
Abstract
Background
Glomerular filtration rate (GFR) and mortality is more accurately determined by gold standard measures than serum creatinine-based estimates in cirrhosis. No formal validation of any gold standard method has been reported.
Methods
An isocratic methanol-based method incorporating the reference standard iohexol-related compound C was developed and validated in 12 patients with cirrhosis by simultaneously determining GFR using iohexol and chromium-51 labelled ethylenediamine tetraacetic acid (51Cr-EDTA) clearance. Iohexol pharmacokinetics was also studied with the collection of blood and ascitic fluid at intervals following an iohexol bolus.
Results
Triplicate assays produced a linear calibration curve (R2 = 0.99, N = 5) over an iohexol concentration range of 23.6–755 µg/L. Mean (range) extraction recovery of iohexol from serum was greater than 95% (94–97%), with an intra-day coefficient of variation less than 3%. Twelve patients with cirrhosis with mean Child-Pugh score of 9 displayed a mean difference (bias) −1.3 mL/min/1.73 m2 (−18 to + 16) comparing iohexol with 51Cr-EDTA. Iohexol equilibrated between blood and ascitic compartments after 4 h.
Conclusion
A simple, cheap, and accurate isocratic, methanol-based method for the determination of iohexol concentrations is described, validated according to Food and Drug Administration guidance. Iohexol demonstrated comparable performance with 51Cr-EDTA in determining GFR. Delayed equilibrium of iohexol between blood and ascitic compartments suggests sampling beyond 4 h would improve accuracy of GFR determinations in patients with cirrhosis.
Introduction
Kidney function is an important determinant of mortality in patients with cirrhosis both before and after liver transplantation.1,2 Serum creatinine concentration has routinely provided the best performing endogenous marker of glomerular filtration rate (GFR). However, neither the measurement of serum creatinine concentration nor the estimation of GFR is accurate in patients with cirrhosis.1,2 Several formulae have been derived to improve the accuracy of estimated GFR (eGFR) by incorporating non-serum creatinine factors, including cystatin C-based methods, but continued deficiencies remain.1–3 Nonetheless, serum creatinine concentration has been incorporated into models predicting mortality, prognosis and outcome such as model for end-stage liver disease score (MELD). 4 The numerous methods available for the determination of serum creatinine concentration have been shown to affect MELD scores 3 and the substitution of true GFR for serum creatinine in the MELD score displays superior performance in predicting mortality. 2
True GFR measurement involves the analysis of the rate of clearance of an exogenous marker, like chromium-51 labelled ethylenediamine tetraacetic acid (51Cr-EDTA) or the iodinated contrast medium, iohexol. Both have been widely studied with reportedly good correlation in patients with GFR >40 mL/min/1.73 m2. 5 No specific validation in patients with cirrhosis has been reported. Iohexol, a non-ionic contrast media, has been used for the determination of GFR for many years and is now recognized as an established gold standard measure.5–8 Iohexol has two major advantages over 51Cr-EDTA: firstly, it is not a radioactive isotope associated with strict regulations regarding distribution, handling and administration to patients; secondly, 51Cr-EDTA complex is not available for clearance studies in the United States.
Iohexol concentrations in serum or plasma have been measured largely by high-performance liquid chromatography coupled to ultra-violet light absorption (HPLC-UV) techniques. These methods rely largely on the use of the solvent acetonitrile. Only one documented method in the literature incorporates an internal standard and that employs a gradient method with methanol (MeOH). 9 In 2009, the global economic downturn led to significant reduction in manufacturing output and a shortage of acetonitrile, a by-product of car manufacturing, so dramatically increasing its cost.
The aims of this study were: firstly, to develop a cheap and simple isocratic method for determining iohexol concentrations in serum using UV-HPLC techniques incorporating an internal standard to accommodate unrecognized sample-processing errors; secondly, to validate the method according to formal guidance in patients with cirrhosis; thirdly, to undertake a direct comparison clinical study of iohexol clearance versus a reference gold standard method, 51Cr-EDTA. Finally, to study the pharmacokinetics of iohexol in patients with large volume ascites. Interval analysis of iohexol concentrations, in both serum and ascites, after an initial bolus was undertaken to understand the distribution of iohexol in such patients.
Materials and methods
Patients and study design
Twelve patients (nine men) with cirrhosis and a serum creatinine <110 µmol/L were studied. All showed at least one of the following: a significant coagulopathy (international normalized ratio (INR) >1.5), serum bilirubin rising >150 µmol/L and diuretic resistant ascites.
Patient demographics.
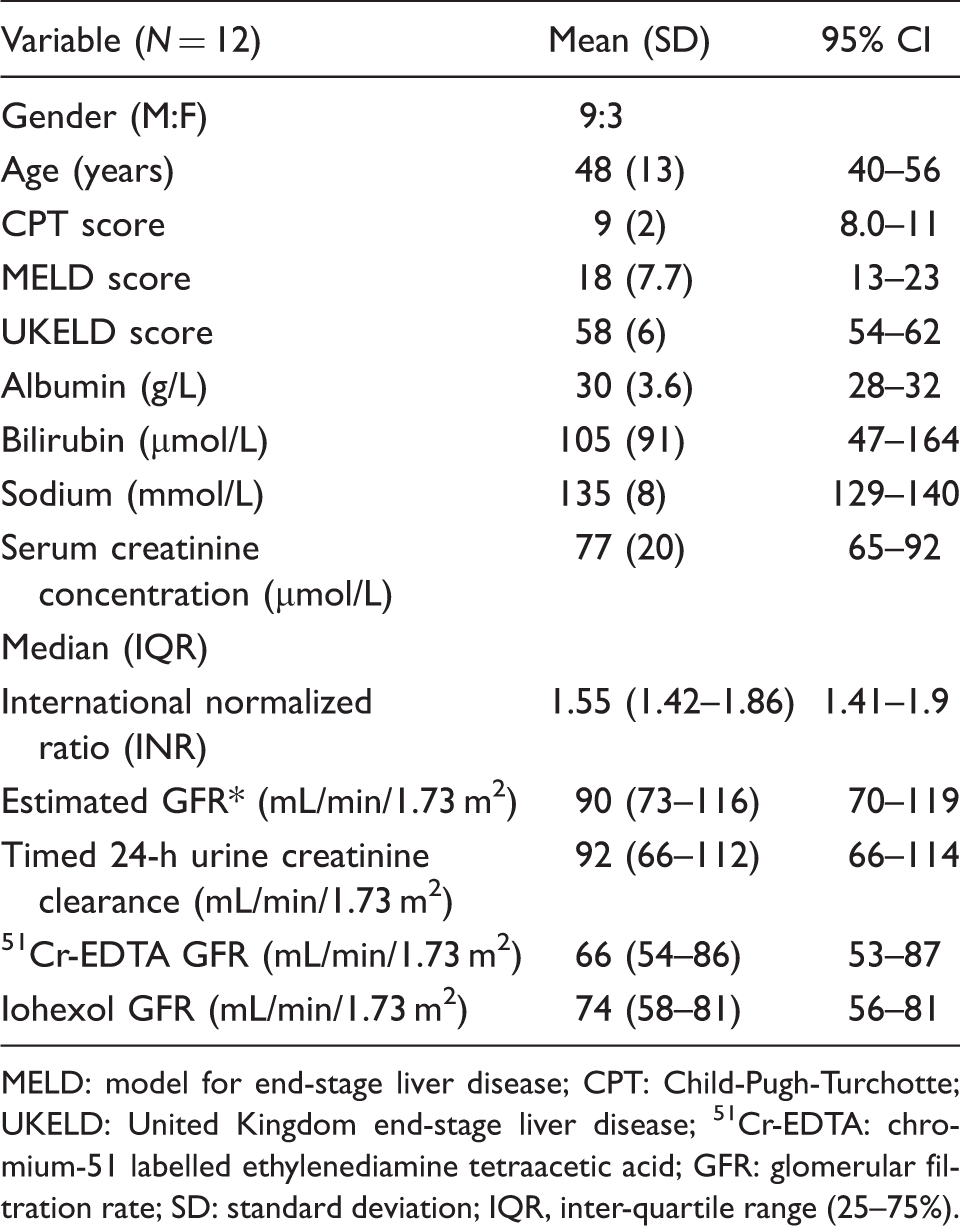
MELD: model for end-stage liver disease; CPT: Child-Pugh-Turchotte; UKELD: United Kingdom end-stage liver disease; 51Cr-EDTA: chromium-51 labelled ethylenediamine tetraacetic acid; GFR: glomerular filtration rate; SD: standard deviation; IQR, inter-quartile range (25–75%).
We developed and validated an HPLC-UV isocratic methanol-based method for determining serum iohexol concentration in patients with cirrhosis between January 2010 and January 2012. The validation process followed the United States Department of Health and Human Services Food and Drug Administration (FDA) and European Medicines Agency (EMA) guidance12,13 for the isocratic HPLC-UV method using methanol in the mobile phase with incorporation of the United States Pharmacopeia (USP) reference standard iohexol-related compound C, as a reference internal standard. A direct comparison of iohexol and 51Cr-EDTA clearance in the 12 patients with cirrhosis was performed. Three patients underwent an interval analysis of the distribution of iohexol concentrations over time in serum and ascites. Serum and ascites were collected in 10 mL aliquots at 15–25 min intervals following a bolus of 5 mL of iohexol (755 mg/mL). The collection of ascites required the percutaneous insertion of a BD Bonnano™ suprapubic catheter into the peritoneum under aseptic conditions. Paracentesis was clinically indicated, but drainage of ascites was delayed for 2 to 4 h until the study period was over. All patients had indwelling intra-arterial catheters for the collection of blood.
Ethics approval
The Coventry Research and Ethics committee, authorized the research in accordance with Mental Capacity Act 2005 (given the possibility of hepatic encephalopathy). The Research and Development Department in the hospital and Administration of Radioactive Substances Advisory Committee, 1998 (ARSAC) also approved the study, 09/H1210/72. All patients were able to give their written informed consent to participate.
Baseline variables collected were age, gender, serum creatinine concentration, bilirubin, albumin, sodium and estimated GFR (using the four-variable MDRD equation) and a timed urine creatinine clearance. Liver-specific variables included aetiology of chronic liver disease, MELD, 4 UKELD 11 and Child-Pugh (CP) Scores. 14 Ascites grade was determined using the international ascites club classification. 15
Iohexol and 51Cr-EDTA studies
Simultaneous iohexol and 51Cr-EDTA clearance studies were performed in the nuclear medicine department. A butterfly needle was inserted into a vein in either arm, and baseline, blood, serum (iohexol) and plasma (51Cr-EDTA) samples were drawn. A bolus injection of 5 mL Omnipaque (755 mg/mL of iohexol corresponding to 350 mg iodine/mL) (GE Healthcare, Buckinghamshire, UK) was administered followed by 10 mL saline flush. Immediately afterwards, 4 mL 51Cr-EDTA tracer in a prefilled syringe was administered followed by 10 mL saline flush. Interval blood sampling was undertaken at approximately 2, 3 and 4 h, from a vein on the contra-lateral arm. Blood (10 mL) was collected into one BD Vacutainer® SSTTM II Advance and one Heparin Tube (BD Vacutainer, Plymouth, UK). Blood samples were centrifuged for 10 min at 1500 g and room temperature. Separated serum was stored at −80℃ until analysis and 1 mL plasma was transferred into pre-labelled counting tubes. Duplicate samples and standards were counted in a Packard Cobra II 5003 Gamma Counter. Background counts were subtracted and mean values calculated. The GFR was determined using the area under the activity versus time curve for both methods with the application of Brochner Mortensen’s quadratic equation. 16
HPLC reagents and method
Iohexol: (N,N′-Bis(2,3-dihydroxypropyl)-5-[N-(2,3-dihydroxypropyl)-acetamido]-2,4,6-triiodoisophthalamide) (molecular weight 821.14, iodine span 46.36%) was obtained from GE Healthcare (Buckinghamshire, UK) as Omnipaque 350. In aqueous solution, each triiodinated molecule remains undissociated and contains 755 mg/mL of iohexol, equivalent to 350 mg/mL of organic iodine. Each millilitre of iohexol solution (pH adjusted to 6.8–7.7) also contains 1.21 mg tromethamine and 0.1 mg edetate calcium disodium.
Iohexol-related compound C: (N,N′-bis(2,3-dihydroxypropyl)-5-nitro-1,3-benzenedicarboxamide) was purchased from the USP convention.
Other chemicals: Trifluoracetic acid (TFA) Chromasolv® for HPLC >99.0% and HPLC grade methanol (MeOH) were obtained from Sigma–Aldrich Company Ltd (Gillingham, Dorset, UK). Perchloric acid (PCA, analytical grade) was purchased from BDH Laboratory Supplies, Poole, Dorset, UK. A water purification system (Milli Q system, Millipore U.K. Limited, Watford, UK) provided deionized water.
Chromatography was performed using a 5-µM Supelco Discovery C18 analytical column (250 mm × 4.6 mm internal diameter (i.d.); Sigma-Aldrich Company Ltd, Gillingham, UK). An in-line 40–50 µm particulate C18 guard column (30 mm × 4.6 mm i.d.) preceded the analytic column. Analysis was performed using two Waters™ pumps, 501 and 510 (Water, Elstree, UK) with a Waters™ 717 Autosampler (Water, Elstree, UK) and a Waters™ 996 photodiode array detector. Millennium32 Version 4.00 software, (Waters, Elstree, UK), was used to run the isocratic method and process chromatographic data.
Calibrators and quality control standards preparation
Serial dilution of iohexol was made in deionized water to achieve six standard concentrations of 3775, 1887.5, 943.7, 471.8, 235.9 and 117.95 µg/mL. These standards were then processed in an identical manner to patient serum and ascitic samples with a one in five dilution with the precipitation solution. The final working concentrations of the standards following processing with 5% PCA containing iohexol-related compound C (IRC) included 755 µg, 377.5, 188.75, 94.375, 47.18 and 23.59 µg/mL. Internal quality control (IQC) samples were prepared by performing serial dilutions of aqueous standards in blank serum and patient ascites to produce high, medium and low concentration IQCs containing 252, 126 and 63 µg/mL, respectively. All working standards and controls were stored at −80℃, Processed patient samples, calibrators and quality control standards were injected in triplicate.
The working internal standard/precipitation solution was prepared from IRC (5 mg) in 5% PCA (10 mL) followed by a further 1:25 dilution with 5% PCA to 20 µg IRC per mL. A standard curve was produced, from the determination of the six standard concentrations in triplicate. The low-, medium- and high-quality control (QC) samples were repeatedly assayed five times to determine the accuracy and precision of the method with the coefficient of variation (CV) calculated. Recovery was determined by analysing the three high-, medium- and low-concentration QCs prepared in serum.
Chromatography
The mobile phases were 95% MeOH/5% deionized H2O/0.1% aq TFA at pH 2.2 (organic) and 95% H2O/5% MeOH/ 0.1% TFA pH 2.2 (aqueous). These were mixed isocratically using 15% organic and 85% aqueous at a flow rate of 1 mL/min.
The serum samples collected from patients, serum calibrators or IQC samples (100 µL) were vortexed with PCA containing internal standard (400 µL) in 1.5 mL microcentrifuge tubes for 30 s and centrifuged for 10 min in an Eppendorf micro-centrifuge at 3000 rpm for 10 min. Supernatant (150 µL) was transferred into 5.0 mm clear micro-inserts within amber vials on the auto-sampler carousel and 20 µL injected after establishing stable chromatographic conditions.
Chromatography profiles are shown for an iohexol-free sample (pre-dose) and a corresponding sample spiked with iohexol (Figure 1a and b, respectively). Total run time of 12 min was required with an internal standard (IRC) that eluted at 9.63 min and the geometric exo and endo-isomers
17
of iohexol eluting at 4.49 and 4.72 min, respectively. All patients who underwent an iohexol clearance had pre-iohexol bolus serum sample analysed to determine if any interfering peak were evident at the retention times for both the endo-isomer of iohexol and the IRC. The photodiode-array detector was used to produce 3D data to analyse the endo-isomer peak, which had a maximum absorbance of 245.6 nm. These data were utilized to interrogate chromatograms to ensure no co-eluting peaks were present. No major interfering peaks at the time of elution of iohexol or IRC were identified for any of the patients with chronic liver disease in this study.
Chromatograms for iohexol isomers and internal standard, iohexol-related compound C. Iohexol chromatograms showing Iohexol-related compound C eluting at 9.6 min (a) and iohexol isomers at 4.5 and 4.7 min (b).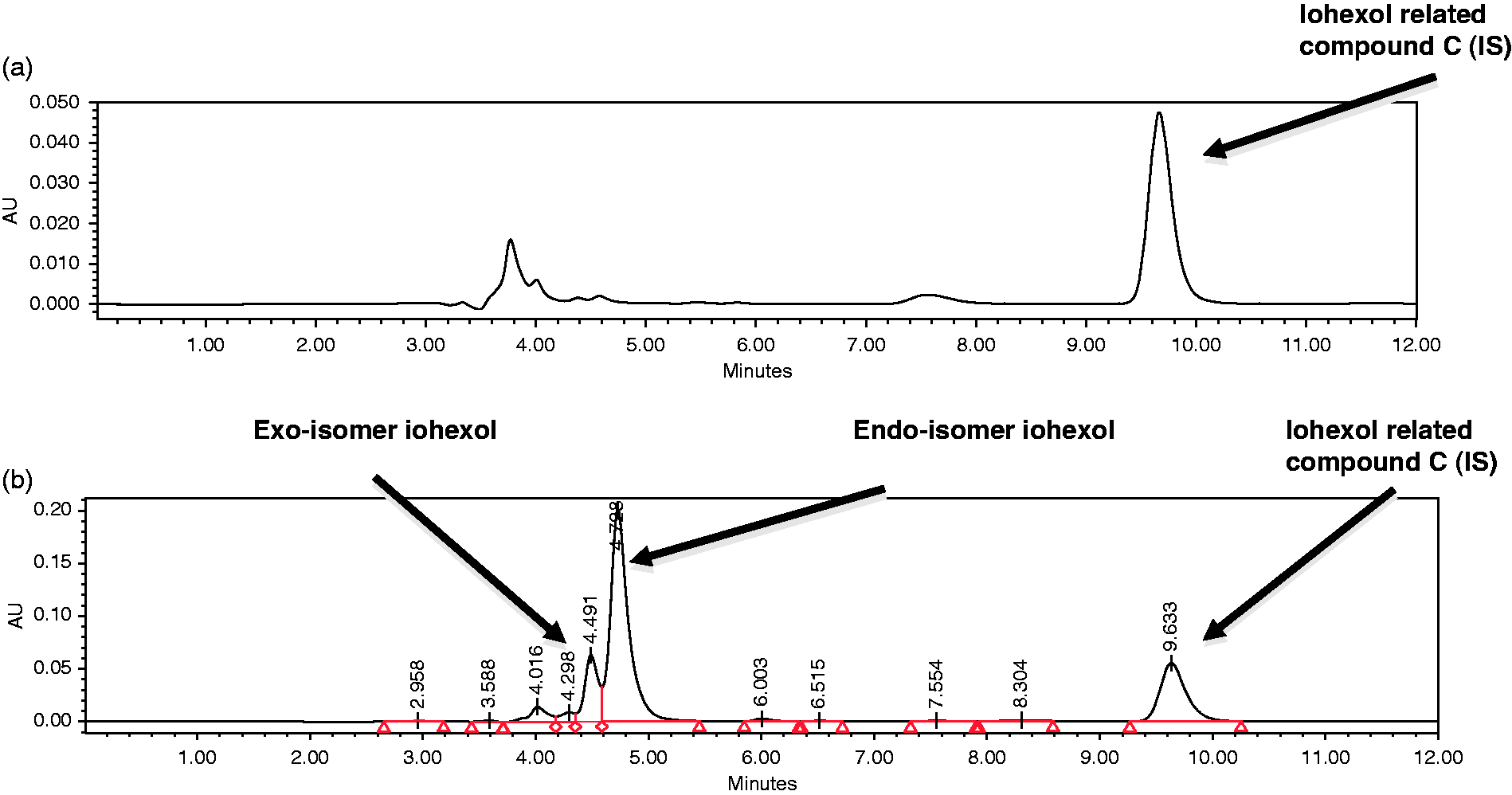
The ratio of the, single isolated, larger exo-isomer peak area of iohexol, retention time 4.7 min and IRC peak area, retention time 9.6 min was used to calculate an iohexol:IRC ratio for quantification. The method was validated using guidelines issued by the US FDA and EMA.10,18 Serum samples collected prior to iohexol bolus administration were analysed with any detectable chromatographic peaks, reflecting baseline noise at the retention time for exo-isomer of iohexol, quantified. The lower limit of detection (LOD) was determined by the standard deviation of these chromatographic peaks multiplied by 3.29. 18 The lower limit of quantification (LOQ) was the lowest concentration identified from the best-fit curve of CV % versus iohexol concentration at a limit of 20%.
Analyte stability was assessed over 16 h by analysing calibrators and QCs repeatedly on three separate occasions, at 6-h intervals, during a continuous analytical run. The three concentrations of QCs, stored at −80℃ for over one week, were thawed at room temperature and then analysed. Matrix effects were evaluated by analysing the accuracy, precision and recovery of high-, medium- and low-concentration QCs produced by spiking patient ascitic fluid with iohexol as described.
Statistical analysis
Data were assessed for normality using the D’Agostino Pearson test. Measures of central tendency were compared using the Student t test (ANOVA) or Mann–Whitney U test (Kruskall Wallis) test for independent normally or non-normally distributed data. Repeated measures ANOVA or the Friedman test was used for serially measured data. Categorical data were compared using the chi-squared test. Bland-Altman plots evaluated the agreement between methods used for determining GFR.
Results
GFR estimates
Mean estimated GFR using MDRD calculations from serum creatinine was median (range) 90 (51–129) mL/min/1.73 m2. The 10 patients who completed a timed 24-h urinary creatinine clearance showed mean 92 (32–120) mL/min/1.73 m2. One patient was incontinent of urine due to learning difficulties and one collection was lost. 51Cr-EDTA and iohexol clearance displayed a median of 66 (45–103) mL/min/1.73 m2 and 74 (48–100) mL/min/1.73 m2, respectively (Table 1). A significant difference was demonstrated between all four measures of GFR, in the 10 patients with complete data available (Figure 2). Results using a four-variable MDRD equation for eGFR, timed 24-h urinary creatinine, 51Cr-EDTA and iohexol clearance were 81 (51–129), 92 (32–120), 60 (45–103) and 66 (48–100) mL/min/1.73 m2, respectively (P = 0.006, ANOVA, Friedman test).
Box and Whisker plots for four measures of GFR in 10 patients with cirrhosis. MDRD 4: modified diet in renal disease four-variable equation; Creatinine clearance: timed urine creatinine clearance over 24 h; Iohexol: Iohexol clearance; Cr51_EDTA: chromium-51 labelled ethylenediamine tetraacetic acid.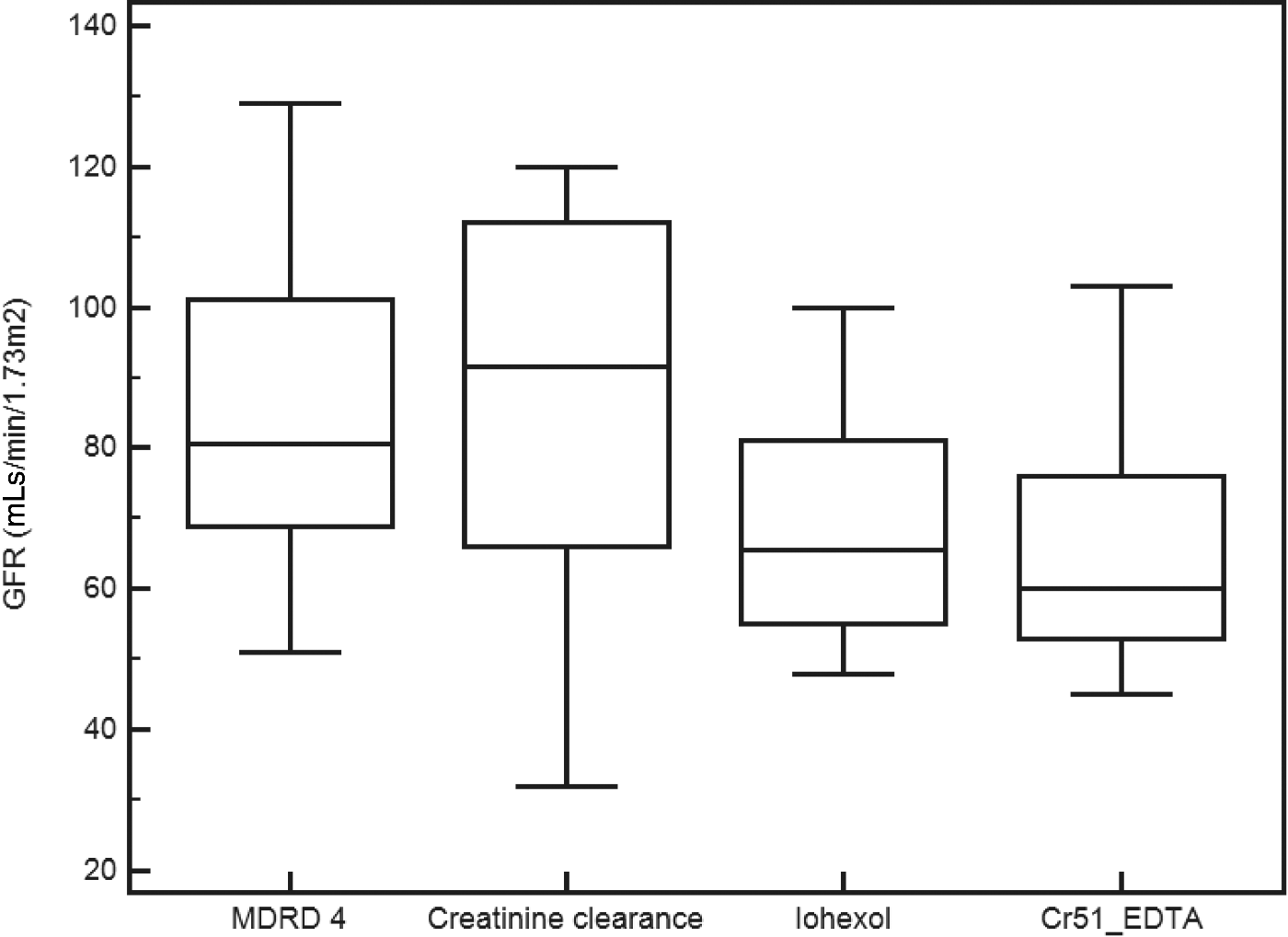
Bland-Altman analysis of the three methods was performed against the gold-standard 51Cr-EDTA. This demonstrated that eGFR determined using the four-variable MDRD equation and timed urinary creatinine clearance were the least accurate and precise: −22 (−46 to +1.4) and −22 (−73 to +29) mL/min/1.73 m2, respectively. Iohexol results were comparable to 51Cr-EDTA with a mean difference (bias) of −1.3 (−18 to +16) mL/min/1.73 m2 (Figure 3).
Bland-Altman plot comparing 51Cr-EDTA with iohexol clearance for determining glomerular filtration rate in 12 patients with cirrhosis.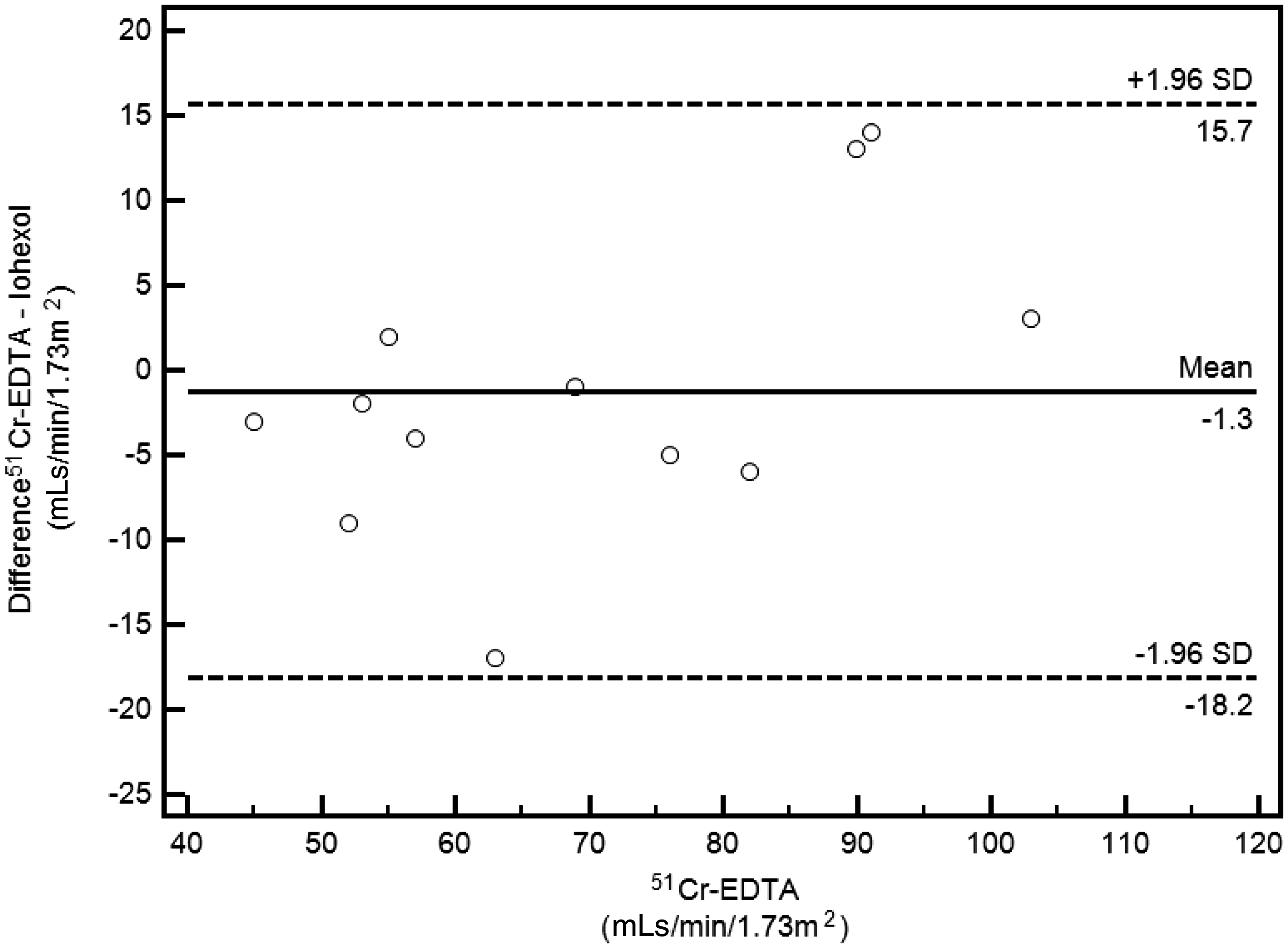
HPLC
Performance of the Iohexol liquid chromatography assay.
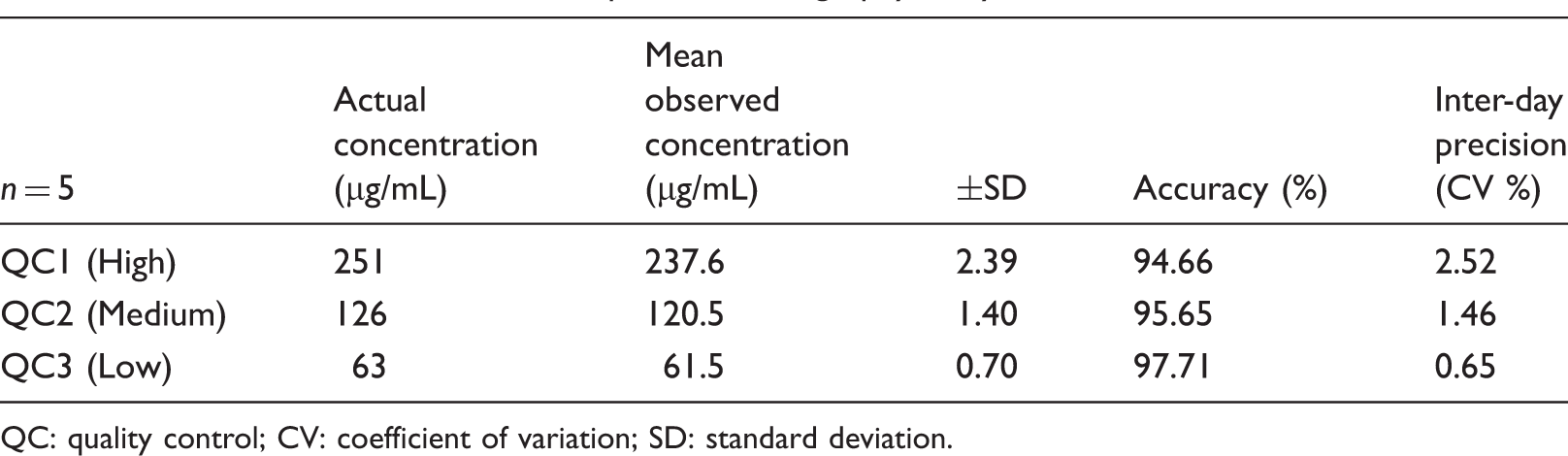
QC: quality control; CV: coefficient of variation; SD: standard deviation.
Ascitic fluid spiked with iohexol to produce high-, medium- and low-QCs concentrations at 252, 126 and 63 µg/mL displayed an accuracy of 106 (100–109), 101 (93–105) and 102 (100–104)%, respectively, n = 5. The calculated precision (CV) at each concentration was 4, 5 and 1%. The recovery (SD) for the ascitic QCs high, medium and low were 106 ± 4, 101 ± 5 and 102 ± 1%, respectively.
Iohexol clearance and ascites
Dynamic iohexol concentration curves demonstrated that iohexol entered the ascitic compartment and accumulated over time reaching equilibration within blood by 5 h in patient 1 (Figure 4a). Equilibration between the vascular and ascitic compartments was not achieved completely before 4 h following the bolus of iohexol in patients 2 and 3 (Figure 4b and c).
Dynamic evaluation of the distribution of iohexol in three patients with cirrhosis and large volume ascites. (a) Patient 1 – MDRD, 65 mL/min/1.73 m2; Iohexol GFR, 36 mL/min/1.73 m2. (b) Patient 2 – MDRD, 76 mL/min/1.73 m2; Iohexol GFR, 35 mL/min/1.73 m2. (c) Patient 3 – MDRD, 105 mL/min/1.73 m2; Iohexol GFR, 60 mL/min/1.73 m2. MDRD: modified diet in renal disease four-variable equation.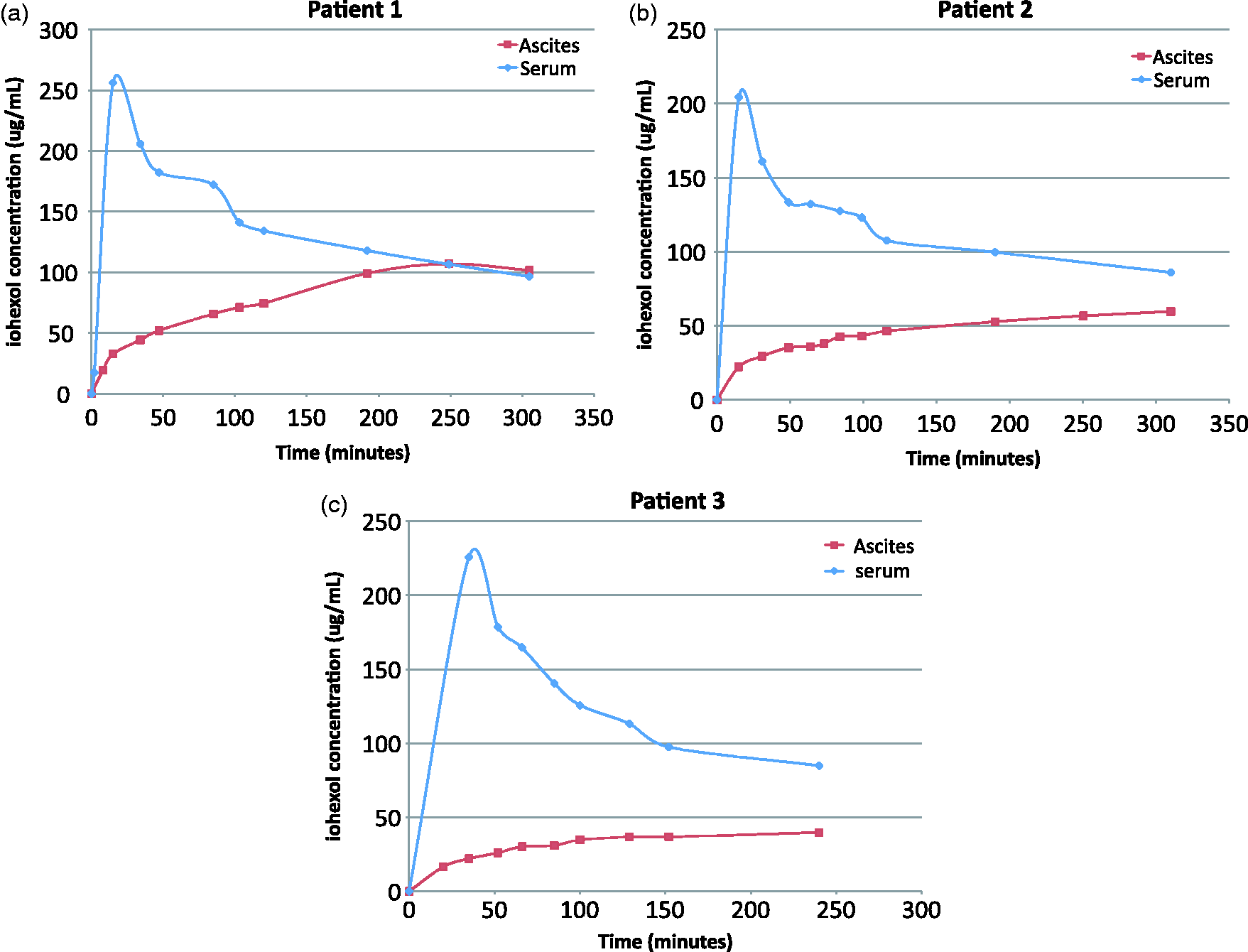
Discussion
We describe the first validated true measure of glomerular filtration in patients with cirrhosis using direct estimation with iohexol and demonstrate comparable results with a 51Cr-EDTA technique. These two methods have been shown to be comparable in patients with renal disease and an estimated GFR >40 mL/min/1.73 m2, but not previously in a cohort of patients with liver disease. 5 This method, in keeping with other gold standard measures, displayed superior accuracy and precision to estimated GFR and timed urine creatinine clearance confirming their well-described inaccuracies in patients with cirrhosis. 1
Iohexol was measured using a novel isocratic, methanol-based method improved by inclusion of a reference internal standard and validated against FDA and EMA guidelines.10,18 The potential for application of this method in a wider clinical setting relates to its lower material costs and robustness. Direct comparison of iohexol clearance with 51Cr-EDTA indicates good accuracy and precision suggesting application in outpatient and ward based environments is possible, unlike radio-isotopic methods.
When GFR rather than serum creatinine is used for calculating MELD scores, a closer prediction of mortality is possible. 10 An accurate assessment of GFR may allow better evaluation of the suitability for both liver and combined liver-kidney transplantation given creatinine concentration reflects true GFR so poorly. The case for making iohexol-based calculations of true GFR in all such transplant recipients seems convincing.
Abdominal ascites acts as a third space fluid compartment into which exogenous markers like iohexol diffuse and can be associated with a 20% overestimation in true GFR. 2 Iohexol has been shown to distribute into the ascitic compartment following contrast computer tomography scanning persisting for up to three days. 19 The pharmacokinetic measurements described here demonstrate that iohexol reaches equilibrium between blood and ascitic fluid compartments after 4 h in these patients with an estimated GFR greater than 60 mL/min/1.73 m2. In patients without cirrhosis sampling intervals have been suggested to be 3–4 h or 3 and 4 h in one and two sample methods in patients with an estimated GFR >40 mL/min/1.73 m2. 20 Sampling intervals of iohexol clearance studies in patients with cirrhosis and ascites should perhaps be prolonged based on this evidence.
Several limitations to this study are recognized. The study was undertaken in a single centre with only a small number of patients in both aspects of the study. We did not measure the iohexol concentration in urine, thus a timed urine clearance for iohexol could not be determined. This has been advocated as a more accurate method of determining GFR in patients with large third space fluid volumes. 21
In summary, this is the first report of a validated clearance method for determining true GFR in patients with cirrhosis. Such serum/plasma-based studies in cirrhotic patients with ascites require a delayed sample given the inaccuracies of estimated GFR and the time elapsed for iohexol to equilibrate within the ascitic compartment. A measure of true GFR should be performed in all potential liver transplant recipients. This cheap and simple iohexol method could facilitate such practice.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
None.
Funding
Funding received from King’s Liver charitable fund.
Ethical approval
Coventry Research and Ethics committee and Administration of Radioactive Substances Advisory Committee, 1998 (ARSAC) approved the study, Reference: 09/H1210/72.
Guarantor
AS.
Contributorship
KM, NB and MT assisted with HPLC development and validation. BC assisted with the ARSAC application and undertaking of the direct comparison study of iohexol with 51Cr-EDTA in the nuclear medicine department. All the authors contributed to the manuscript.