
Abstract
Background
The inhibition of glycolysis prior to glucose measurement is an important consideration when interpreting glucose tolerance tests. This is particularly important in gestational diabetes mellitus where prompt diagnosis and treatment is essential. A study was planned to investigate the effect of preservatives and temperature on glycolysis.
Methods
Blood samples for glucose were obtained from consented females. Lithium heparin and fluoride-EDTA samples transported rapidly in ice slurry to the laboratory were analysed for glucose concentration and then held either in ice slurry or at room temperature for varying time intervals. Paired fluoride-citrate samples were received at room temperature and held at room temperature, with analysis at similar time intervals.
Results
No significant difference was noted between mean glucose concentrations when comparing different sample types received in ice slurry. The mean glucose concentrations decreased significantly for both sets of samples when held at room temperature (0.4 mmol/L) and in ice slurry (0.2 mmol/L). A review of patient glucose tolerance tests reported in our hospital indicated that 17.8% exceeded the recommended diagnostic criteria for gestational diabetes mellitus. It was predicted that if the results of fasting samples were revised to reflect the effect of glycolysis at room temperature, the adjusted diagnostic rate could increase to 35.3%.
Conclusion
Preanalytical handling of blood samples for glucose analysis is vital. Fluoride-EDTA is an imperfect antiglycolytic, even when the samples are transported and analysed rapidly provides such optimal conditions. The use of fluoride-citrate tubes may offer a viable alternative in the diagnosis of diabetes mellitus.
Introduction
Accurate diagnosis of gestational diabetes mellitus (GDM) remains dependant on the results of an oral glucose tolerance test (OGTT) using limits recommended by international bodies, such as the International Association of Diabetes and Pregnancy Study Groups 1 (IADPSG). Guidance from the IADPSG is based on data obtained from the Hyperglycaemia and Adverse Pregnancy Outcomes (HAPO) study. 2
The HAPO study used standardized sample collection criteria – fluoride oxalate in ice slurry – across its many study centres. The OGTT comprises three glucose samples taken at 0, 1 and 2 h after a 75 g glucose load. It is reported that despite the use of fluoride as an antiglycolytic agent, glycolysis continues in blood samples after collection. 3 If samples are held together as a set prior to analysis, a delay in receipt and analysis may affect the reported results of the first sample more than the last.
Accurate GDM diagnosis and risk stratification require the use of accurate measurement of properly stabilized samples for the measurement of glucose.4,5 This is particularly important in antenatal and postnatal clinics, where there is a limited timeframe in which GDM is diagnosed and treatment initiated.
The National Academy of Clinical Biochemistry guidelines 6 recognizes the importance of preventing in vitro glycolysis due to its effects on diagnosis. The guidance recommends either transport of the sample in ice and separation from blood cells (within 30 min) or the use of an antiglycolytic agent such as citrate buffer.
The aim of the study is to investigate the effect of preservatives and ice as glycolytic inhibitors over the time period normally experienced in the hospital setting, as well as its effect of on the diagnosis of GDM.
Materials and methods
Venous blood for glucose analysis was obtained from 200 pregnant females with consent. The study was approved by the Hospital Research Ethics Committee.
Blood was drawn from each subject at intervals during their pregnancy (12 weeks, 24–28 weeks and 36 weeks) and six weeks postnatal into a fluoride-EDTA tube (Sarstedt 05.1073.001; Sarstedt, Numbrecht, Germany). All fluoride-EDTA samples were placed in an ice-water slurry for transport to the laboratory.
Blood samples were drawn from a random subgroup of this cohort into lithium heparin tubes (Sarstedt 05.1553.001), and held either in ice-water slurry or at room temperature during transport to the laboratory. These samples were paired to the fluoride-EDTA samples transported in ice-water slurry.
Blood samples were drawn from a random subgroup of this cohort into citrate-EDTA tubes (Sarstedt 05.1074.001) and paired to the fluoride-EDTA samples which were being transported in ice-water slurry. The citrate-EDTA samples were transported to the laboratory at room temperature.
Glucose concentration measurements were performed in a laboratory, accredited to ISO 15189, on a Beckman Coulter AU640 (Beckman Coulter Inc., Brea, CA, USA) automated chemistry analyser. Analytical imprecision (standard deviation) was 1.64% (0.09 mmol/L) at glucose concentration 5.46 mmol/L.
Statistical analysis, using Bland–Altman analysis to compare paired results, was performed using Analyse-It software for Microsoft Excel (Analyse-It Software Ltd, Leeds, UK).
Study design
The time of receipt of samples to the central laboratory was measured.
The results of two cohorts of patients were examined, and the diagnostic rates of GDM were calculated using these results against the HAPO criteria.
Paired samples were received, and the transport time from phlebotomy was recorded for each sample. Paired samples received within 30 min were separated and analysed after aliquots were removed. The aliquots were held for specified times and temperatures before separation and analysis (Figure 1).
Flow chart for sample analysis; fluoride-EDTA and lithium heparin samples.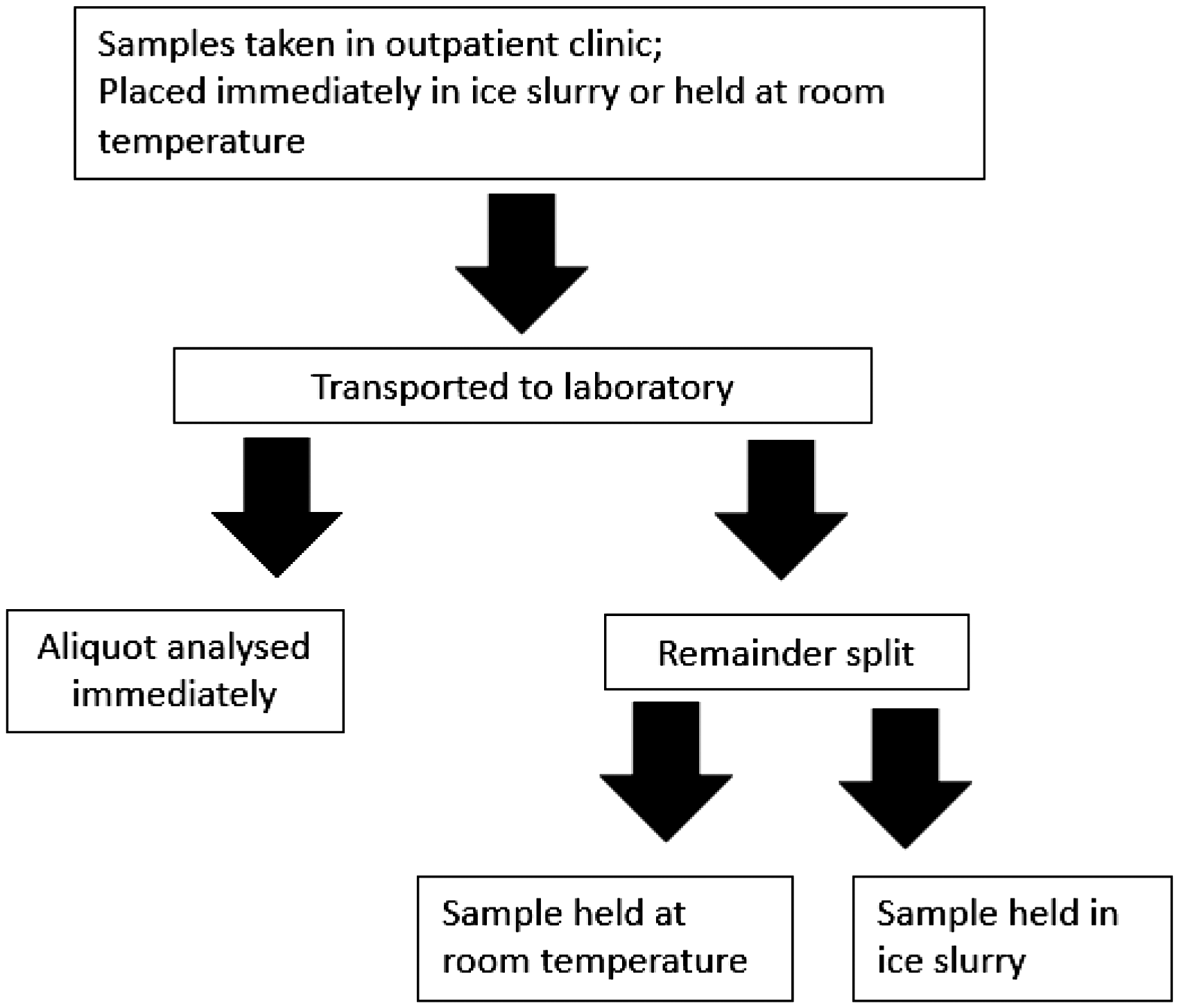
The difference in glucose concentration between samples held on ice and room temperature for different time intervals was calculated.
The standard against which other preservatives and conditions were compared was the glucose concentration reported in samples of fluoride-EDTA preservative which were received on ice.
The difference in mean glucose concentrations were analysed using Student’s t-test.
To investigate the effect of temperature and/or preservative on glycolysis, the glucose concentration at time of receipt was compared for paired samples.
Fluoride-EDTA on ice; lithium heparin on ice. Fluoride-EDTA on ice; lithium heparin received at room temperature. Fluoride-EDTA on ice; citrate-EDTA received at room temperature.
To investigate the effectiveness of preservatives on glucose over time, the glucose concentration was measured at various time intervals within the time period determined by the findings of transport time to the laboratory (Figure 2).
Samples (fluoride-EDTA and lithium heparin) were held on ice or room temperature for 2.5 h before separation and glucose measurement. Samples (fluoride-EDTA and lithium heparin) were held on ice or room temperature for up to 90 min with separation and glucose measurement of aliquots at 15-min intervals. Samples were held on ice (fluoride-EDTA) or room temperature (citrate-EDTA) for up to 90 min with separation and glucose measurement of aliquots at 15-min intervals.
Results
The mean time taken for samples from glucose tolerance test series to be received into the laboratory was 154 min (range: 123–190 min). Based on these findings, the time used to delay the analysis of samples was chosen to be 150 min (2.5 h).
Difference in glucose concentration at time of receipt between different preservatives transported at differing temperatures.
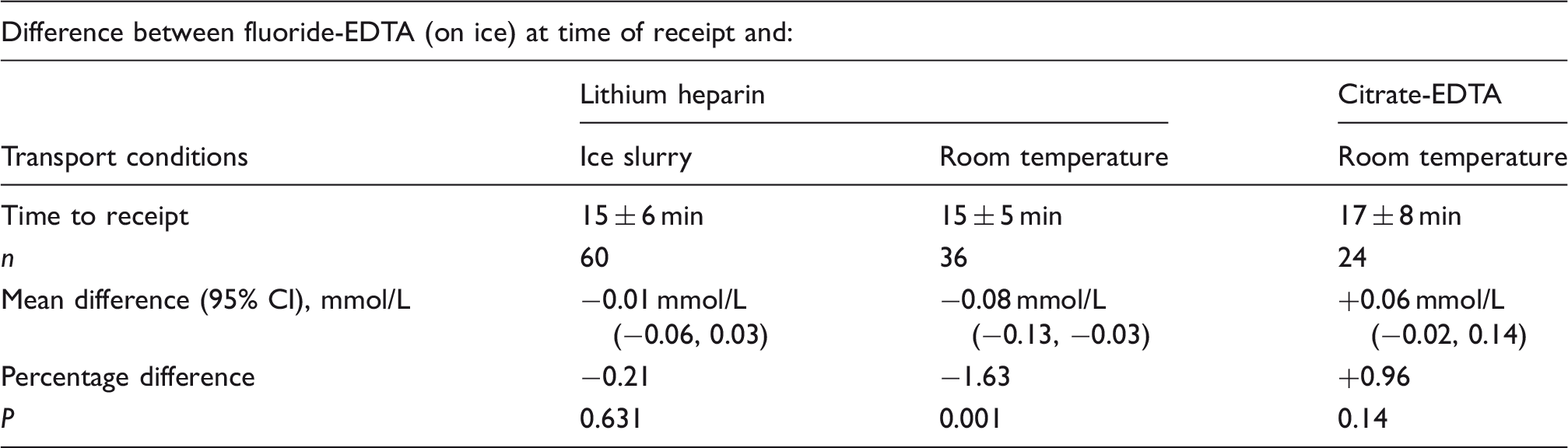
There was a significant difference between mean glucose concentrations when received in either fluoride-EDTA or citrate-EDTA preservative type. Mean glucose concentration in the citrate-EDTA set was greater than that seen in the fluoride-EDTA samples (Table 1).
Aliquots of paired fluoride-EDTA and lithium heparin samples were incubated for 2.5 h at two different temperatures: room temperature and ice slurry.
Difference in glucose concentration when held for 2.5 h.
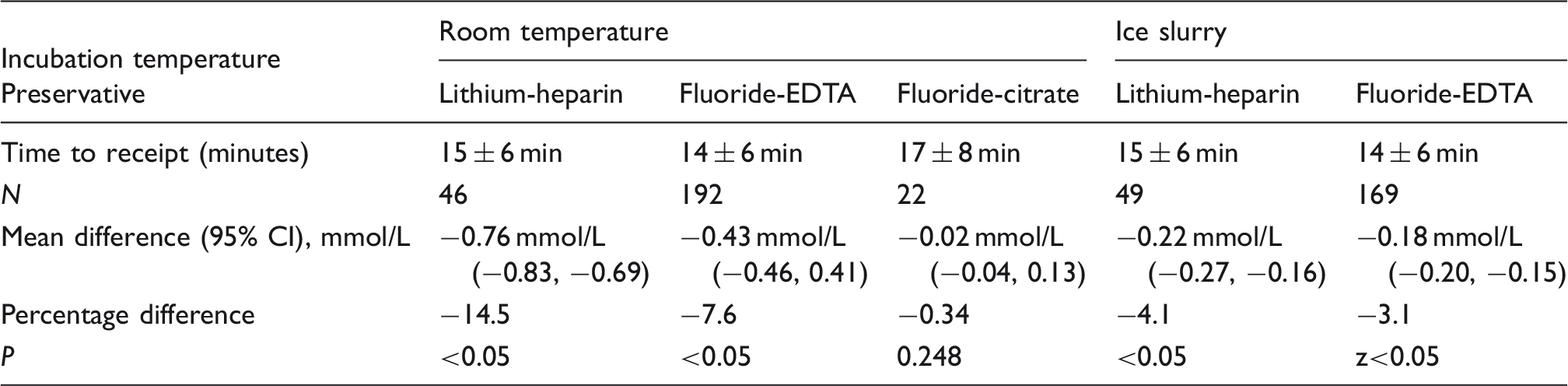
Note: Three preservative types are compared.
The rates of glycolysis within each preservative type at either room temperature or in ice slurry were compared for paired samples (n = 23). Differences in glucose concentrations measured at the time of receipt and time points chosen for analysis were compared (Figures 3 and 4).
Flow chart for sample analysis. Fluoride-citrate samples. Samples analysed at 15-min intervals: Fluoride-EDTA and lithium heparin. Samples analysed at 15-min intervals: Fluoride-EDTA and fluoride-citrate.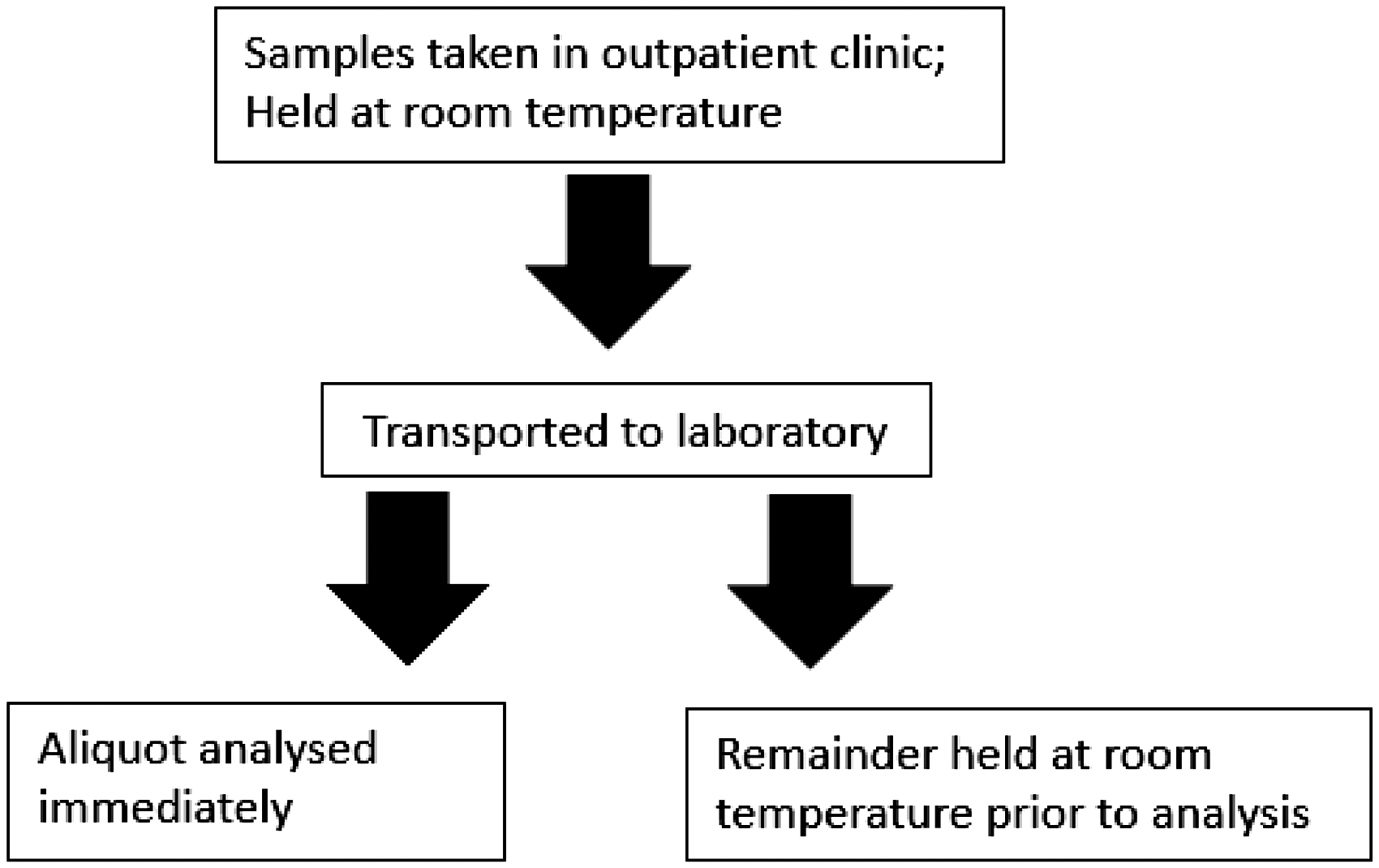
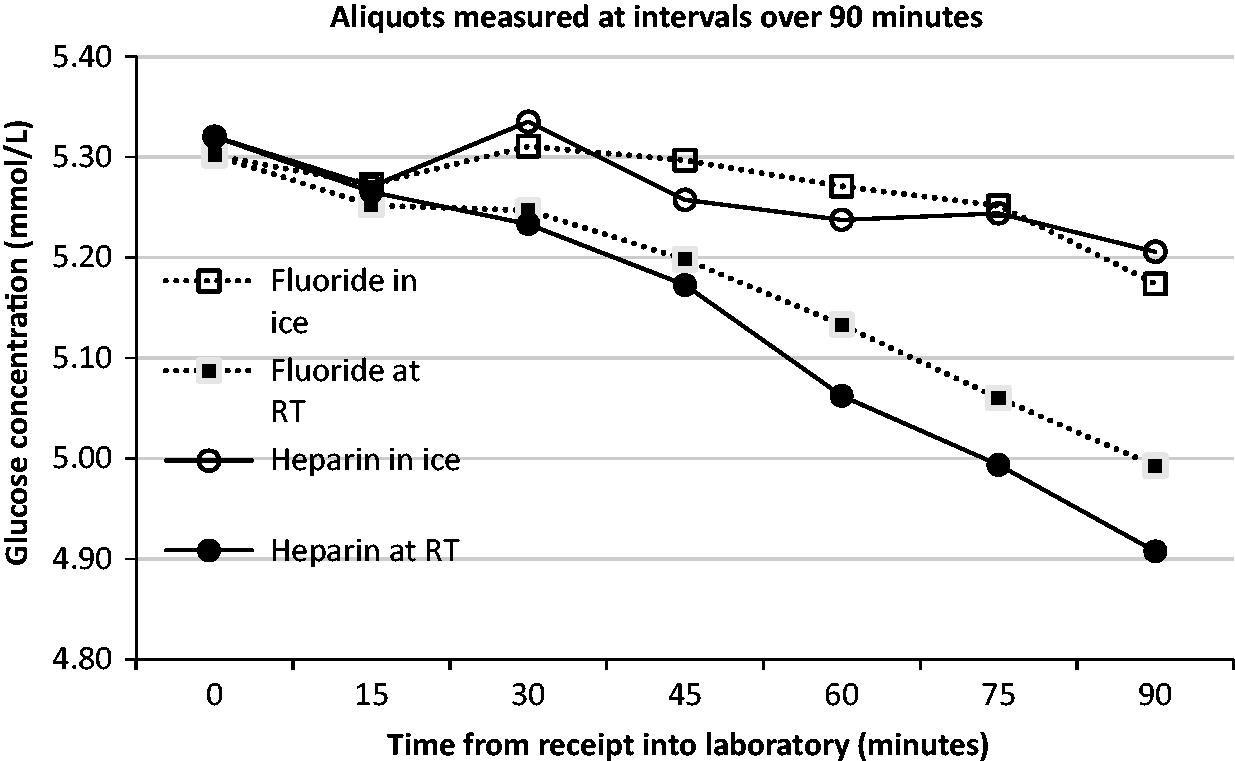
For paired fluoride-EDTA and Lithium heparin samples (n = 23), the differences in glucose concentration between t = 0 and samples held at room temperature were statistically significant at every time point.
The differences in glucose concentration between t = 0 and samples held in ice slurry were statistically significant at every time point for lithium heparin samples.
The differences in glucose concentration between t = 0 and samples held in ice slurry were statistically significant for time points after 30 min for fluoride-EDTA samples.
The change in glucose concentration between preservative types at the same environmental conditions was also compared. The rate of change was similar between sample types if held at the same temperature. However, there was a significant difference between rates after an hour for samples held at room temperature.
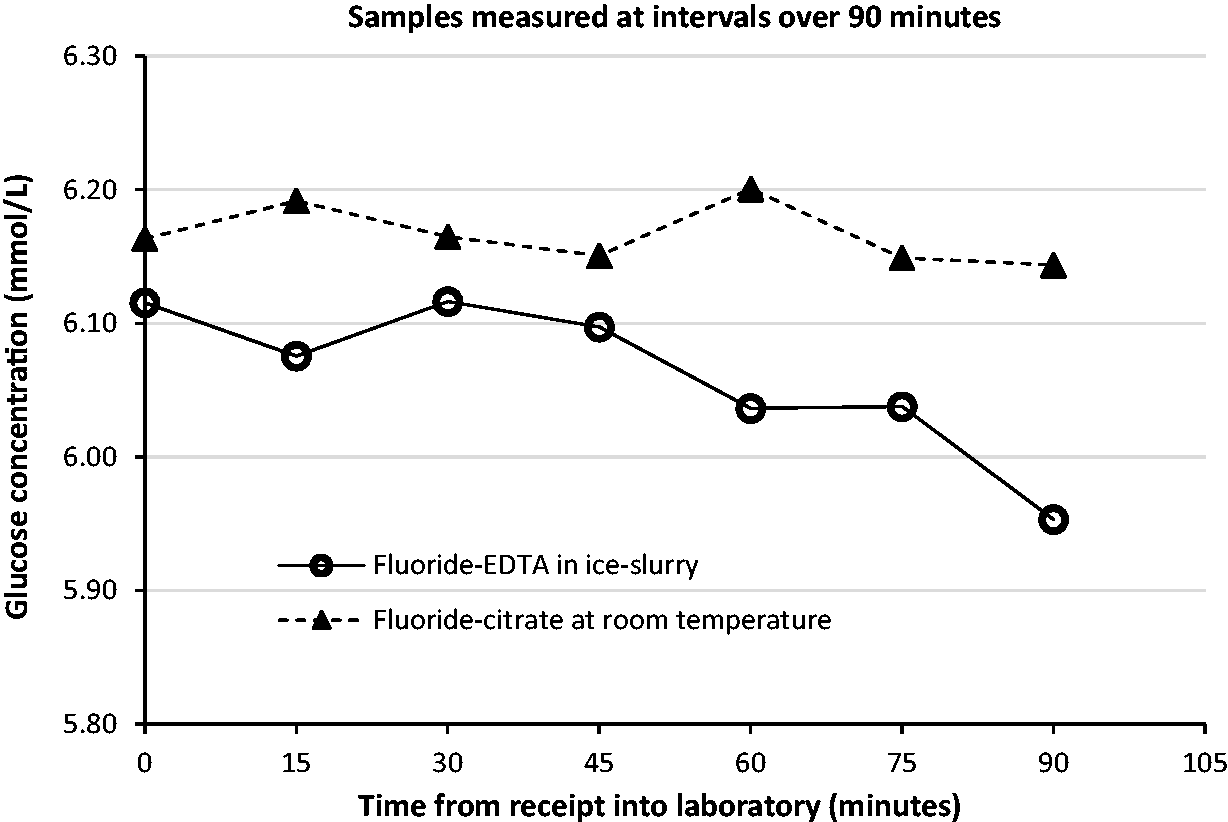
The changes in mean glucose concentration between paired samples of fluoride-EDTA held on ice and fluoride-citrate samples held at room temperature were examined (Figure 4). A difference in mean glucose concentration is noticeable, with a significant difference in fluoride-EDTA samples noted at 15 min postreceipt. While reviewing data from the fluoride-citrate tubes, it was noted that there was no significant difference between the mean glucose concentration at the time of receipt and at any of the time points investigated.
A review of 400 patient glucose tolerance tests reported in an outpatient clinic in our hospital indicated that 17.8% were reported as fulfilling the recommended diagnostic criteria for GDM in one or more samples. Of a sample of 113 patients’ glucose tolerance tests sampled at a clinic located 30 km from the hospital (external clinic), 10.6% were reported as exceeding the recommended diagnostic criteria for GDM in one or more samples.
It was predicted that if the results of fasting samples were reviewed to include or incorporate the difference due to glycolysis in fluoride tubes at room temperatures as calculated in this study (0.4 mmol/L), the revised diagnostic rate would be 35.3% of the females chosen for selective screening in the outpatient clinic. For samples taken in the external clinic, this value could be added to all patient results, due to the increased delay in sample receipt. It is predicted the revised diagnostic rate would be 38.1% of these females chosen for selective screening.
Discussion
The diagnostic limits derived from the HAPO study were based on samples collected and transported in ice-slurry, and separated within 1 h. To obtain accurate diagnosis using these limits, the methods of glycolysis inhibition when analysing glucose samples in antenatal OGTTs ought to mirror those used in the study. 7
It is shown that if there is rapid transport of samples prior to separation and analysis, there is little difference in glucose concentrations reported when paired samples are transported on ice, even in the absence of fluoride-EDTA preservative.
When comparing average glucose concentrations of samples received and analysed rapidly (within 30 min) in fluoride-EDTA to fluoride-citrate preservatives, a positive bias of mean glucose concentration is observed for fluoride-citrate samples. This bias may be due to ongoing glycolysis in the fluoride-EDTA tubes due to delayed cooling of the blood in the tubes. 8 Alternatively, it has been proposed that the conversion factor used for liquid preservative may require revision. 9
When investigating a delay of 2.5 h for samples held at room temperature – the time taken for samples to reach the laboratory – it can be seen that the 7.6% (0.4 mmol/L) decrease seen in the fluoride-EDTA samples is consistent with previous reports, while that of the lithium heparin nears 15% (0.8 mmol/L). The difference in glucose concentration calculated from samples of citrate preservative is negligible over the 2.5 h.
In the unlikely event that samples would be held for extended periods of time in ice slurry, it is shown that a significant difference is seen at 2.5 h for samples containing the fluoride-EDTA preservative. At a 3% (0.2 mmol/L) decrease from the original analysis, this decrease is similar to that seen in the lithium heparin samples (4%; 0.2 mmol/L). The ice therefore appears to have an incomplete effect in inhibiting the glycolytic process. This is in contrast with the consistency in mean glucose concentration noted in the fluoride-citrate samples over the same time period. Indeed, over a longer time period – 4 h – there is negligible difference (0.28%) in mean glucose concentration measured in fluoride-citrate tubes.
When results from delayed analysis using shorter timeframes are examined, it may be seen that even at a short an interval as 15 min, there is a significant change in glucose concentration for paired samples held either at room temperature or for samples held on ice. This consistent change is not seen in samples preserved using fluoride-citrate.
Although the rates of change are similar across time points, there is a slight variability in average glucose concentration at each time point. This may be due to the small sample size of the study.
Transporting every glucose sample individually on ice prior to analysis is not a viable option for hospitals and clinics. A possible alternative is the use of fluoride-citrate preservative for glucose analysis.10,11
The recommendation of citrate as an antiglycolytic agent has been popularized recently, due its reemergence as a viable glycolytic inhibitor.6,10,12,13
Sample tubes containing either powdered or liquid preservative have been studied, and the results are compared against the traditional fluoride glucose tubes. 14
Due to the dilution of the sample by the liquid preservative, a correction factor is required for samples, the published values of which have come under scrutiny. The difference between the mean glucose concentrations reported in fluoride when held on ice and those reported in citrate tubes using a liquid preservative have been sufficiently similar to allow their introduction. However, this consistent difference was investigated and has been reported as due to the manufacturer’s recommended correction factor. 9
Conclusion
This study investigated the effect of fluoride, citrate and ice as glycolytic inhibitors over the time period normally experienced in the hospital setting.
The importance of an early and accurate diabetes diagnosis, including GDM by the stringent HAPO criteria, is such that health professionals cannot overlook the impact of glycolysis. By diagnosing using HAPO criteria, and not adhering to the collection practices in the study, it is likely that there is consistent underdiagnosis of GDM in our patient population.
Optimal preanalytical standardized conditions are critical for the accurate classification of diabetes, particularly GDM, where the window for diagnosis is limited and the treatment is immediate. Where the findings in our paper are important in all investigations of patients for diabetes mellitus and impaired glucose tolerance, the lack of diagnostic utility of HBA1c in the setting of GDM, makes defining the evidence base for preanalytical criteria for the GTT critical.
Footnotes
Acknowledgements
The authors wish to acknowledge the support of staff in the biochemistry laboratory throughout this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of the Coombe Women and Infants University Hospital approved the study (study no. 26-2011).
Guarantor
ROK.
Contributorship
MS and ROK researched literature, conceived the study. ND and MT obtained ethical approval. ND recruited patients. MS wrote the first draft of the manuscript. All authors reviewed the manuscript and approved the final version.