
Abstract
Background
Few studies have reported the characterization of postnatal serum concentrations of endogenous free fatty acids (FFAs) in high-risk newborns and their effects on unbound bilirubin (UB).
Methods
Serum concentrations of FFA, albumin (Alb), UB and total bilirubin (TB) were measured in 713 samples obtained within 5 days after birth from 439 newborns without intravenous lipid supplementation admitted to the neonatal intensive care unit (NICU). Serum FFA was reported as the day-specific percentile-based curve. Serum FFA and FFA/Alb ratios were compared in term and preterm patients. To assess the impact of FFA on UB, daily changes in FFA/Alb and UB/TB ratios were compared in term patients without receiving phototherapy or any drugs, and linear regression analysis was performed between FFA/Alb ratio and serum UB concentration or UB/TB ratio using 140 sera with hyperbilirubinemia of term and preterm patients.
Results
A percentile-based curve showed that serum FFA peaked at 1 day of age and progressively decreased. Serum FFA and the FFA/Alb ratio were significantly higher in term than in preterm patients at birth and 1 and 3 days of age. FFA/Alb ratio significantly changed over 5 days after birth, but UB/TB ratio remained constant. FFA/Alb ratio did not correlate with serum UB concentration or UB/TB ratio in sera with hyperbilirubinemia.
Conclusions
We assessed postnatal concentrations of serum FFA in a large number of high-risk newborns admitted to the NICU. The concentration of endogenous FFAs in newborns admitted to the NICU was not rising until it influenced UB.
Background
Serum concentrations of unbound bilirubin (UB), which is bilirubin not bound to albumin (Alb), have been suggested to identify more strongly than serum total bilirubin (TB) levels alone, with those infants at risk for developing bilirubin-induced neurologic dysfunction such as acute bilirubin encephalopathy and its sequelae, kernicterus.1–5 Serum UB concentrations depend not only on serum TB and Alb concentrations, but on the bilirubin–albumin binding affinity and the presence of displacers like free fatty acids (FFAs).6–10
FFAs affect bilirubin–albumin binding. Briefly, Alb contains a primary high-affinity site for bilirubin and a secondary low-affinity site. FFAs preferentially bind to Alb at its high-affinity site; if unavailable, FFAs can displace bilirubin from its high-affinity site, resulting in its transport to the secondary, low affinity site. 11 Aromatic anions, in turn, can displace bilirubin from its secondary site on Alb, thereby increasing the serum concentrations of UB.11,12 Indeed, intralipid therapy, which increases serum FFA concentrations, also increases serum UB concentrations in premature newborns of gestational age (GA) ≤ 28 weeks.9,10
Serum FFAs can be increased not only by exogenous lipid emulsions, but by endogenous fasting and stress conditions.13–16 The neonatal intensive care unit (NICU) admits sick newborns, including those with asphyxia and respiratory diseases, with stress during the early postnatal period. Despite their being under the care of neonatologists, standard serum FFA curves are not available for these populations. Newborns with high serum FFA concentrations should be closely monitored for the occurrence and treatment of neonatal hyperbilirubinemia. The objectives of this study were to characterize postnatal serum concentrations of endogenous FFA in high-risk newborns with various diseases admitted to the NICU and investigate the impact of endogenous FFA on UB during the early postnatal period.
Methods
Setting
The NICU in Kobe University Hospital, Japan, includes 9 beds for level III intensive care and 15 beds for level II transitional care, with over 400 newborns admitted annually. The NICU accepts newborn patients born in Kobe University Hospital from women with complicated pregnancies, and sick or premature newborns born in general hospitals or clinics in the surrounding area. Patients admitted to the NICU include those requiring intensive care treatments, including surgery and inhaled nitric oxide.
Study methods
Patient characteristics.
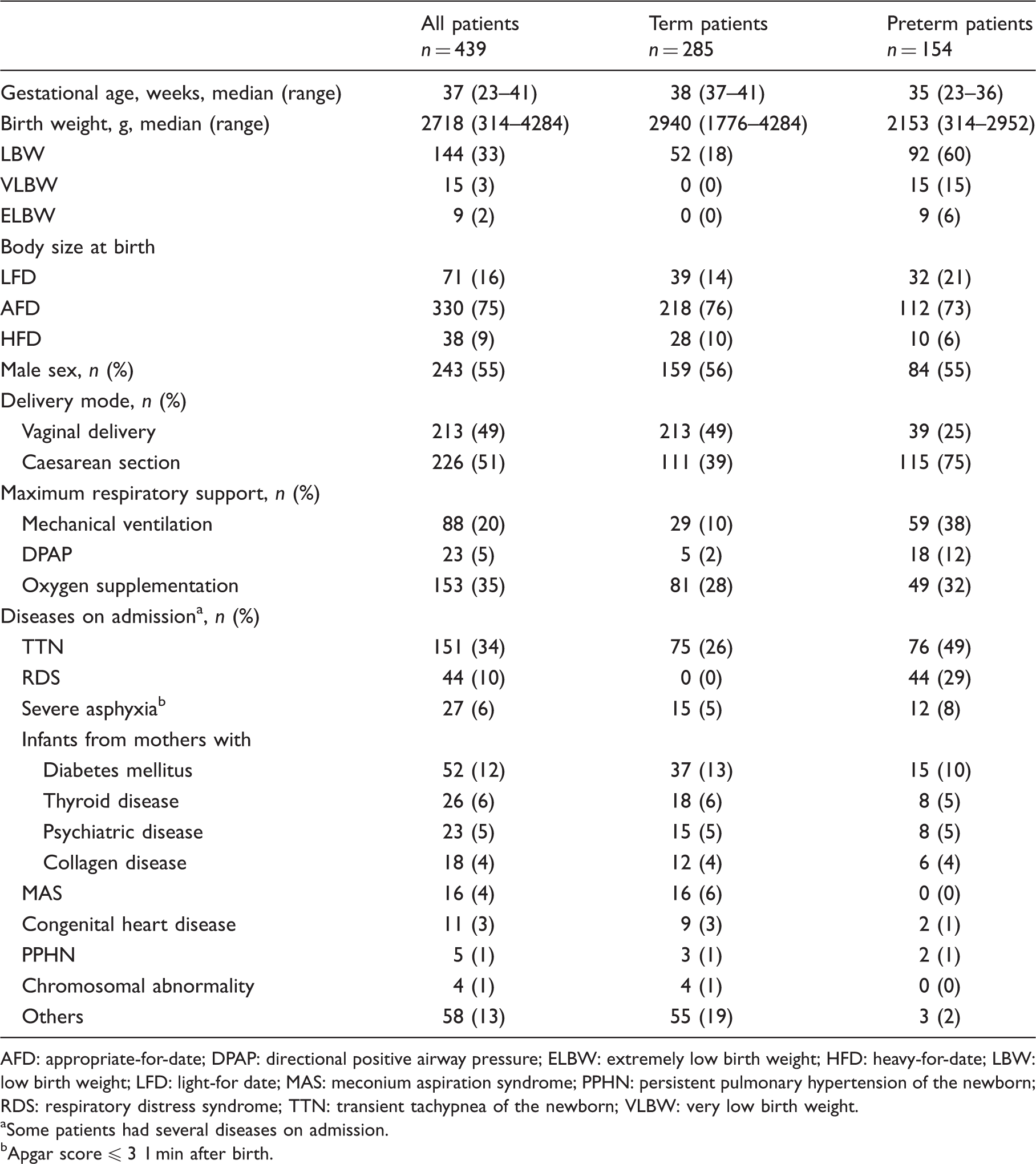
AFD: appropriate-for-date; DPAP: directional positive airway pressure; ELBW: extremely low birth weight; HFD: heavy-for-date; LBW: low birth weight; LFD: light-for date; MAS: meconium aspiration syndrome; PPHN: persistent pulmonary hypertension of the newborn; RDS: respiratory distress syndrome; TTN: transient tachypnea of the newborn; VLBW: very low birth weight.
Some patients had several diseases on admission.
Apgar score ≤ 3 1 min after birth.
Postnatal serum concentrations of FFA and Alb were reported as day-specific percentile-based curves. Newborn patients were divided into three subgroups by body size at birth: light-for-date (LFD, n = 71), appropriate-for-date (AFD, n = 330), and heavy-for-date (HFD, n = 38) and serum FFAs and FFA/Alb ratios were compared among them on each day after birth. LFD, AFD or HFD was defined as a birthweight less than 10th percentile, between 10th and 90th percentile, or more than 90th percentile for the same GA. 17 Furthermore, the time courses of serum FFAs and FFA/Alb ratios were also compared in term (birth at GA ≥ 37 weeks, n = 285) and preterm (birth at GA < 37 weeks, n = 154) patients on each day after birth.
To investigate the impact of FFA on UB, first, FFA/Alb ratio and UB/TB ratio during the first 5 days after birth were assessed in 310 serum samples from 235 term newborns without receiving phototherapy or any drugs. On each day after birth, the number of patients receiving infusions or feedings, including with types of milk, was recorded. Secondly, correlations between FFA/Alb ratio and serum UB concentration or UB/TB ratio were analyzed using 140 sera with hyperbilirubinemia in term and preterm patients without receiving phototherapy or any drugs (serum TB ≥ 120 mg/L for term sick patients, n = 79, and serum TB ≥ 80 mg/L for preterm patients, n = 61). 18
Samples
Blood samples were obtained from newborn patients at birth to 5 days of age at the discretion of the attending neonatologist, based on their clinical conditions, with multiple blood samples obtained from some patients on different days. Blood samples were obtained around 3 h after feeding from newborns who were tube-, bottle-, or breast-fed, and around 2 h after feeding from patients with birth weight <1500 g. Newborns received breast milk, formula, or both breast milk and formula (mixed feeding). Blood samples were promptly centrifuged and sera obtained.
Assay methods
Serum Alb concentrations were measured using the modified bromocresol purple method (Kainos laboratories, Inc., Tokyo, Japan), whereas serum FFA concentrations were assessed using an enzymatic acyl-CoA synthetase-acyl-CoA oxidase-peroxidase method (Eiken Inc., Tokyo, Japan), as described.19,20 Serum UB and TB concentrations were measured using a Food and Drug Administration-approved analyzer (UB Analyzer; Arrows Co., Ltd, Osaka, Japan), using spectrophotometry and the glucose oxidase-peroxidase method, respectively, as previously described.6,21–26 Serum UB concentrations were measured using a single peroxidase concentration method, as recommended by the manufacturer.6,21–26
Calculations and statistical analyses
The UB/TB ratio and FFA/Alb ratio were calculated using the following equations:


Results
The clinical characteristics of the 439 enrolled patients are shown in Table 1. Of these newborns, 51% were born by caesarean section and 60% received respiratory support. Most of the enrolled patients had common neonatal diseases, although two, both born at term, had congenital abnormalities of the gastrointestinal tracts and required surgery.
Figure 1 shows the postnatal day-specific percentile-based curve of serum FFA and Alb in these 439 newborns. Serum FFA concentrations peaked at 1 day of age and decreased thereafter, whereas serum Alb concentrations remained almost constant over the study period. On each day after birth, no significant differences in values of serum FFA and FFA/Alb ratio were found among newborns with LFD, AFD and HFD (Table 2). Figure 2 shows the time course of serum FFA and FFA/Alb ratio in term and preterm newborns from birth to 5 days of age. Serum FFA concentrations were significantly higher in term than in preterm patients at birth and at 1 and 3 days of age. In term patients, the serum concentrations of FFA and the FFA/Alb ratio were significantly lower at 5 days than at 1, 2 and 3 days of age, and were significantly lower at 4 days than at 1 day. In preterm infants, there were no significant differences in serum FFA and FFA/Alb ratio from 1 to 5 days of age.
Postnatal day-specific percentile-based curves showing the 5th, 50th and 95th percentile tracks of serum FFA (a) and Alb (b) concentrations from birth to 5 days of age in 713 serum samples from 439 newborns without intravenous lipid supplementation admitted to the NICU. Alb: albumin; FFA: free fatty acid; NICU: neonatal intensive care unit. Time course of serum FFA (a) and FFA/Alb ratio (b) in term and preterm newborns. Data are expressed as mean ± SD. In term infants, serum FFA and FFA/Alb ratio were significantly lower on day 5 than on days 1, 2 and 3, and were significantly lower on day 4 than on day 1. In preterm infants, there were no significant differences in serum FFA and FFA/Alb ratio on days one to five. Serum FFA levels were significantly higher in term than in preterm infants at birth and at 1 and 3 days of age. *p < 0.05, **p < 0.01 compared with preterm infants. Alb: albumin; FFA: free fatty acid. Serum FFA (A) and FFA/Alb ratio (B) in newborns with LFD, AFD and HFD.a AFD: appropriate-for-date; Alb: albumin; FFA: free fatty acid; HFD: heavy-for-date; LFD, light-for-date. Data are expressed as mean ± SD.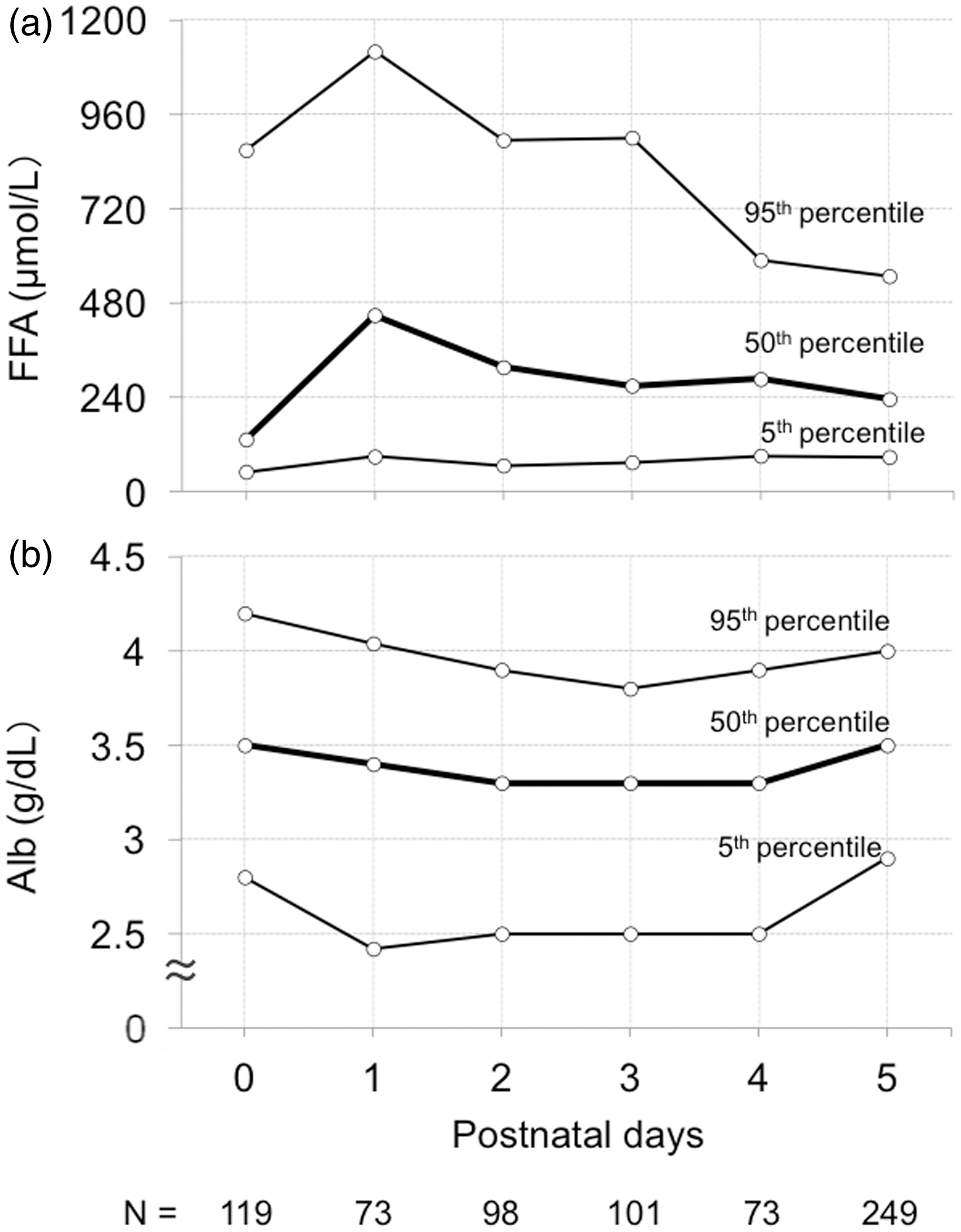
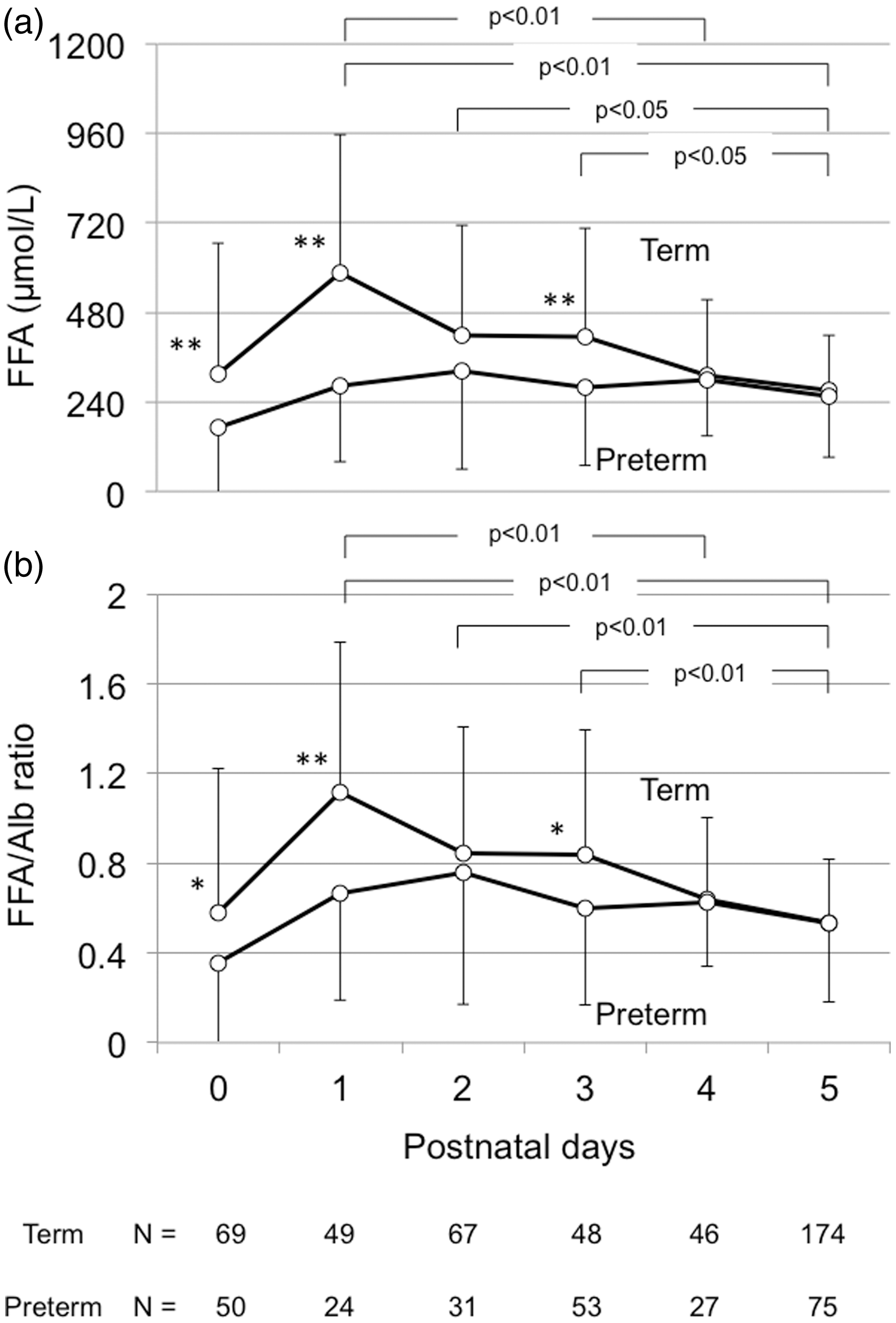
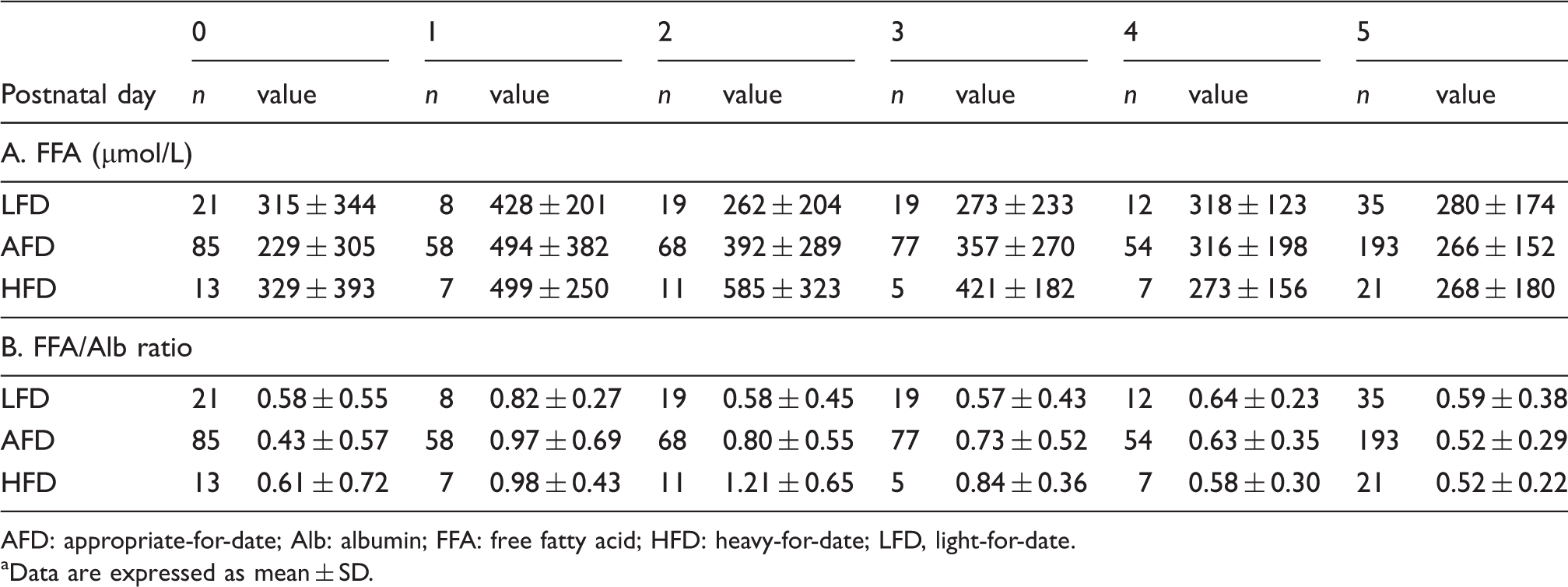
Figure 3 shows the FFA/Alb and UB/TB ratios from at birth to 5 days of age in the sera of term newborns without receiving phototherapy or drugs. All sera at 0 day of age were obtained before the introduction of feeding or any treatment. The numbers of serum samples obtained following infusions were significantly higher on days 1 and 2 than on days 3, 4 and 5, whereas the numbers of samples obtained following feeding were significantly lower on day 1 than on any other days. The FFA/Alb ratio changed significantly over the first 5 days after birth, whereas the UB/TB ratio remained relatively constant.
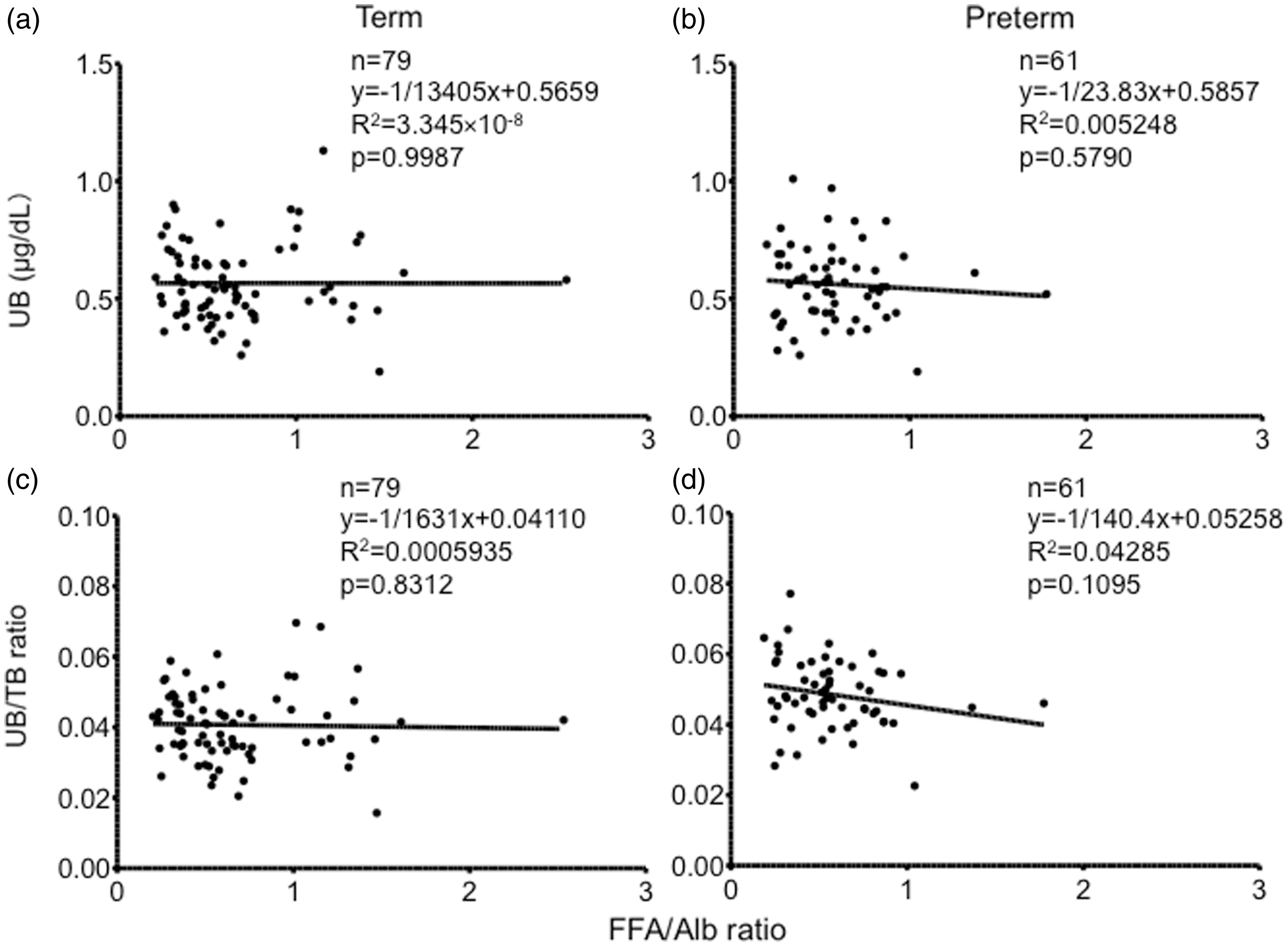
Sera with hyperbilirubinemia in term and preterm patients without receiving phototherapy or any drugs were analyzed. Serum TB concentrations in sera of term and preterm patients were 139 ± 13 (range: 120–178) and 115 ± 19 (range: 82–156) mg/L, respectively. Linear regression analysis showed that the FFA/Alb ratio did not correlate with the serum UB concentration or UB/TB ratio in the sera with hyperbilirubinemia (Figure 4).
Changes in FFA/Alb ratio and UB/TB ratio in term newborns not treated with phototherapy or any drugs (upper figure) and the numbers receiving infusions or feeding including a kind of milk (lower table). FFA/Alb ratio changed significantly over 5 days after birth, but UB/TB ratio remained constant. All sera on day 0 were obtained before the introduction of feeding or any treatment. Data are expressed as mean ± SD or number (%). *p < 0.05 compared with another age. Alb: albumin; FFA: free fatty acid; TB: total bilirubin; UB: unbound bilirubin. Correlation between FFA/Alb ratio and serum UB concentration or UB/TB ratio in sera with hyperbilirubinemia of term (a and c) and preterm patients not treated with phototherapy or any drugs (b and d). Sera with TB ≥ 120 mg/L for term patients and TB ≥ 80 mg/L for preterm patients were analyzed. Alb: albumin; FFA: free fatty acid; TB: total bilirubin; UB: unbound bilirubin.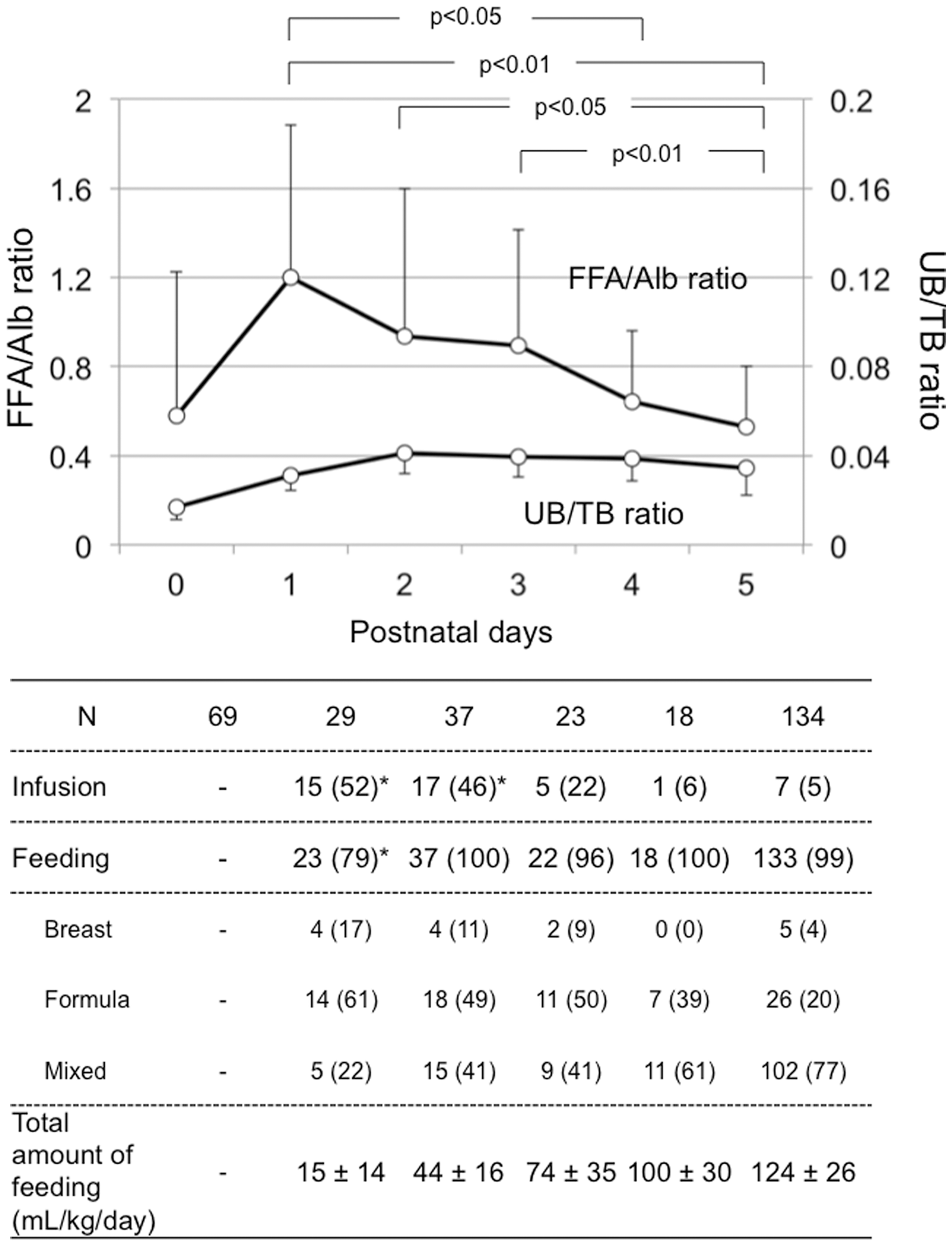
Discussion
We assessed serum FFA concentrations and FFA/Alb ratio during the first 5 days after birth in a large number of high-risk newborns admitted to the NICU. Importantly, we found all of these patients, regardless of age, had an FFA/Alb ratio < 4. A ratio ≥ 4 would result in the displacement of bilirubin from binding sites and leads to elevated serum UB,7,8,10,27,28 although bilirubin displacement effects depend on the number of carbon atoms in FFA. 12 We also clearly demonstrated that endogenous serum FFA concentrations did not affect serum UB, as shown by comparisons between FFA/Alb ratio and UB/TB ratio over time in term patients and linear regression analysis between FFA/Alb ratio and serum UB concentration or UB/TB ratio in the sera with hyperbilirubinemia of term and preterm patients. These results should be useful in guiding the management of hyperbilirubinemia in patients admitted to the NICU, in that the effects of endogenous FFA on the displacement of bilirubin can be ignored.
Although previous studies have reported the postnatal concentrations of endogenous serum FFA in newborns,7,8,29,30 little was known about serum FFA concentrations at 4–5 days of age, when serum TB peaks. We found that serum FFA and FFA/Alb ratio at 4 and 5 days of age were significantly lower at 1 day of age in term patients. This result was in agreement with a report by Anagnostakis et al. 30 Another previous study, however, reported that serum FFA progressively increased from birth, peaking at 3 days of age. 29 This discrepancy was likely due to the differences in patient populations, in that the previous study enrolled newborns with normal adaptation, while excluding those who had acidosis or hypoxia. 29 We speculate that mortality and morbidity rates, as well as medical approaches and treatments, also differed in the two studies.
Our results showed that serum FFA peaked at 1 day of age because the factor influencing the serum FFA level is fatty acids release from adipose tissue in the delivery rather than uptake of fatty acids. 30 On the other hand, serum Alb was constant during the first 5 days of age. A human homeostasis system may play an important role to maintain the Alb level, although the detailed reasons are unclear.
In this study, serum FFA levels in newborns with LFD were not significantly higher than that in newborns with AFD and HFD. In contrast with our results, Anagnostakis et al. reported that LFD newborns during the first 2 days of life showed a significantly higher plasma FFA levels than the other newborn groups although the reasons were obscure. 30 We also found that serum FFAs and FFA/Alb ratio were lower in preterm than in term patients during the first 5 days after birth. Preterm infants may have less nutrition and immature lipolysis; an increased production of metabolic hormones, such as insulin, which can decrease FFAs; and/or limited amounts of fat.31,32
Although the impact of endogenous FFA has not been assessed directly, increased FFA has bilirubin displacing effects, especially in premature newborns receiving intravenous lipid supplementation for nutrition and growth.7,9,10,28,33 At an FFA/Alb ratio ≥4, FFAs compete with bilirubin at the bilirubin binding site, resulting in the displacement of bilirubin.7,8,10,27,28 We found that endogenous FFAs did not affect Alb binding of bilirubin, resulting in elevations of UB, since none of the sera, from both term and preterm infants, had FFA/Alb ratios ≥4. FFA/Alb ratios were <2 at 4–5 days of age, suggesting that FFA had little effect on Alb binding of bilirubin in the presence of high serum TB. Furthermore, FFA/Alb ratio was not correlated with serum UB concentration and UB/TB ratio in sera with hyperbilirubinemia of term and preterm patients.
It has been reported that increases in serum FFA and FFA/Alb ratio result in a decrease in bilirubin–albumin binding affinity in infants of GA ≤ 28, but not >28, weeks. 10 Furthermore, FFA was reported to affect the displacement of UB in premature infants of GA < 28 weeks only when they were receiving ≥1.5 g/kg/day intravenous lipid supplementation. 9 Because the median GA in our enrolled preterm infants was 35 weeks and their serum FFA and FFA/Alb ratio were lower, GA likely had little effect on bilirubin–albumin binding affinity and endogenous FFAs should not affect the Alb binding of bilirubin in this study.
Clinical factors, such as surgical operation, sepsis and steroid treatment, would likely contribute to elevated serum FFA. Surgery may increase fasting and stress in newborns. Two of our patients underwent surgery, but preliminary data showed that the FFA/Alb ratio did not increase to over 3 after surgery (data not shown). This result agrees with those in a previous report. 16 In contrast, none of the patients in this study had sepsis or were treated with steroids.
We measured serum UB concentrations using a single peroxidase concentration method, as described in many studies of Japanese infants.6,21–23,25,26 It has been suggested that UB concentrations measured by a single peroxidase concentration method do not equal equilibrium UB concentrations, which are confirmed by measuring UB concentrations at two different peroxidase concentrations. 24 However, close correlations have been observed between UB concentrations measured by single and two peroxidase concentration methods.22,24
As a limitation of this study, the postnatal day-specific percentile-based curve of serum FFA and the time course of serum FFA and FFA/Alb ratio in term and preterm newborns were established using cross-sectional data. However, longitudinal data may be more accurate.
In conclusion, this study showed serum FFA concentrations during the first 5 days after birth in a large number of high-risk newborns admitted to the NICU. Changes in serum FFAs and FFA/Alb ratio were different in preterm and term patients. The concentration of endogenous FFAs in newborns admitted to the NICU was not rising until it influenced UB.
Footnotes
Declaration of conflicting interest
None of the authors have any conflicts of interest to declare.
Funding
This work was supported by grants for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology in Japan (IM).
Ethical approval
The collections and uses of human materials for this study were approved by the Ethical Committee of Kobe University Graduate School of Medicine (Number: 844).
Guarantor
IM.
Contributionship
All authors contributed to the intellectual content of this manuscript. TK, IM, TY, DK, KF, MN, KM, and AS were neonatologists who cared the patients and collected the clinical samples and data. IS and SK measured serum concentrations of FFA, Alb, TB and UB. TK, IM, HY, HN and KI performed analysis of clinical findings. TK, IM, HN and KI designed this study. TK and IM wrote the first draft of this manuscript.