
Abstract
Background
A new formula was recently proposed by Cordovo et al. that was more highly correlated with low-density lipoprotein (LDL) measured directly than the Friedewald LDL formula. We conducted this prospective study to establish whether the new formula allows true variations in LDL within the same individual to be tracked more closely than that of the Friedewald formula.
Methods
A cross-over study of biological variation of lipids in 26 patients with Type 2 diabetes (T2DM) taking either a short half-life statin, simvastatin 40 mg (n = 10), or a long half-life statin, atorvastatin 10 mg. After three months on one statin, fasting lipids were measured on 10 occasions over a five-week period. The same procedure was then followed for the other statin. The LDL was measured by a direct LDL immunoassay and was compared to the LDL estimated by the Friedewald and Cordova (0.7516) × (total cholesterol [TC]−high-density lipoprotein cholesterol [HDL-C]) formulae.
Results
As a group, the calculated or measured mean LDL was no different between statins. However, the biological coefficient of variation (CV) of directly measured LDL was far larger with simvastatin than atorvastatin. This difference was detected by Cordova LDL but not found with the Friedewald LDL formula.
Conclusions
In contrast to Friedewald LDL, Cordova LDL estimation revealed LDL to be much more stable in T2DM patients taking atorvastatin rather than simvastatin that was in accord with LDL when measured directly. Therefore, Cordova LDL which is a measure of non-HDL-cholesterol is the simplest, cheapest and the most convenient measurement for assessment of response to statin treatment.
Keywords
Introduction
Low-density lipoprotein cholesterol (LDL-C) is a major lipid parameter in cardiovascular risk assessment. The Friedewald formula is widely used for estimating LDL-C but has known limitations, including its use in patients with Type 2 diabetes (T2DM). More recently, a simpler formula has been proposed to estimate LDL-C with higher accuracy and simplicity for general clinical use as well as have a higher correlation with directly measured LDL-C (Cordova LDL-C). 1 Using an immunoassay to directly measure LDL-C, we have shown that the biological coefficient of variation (CV) of directly measured LDL-C in T2DM patients was far larger with simvastatin than with atorvastatin even though the mean value of LDL-C achieved by individuals taking simvastatin 40 mg was not inferior to that of atorvastatin 10 mg. 2 In contrast, there were no significant differences in this biological variability between atorvastatin and simvastatin when Friedewald’s formula was used, 3 which may in part be because Friedewald LDL-C is known to be less reliable in patients with Type 2 diabetes. The current study was undertaken to see if the biological variation of calculated LDL-C using Cordova’s formula was closer to that of directly measured LDL-C than of the Friedewald LDL-C formula.
A cross-over study of biological variation of lipids in 26 patients with T2DM taking either a short half-life statin, simvastatin 40 mg (n = 10), or a long half-life statin, atorvastatin 10 mg. After three months on one statin, fasting lipids were measured on 10 occasions over a five-week period. 3 The same procedure was then followed with the other statin. The LDL-C was estimated by the Friedewald and Cordova (0.7516) × (total cholesterol [TC]−high-density lipoprotein cholesterol [HDL-C]) formulae, and measured by a direct LDL-C immunoassay. The direct LDL was measured using a Synchron DxC analyser (Beckman-Coulter, High Wycombe, UK). The sensitivity for the direct LDL assay was <8 mg/dL (<0.21 mmol/L).
Within-patient biological variability of LDL-C was calculated by subtracting the analytical variance (estimated from duplicate samples) from the within-subject variance. 4
Results
The baseline demographics, duration of diabetes and glycaemic control were comparable in both groups.
3
The (mean ± standard deviation [SD]) calculated LDL-C concentration using Cordova’s formula on atorvastatin 10 mg was no different than when taking simvastatin 40 mg (2.21 ± 0.15 mmol/L vs. 2.12 ± 0.25, respectively, P = 0.52 using an unpaired t-test), confirming that the simvastatin and atorvastatin drug dosages were equivalent. In contrast, the variability of estimated LDL-C using Cordova’s formula, expressed as SD, was lower on atorvastatin (average SD ± standard error of mean [SEM]) (0.15 ± 0.02 mmol/L) than on simvastatin (0.25 ± 0.04 mmol/L; P = 0.02) (Figure 1). This equated to a CV of 6.78% for atorvastatin and 11.83% for simvastatin for estimated LDL-C using Cordova’s formula. This was less than the CV of 10.30% for atorvastatin and 13.10 for simvastatin for LDL-C calculated using Friedwald’s formula. On the other hand, the variability in direct LDL-C, expressed as SD, was much lower on atorvastatin (average SD ± SEM) (0.01 ± 0.003 mmol/L) than on simvastatin (0.17 ± 0.02 mmol/L, P < 0.0001) when direct LDL-C was used.
Means (range) of Cordova calculated LDL-C in the same patients taking either simvastatin 40 mg or atorvastatin 10 mg daily.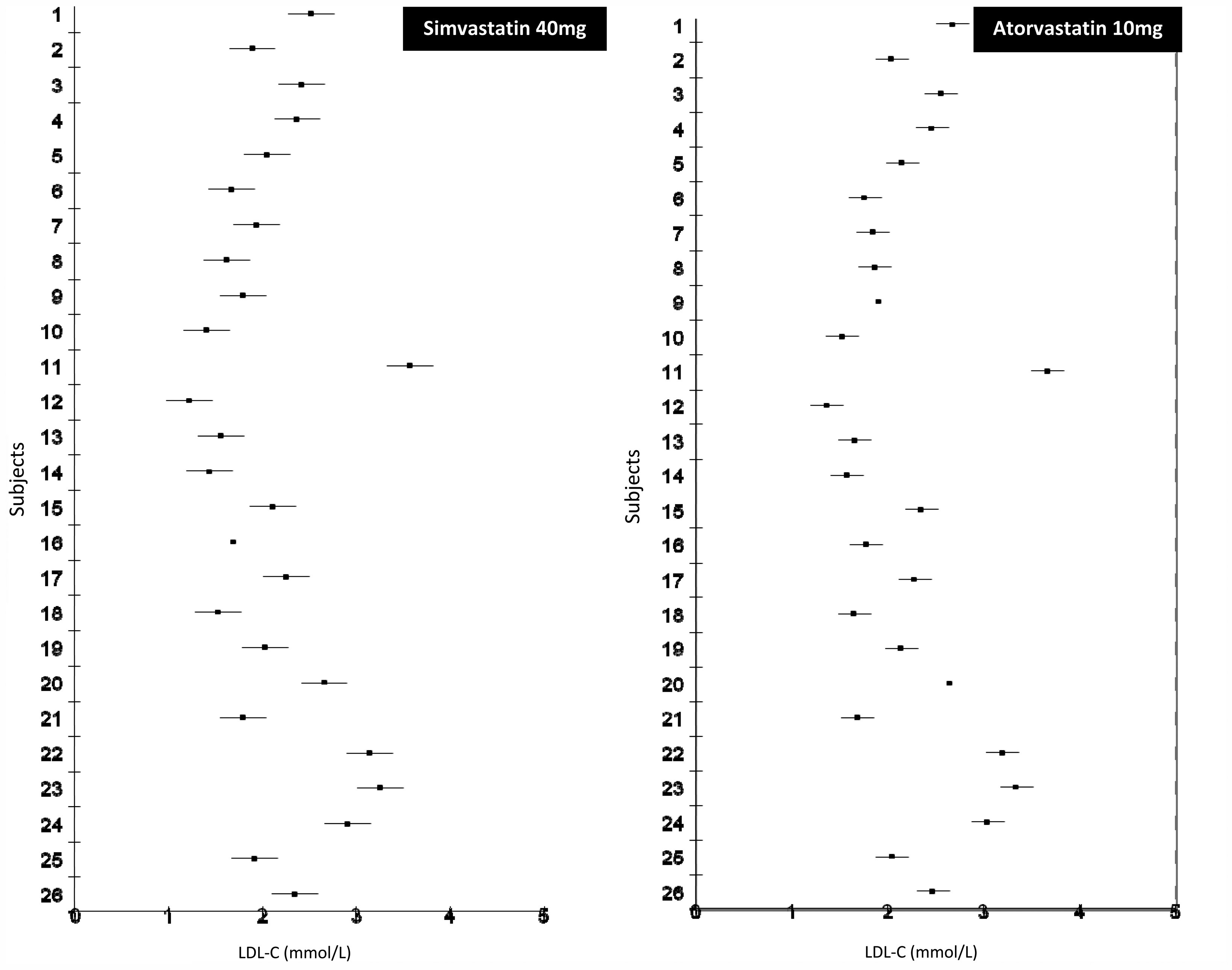
Conclusion
This study has shown that the biological variability of LDL-C cholesterol when measured using Cordova’s formula was significantly lower while taking atorvastatin 10 mg compared to simvastatin 40 mg daily, despite the mean LDL-C values on both treatments being the same. This pattern is consistent with the biological variability of LDL-C measured using direct LDL-C measurement. 2
These findings contrast with the biological variability we found when LDL-C was calculated using the Friedewald equation on the same samples. Although useful in most cases, Friedewald’s formula applies poorly to a number of atypical situations, such as extremes of triglyceride (TG) and TC values as well as in patients with Type 2 diabetes. In addition, the Corvodo’s formula also has the advantage of not requiring a fasting blood sample as it has been demonstrated that a regular fasting period does not significantly interfere with TC and HDL-C determination.
The greater improvement seen when Cordova’s formula is applied to the atorvastatin data could be the reflection of greater CV of triglyceride on atorvastatin. The key difference between the formulas of Friedewald and Cordova is that the triglyceride level is factored into the former but not the latter. The CV of triglycerides on simvastatin was 12.06%, whereas the CV on atorvastatin was 19.71%. When compared to ultracentrifugation, which is the gold standard, LDL-C calculated by Cordova’s formula did not perform well. 5 However, the most useful additional observation would be that non-fasting non-HDL-cholesterol is the simplest, cheapest and the most convenient measurement for assessment of response to statin treatment and is recommended in preference to LDL cholesterol as the goal for lipid lowering therapy by the recent Joint British Societies’ consensus recommendations for the prevention of cardiovascular disease guidelines. 6
In summary, this study has found marked differences in the biological variability of Cordova LDL-C when taking simvastatin compared to atorvastatin that is in accord with directly measured LDL-C. This is in contrast to the lack of a difference found when calculating LDL-C using Friedewald’s formula. While it is unknown whether the increased variability of LDL-C on simvastatin can influence cardiovascular risk, it has direct implications on maintaining an LDL-C concentration below target that will be more effectively achieved using longer half-life treatments such as atorvastatin. These findings suggest that using the Cordova formula to estimate LDL measurement has a potential clinical advantage over LDL calculated using the Friedewald formula when used in patients with T2DM taking statin treatment.
Footnotes
Declaration of conflicting interests
None declared.
Funding
The study was partially funded by an unrestricted educational grant from Pfizer.
Ethical approval
South Humber Local Research Ethics Committee (ref: 04/Q1105/40).
Guarantor
ESK.
Contributorship
ESK, SLA and TS are involved in conceiving, conducting, analysing and drafting the manuscript.