with periostitis. The fluoride levels recorded in two small cohorts of patients receiving these agents were much lower than those seen in patients receiving voriconazole.3,6,12 Therefore, these agents might provide a safer alternative to voriconazole as first-line treatment when good penetration of the blood–brain barrier is required.
Various medical practitioners including infectious diseases specialists, transplant physicians and importantly general practitioners in the community may care for patients on long-term voriconazole. Clinicians should be aware that skeletal fluorosis and painful periostitis deformans can complicate long-term treatment with voriconazole. Should symptoms of periostitis develop, investigations such as skeletal imaging and measurement of serum fluoride levels should be performed and if periostitis deformans is confirmed, clinicians should have a low threshold for reducing or ceasing voriconazole if clinically possible. In addition, the measurement of serum fluoride levels can assist in predicting development of periostitis and although symptoms typically resolve with withdrawal of voriconazole, elevated serum fluoride levels can persist.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-to-profit sectors.
Ethical approval
The patient has given written informed consent for publication.
Guarantor
WR.
Contributorship
BR and DG provided clinical care of the patient. MS, PC and WR coordinated investigations. SG and CF performed the fluoride assays. WR and BR reviewed the literature and MB wrote the first draft of the paper. All authors reviewed and edited the manuscript and approved the final version of the manuscript.