
Abstract
Background
Enzymatic assays, which can be run on a general automated clinical analyser, have been developed for haemoglobin A1c (HbA1c) measurement. The performance of the BM Test HbA1c which is an enzymatic HbA1c assay was evaluated using the Bio Majesty (BM)6010/C, which has an on-board haemolysis system.
Methods
We evaluated whether the difference in sampling position from the centrifuged erythrocyte layer caused a difference in HbA1c values obtained by the BM6010/C and the Tosoh G7. The performance of the BM Test HbA1c was evaluated.
Results
The results of the paired t-test showed no significant difference between the values of HbA1c when the tip positions of the sample probe were at 1 mm, 3 mm or 5 mm and the values given by the Tosoh G7. The coefficient of variation (CV) of intra-assay and inter-assay precision were both approximately 1.0%. The correlation coefficient obtained from an analysis of 351 routine laboratory samples with the BM Test HbA1c and the Tosoh G7 was 0.994. The upper limit of linearity was verified up to 17.0 (NGSP%). No interference was observed from chemically modified derivatives of haemoglobin. The presence of haemoglobin variants produced no statistically significant differences in the results between the BM Test HbA1c and the Primus high-performance liquid chromatography (HPLC). Accuracy evaluation using an International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) HbA1C control was within 3.4% relative error (%) of the assigned value.
Conclusions
The above outcomes prove that the measurement system, the BM Test HbA1c analysed on the BM6010/C, which has an on-board haemolysis system, is effective in laboratory routine tests.
Keywords
Introduction
Haemoglobin A1c (HbA1c) is a molecule in which the N-terminus of the beta-chain of haemoglobin (Hb) is non-enzymatically combined with glucose. The lifespan of a red blood cell is 120 days and its half-life is 60 days, so the HbA1c level reflects the average value of blood glucose concentration over the previous one to two months and can be an index for glucose level control.1–3
An estimated 285 million adults (20–79 years of age) in the world have diabetes mellitus, 4 and that number could rise to 439 million by 2030. Recent research estimated that 33% of adults in the United States will be diagnosed with diabetes by 2050. 5
In Japan, the ‘National Health and Nutrition Survey 2007’ conducted by the Ministry of Health, Labor and Welfare estimated that 22 million people are strongly suspected to have diabetes or pre-diabetes, which is a substantial risk of developing diabetes mellitus in the future. The survey indicated that the number of people who are suspected to have diabetes mellitus increased 1.3 times compared with 10 years earlier and the number continues to grow. 6 Furthermore, the criteria for the diagnosis of diabetes mellitus were revised by the Japan Diabetes Society in July 2010, which now defines that if both the blood glucose level and the HbA1c value obtained from the same blood sample are characterized as diabetes type, the diagnosis of diabetes mellitus can be made based only on the single examination. 7 The revision allows early diagnosis of diabetes mellitus, as well as early intervention, if both blood glucose level and HbA1c are measured during a medical checkup. 8
In our hospital, the number of blood samples obtained for HbA1c measurement has increased since we introduced a health examination that focused on metabolic syndrome and opened a diabetes center. The Tosoh G7 (HLC-723G7, Tosoh Corporation, Tokyo, Japan) has been used for HbA1c measurement in our laboratory, but it has several limitations. First, this method requires a dedicated device. It also requires a long time for measurement, and the HbC and HbE traits interfere with the results, thus causing potential problems. 9 Recently, immunological assays that can be run on a general automated clinical analyser have been developed. However, these methods require manual pretreatment for haemolysis, and then the pretreated solution was measured as a specimen on an automated analyser.
In this study, we conducted evaluations of the enzymatic assay BM Test HbA1c (JEOL Ltd., Tokyo, Japan). The anchor of traceability of this method is the IFCC reference method 10 and we used the test on the Bio Majesty (BM)6010/C (JEOL Ltd., Tokyo, Japan) with an on-board haemolysis system. The tip position of sample probe was selected prior to measurement. Based on this condition, the basic assay performance of this system, interference of chemically modified Hb, labile HbA1c and Hb variants were evaluated.
Materials and methods
Samples
Blood samples of inpatients, outpatients and hospital staff members who have undergone medical checkups were used. NIPRO neo tubes (NIPRO Corporation, Osaka, Japan), which contain EDTA-2 K, were used for blood collection.
The ethics committee in our hospital approved the use of the blood samples for this study.
Devices and reagents
The BM6010/C clinical chemistry analyser was used as the measurement device, because it has an on-board haemolysis system. This on-board haemolysis system on the BM6010/C has the following mechanism: Firstly, the analyser aspirates the sample from the packed erythrocyte layer in the sample that was centrifuged, using the sample probe. Then the aspirated sample is dispensed into a reaction cuvette on the analyser, in which the solution for pre-measurement haemolysis is already dispensed and it is where the on-board haemolysis takes place. After this step, the haemolysed sample is dispensed into another cuvette for the measurements.
The BM Test HbA1c was used as the enzymatic assay reagent.
The Tosoh G7 is an ion-exchange high-performance liquid chromatography (HPLC) that separates HbA1c from other Hb fractions based on differences in ionic charge.
The Primus HPLC (Primus CLC 330, Primus Diagnostics, Kansas, MO) is a boronate affinity method that separates glycated haemoglobin from the non-glycated haemoglobin based on the cis-diol group formed as a result of Hb glycation. The ratio of total glycated Hb, which includes HbA1c and Hb glycated at sites other than the terminus of the beta chain, to total Hb is calculated, and the results are standardized to Diabetes Control and Complications Trial HbA1c equivalents. Because boronate affinity methods measure the ratio of glycated to total haemoglobin regardless of the Hb species present, it is generally assumed that Hb variants do not interfere with HbA1c results. 11
Measurement procedure
We followed the measurement procedures stated in the manufacturers’ instructions for use for all the devices. Firstly, EDTA-containing blood samples were centrifuged at 800 g for 5 min to obtain a packed erythrocyte layer, Then 1.5 µL of the erythrocyte sampled from the packed erythrocyte layer was added to 100 µL of pretreatment solution in a reaction cuvette of the BM6010/C for haemolysis. In this process, haemoglobin was oxidized to methemoglobin and 12 µL of the haemolysed solution was dispensed to another reaction cuvette in which reagent 1 of the BM Test HbA1c had been previously dispensed. In this first reaction, glycated dipeptide (fructosyl-valine-histidine) was generated from the N-terminus of the beta-chain of haemoglobin by the reaction with protease. Then azide-methemoglobin was generated from the methemoglobin by the reaction with sodium azide. Next, the absorbance of azide-methemoglobin was measured for Hb concentration.
In the second reaction, after 30 µL of reagent 2 of the BM Test HbA1c was added to the cuvette, the glycated dipeptides (fructosyl-VH) reacted with fructosyl peptide oxidase (FPOX), generating hydroperoxide. The hydroperoxide allowed 10-(carboxymethylaminocarbonyl)-3,7-bis (dimethylamino) phenothiazine sodium salt (colouring agent) to develop a colour in the presence of peroxidase. The absorbance was measured to obtain the HbA1c concentration. The measurement value of HbA1c is calculated as the ratio of HbA1c concentration to Hb concentration. The result can be demonstrated either by IFCC unit (mmol/mol) or NGSP(%) on the BM6010/C, thus NGSP(%) is used in this study.
The expression unit of IFCC (mmol/mol)
12
and NGSP(%) according to the following equation
13
was calculated using both results of Hb and HbA1c concentration.

Statistical processing
Microsoft Excel 2003 was used for statistical processing.
Details of evaluation
Tip position of sample probe
The manufacturers’ instructions for use of the BM Test HbA1c indicate that the blood sample must be centrifuged at 800 g for 5 min in order to allow sampling from the packed erythrocyte layer. However, the instructions do not indicate the tip position of the sample probe in the layer.
In order to optimize the tip position of the sample probe, 98 samples from hospital employees who presented for an annual health checkup were used. EDTA-2 K was added to each sample and they were centrifuged at 800 g for 5 min, as instructed by the manufacturer. Then, the height of the packed erythrocyte layer of each sample was measured. Overall,119 blood samples were centrifuged at 800 g for 5 min for measurement of each sampling position (1, 3, and 5 mm from the bottom of the sample tube). The measured values were compared with those of the Tosoh G7. Significance was tested by the t-test (paired two sample t-test for means).
Precision
Intra-assay precision was evaluated by measuring the BM Test HbA1c Control (JEOL Ltd., Tokyo, Japan) of two different concentrations 20 times. Inter-assay precision was evaluated by measuring the same control samples for 10 days and the human blood samples in two concentrations for nine days.
Linearity
Linearity was evaluated by preparing 10 mixing ratio series from two samples: one with a low HbA1c value and one with a high value. The range of linearity was verified by running duplicate measurements for each specimen.
Interference of chemically modified derivatives of Hb and labile HbA1c
Five dilution ratio series specimens were prepared: acetylsalicylic acid and sodium cyanate up to 500 mg/L for the evaluation of chemically modified derivatives of Hb and glucose up to 10 g/L for the evaluation of labile HbA1c. The specimens were added to patient samples and incubated at 37℃ for 1 h. Interference of acetylated Hb, carbamylated Hb and labile HbA1c were evaluated by running duplicate measurements for each prepared specimens.
Interference of Hb variants
Twenty-four samples of Hb variants were provided by the Diabetes Diagnostic Laboratory, University of Missouri, School of Medicine. The measured values from the BM Test HbA1c were compared with those from the Primus HPLC to verify interference of Hb variants. The Wilcoxon test was used to check for a significant difference.
The samples included the following: six samples with HbC, six samples with HbD, six samples with HbE and six samples with HbS.
Accuracy
Accuracy was evaluated by running five replicates for each level using IFCC HbA1c Control Set (HBA-IFCC-control: Lot Berlin 2011.108). The mean of the obtained measurement was compared with the assigned value (NGSP%). The comparison was evaluated by the NGSP criterion, which defines the relative error to be within ±7%. 14
Correlation analysis with routine laboratory samples
To conduct the correlation analysis, we evaluated 351 patient samples obtained for routine laboratory test and compared the results of the BM Test HbA1c with those of the Tosoh G7 which we used as the comparative method.
Results
The tip position of sample probe
The average height of the packed erythrocyte layer of 98 samples of our hospital employees was 14.1 mm and the standard deviation was 1.52 mm. The lowest observed value was 11 mm. Considering the height of the packed erythrocyte layer of anaemic patients, we determined that the appropriate tip position of the sample probe should be half of the lowest value, which was 5.5 mm or less. Based on this presumption, the tip positions of the sample probe were set at 1 mm (the default value on the BM6010/C), 3 mm and 5 mm from the bottom of the sample tube to compare the measurement values by the BM Test HbA1c and those by the Tosoh G7.
Result of HbA1c measurements by the BM6010/C at various sampling positions and Tosoh G7.
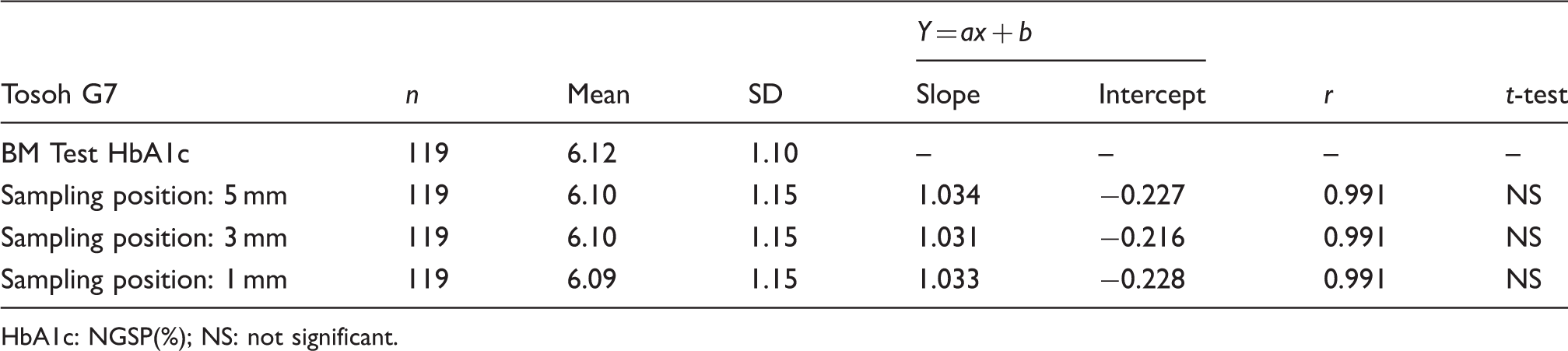
HbA1c: NGSP(%); NS: not significant.
Precision
The coefficient of variation (CV) of intra-assay precision was 0.9% (mean:HbA1c, 4.96%) for control low and 0.5% (mean:HbA1c 9.82%) for control high. The CVs of inter-assay precision were 1.2% (mean:HbA1c, 5.00%) for control low, 0.6% (mean:HbA1c, 9.89%) for control high, 1.0% (mean:HbA1c, 6.03%) for human sample 1, and 0.7% (mean:HbA1c, 10.25%) for human sample 2.
Linearity
The linearity range of measured values of the mixing ratio series was verified from 5.3 to 17.0 (NGSP%).
Interference of chemically modified derivatives of Hb and labile HbA1c
No interference was observed from the chemically modified derivatives of Hb including acetylated Hb and carbamylated Hb up to the maximum concentration of 500 mg/L or labile HbA1c up to the maximum concentration of 10 g/L.
Interference of Hb variants
Based on the correlation analysis results for Hb variants, the correlation coefficient (r) was 0.997. The linear regression formula was (BM Test HbA1c) = 1.011 × (Primus HPLC) − 0.179 (Figure 1). No significant difference was observed between the Primus HPLC and the BM Test HbA1c according to the Wilcoxon test (P < 0.01).
Correlation of Hb variants measurement data.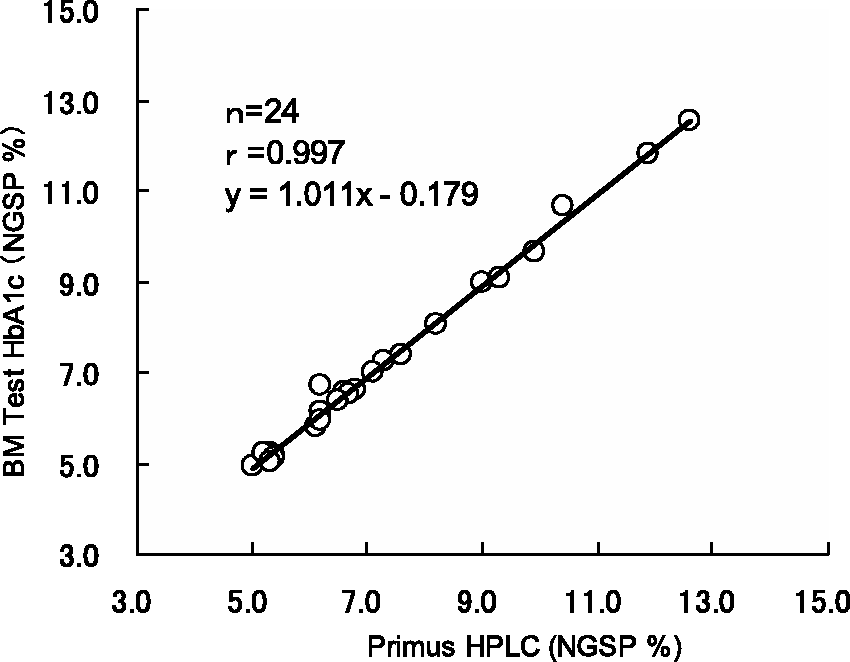
Accuracy
Accuracy evaluation using the IFCC HBA1c control.
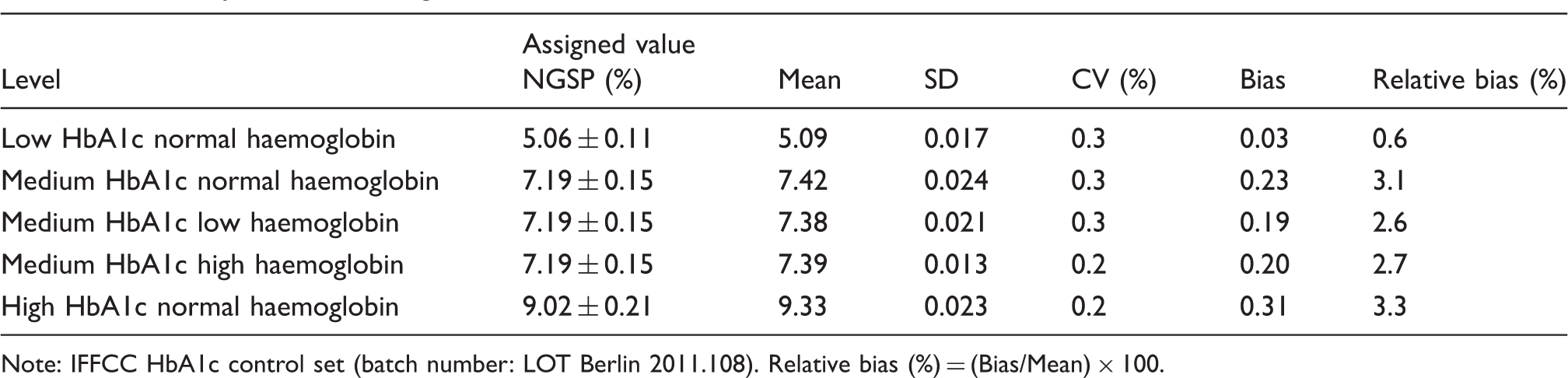
Note: IFFCC HbA1c control set (batch number: LOT Berlin 2011.108). Relative bias (%) = (Bias/Mean) × 100.
Correlation analysis with routine laboratory samples
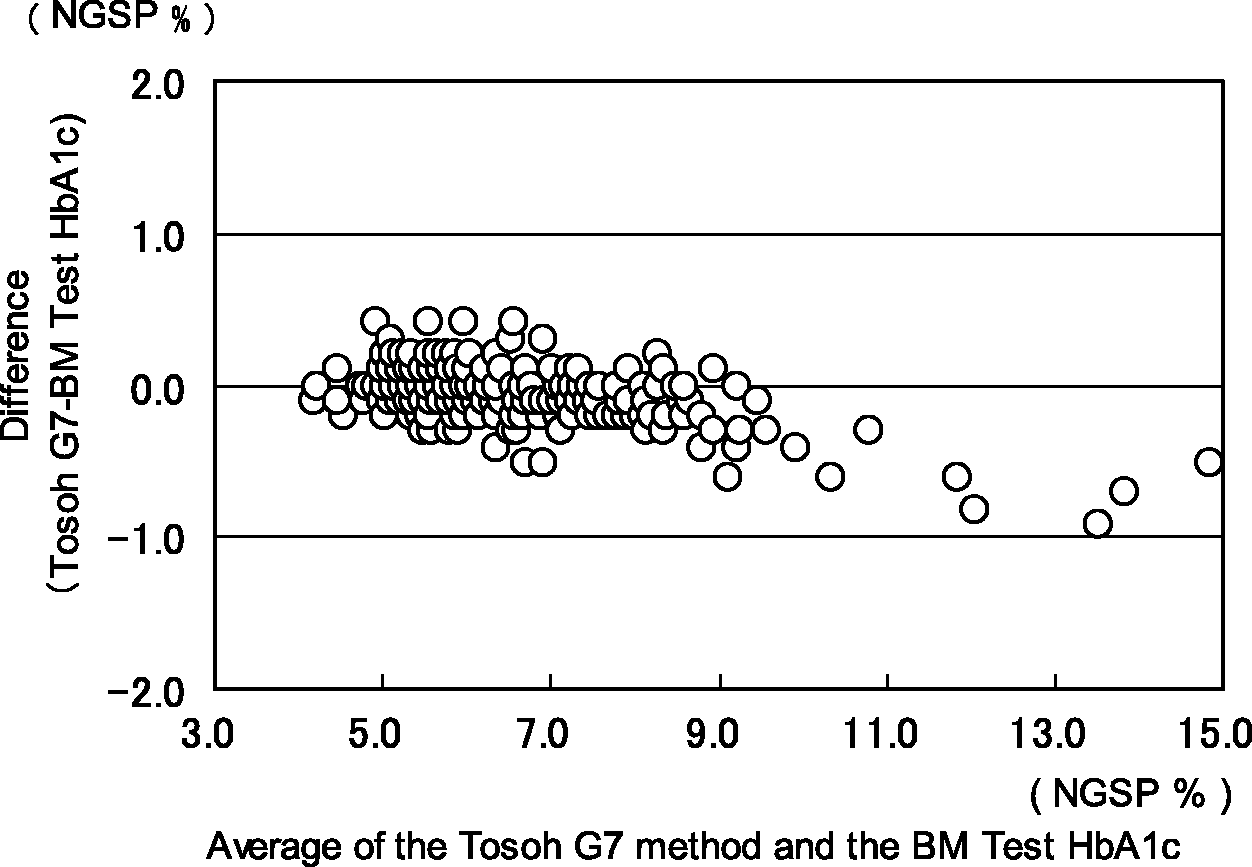
According to the result of the correlation analysis, r = 0.994. The linear regression equation was (BM Test HbA1c) = 1.067 × (Tosoh G7) − 0.379 (Figure 2). The proportional systematic error was observed in the Bland–Altman plot (Figure 3).
Correlation between HbA1c measurements obtained by the BM Test HbA1c and the Tosoh G7. Bland–Altman plot comparing the HbA1c measurements obtained by the BM Test HbA1c and the Tosoh G7.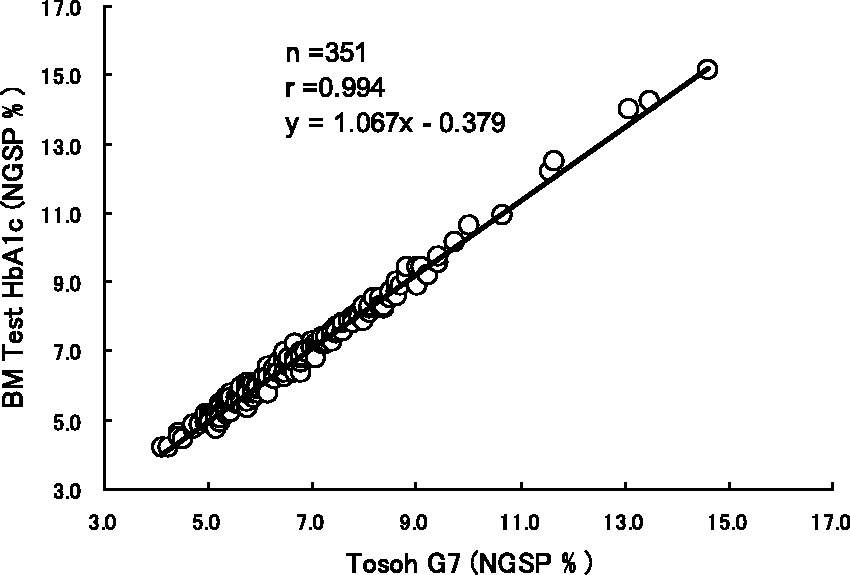
Discussion
In this study, we evaluated the measurement performance of the BM Test HbA1c by using the automated analyser BM6010/C with an on-board haemolysis system. Firstly, it was proved that there was no fluctuation in the measurement results if the tip position of the sample probe was within 5 mm from the bottom of sample tube in order to aspirate the sample from the centrifuged packed erythrocyte layer. However, the following points must be noted, even if the tip position of the sample probe was set at less than 5 mm. If the tip position of the sample probe was set at 1 mm, the fibrin clot, which cannot be seen by the naked eye, but is precipitates at the bottom of the tubes after centrifugation, could interfere with sample aspiration. If the tip position was set at 3 mm or 5 mm, it would not be possible to sample from a lower erythrocyte layer from samples of patients with anaemia or from samples whose volume was less than the required amount. If the tip position of the sample probe was set greater than 5 mm, the probe might not reach the erythrocyte layer of samples from patients with anaemia. In order to avoid such obstacles, it is important to avoid sampling at 1 mm from the bottom of the tubes, carefully observe the height of erythrocyte layer and Hb concentration measured by the BM Test HbA1c, and check the nature and volume of the collected samples. Based on the above findings, we set the tip position of our sample probe at 3 mm for routine laboratory tests.
It has been reported that the non-uniformity of the HbA1c values observed in the samples that were centrifuged at 2000 g for 5 min was due to the non-uniformity of specific gravity of erythrocytes caused by senescence and biochemical changes.15,16 However, the samples that were centrifuged at 1000 g or less for 5 min or less did not show such phenomena. 16 Therefore, we considered that the HbA1c results obtained after centrifugation at 800 g for 5 min are not affected by the non-uniformity of specific gravity of erythrocytes.
The anchor of traceability of the BM Test HbA1c is the IFCC reference method and the measuring object is glycated N-terminal residue of the β-chain of Hb, which is the same as the IFCC reference method. Despite the difference that the detection molecule of the BM Test HbA1c is dipeptide while that of the IFCC reference method is hexapeptide, the measurement results were in accordance with the IFCC reference method. Likewise, the results of the accuracy evaluation test indicated that the bias against the assigned values using the IFCC HbA1c control set was 0.03–0.31% and its relative error (%) was 0.6–3.4%, which is within the NGSP criterion of ± 7%.
The result of correlation analysis between the BM Test HbA1c and the Tosoh G7 using the routine samples indicates the proportional systematic error, which was observed in the Bland–Altman Plot (Figures 2 and 3). However, this tendency is deemed to be in the allowable range because those biases were within the NGSP criterion of ± 7% (relative).
We observed that chemically modified derivatives of Hb, such as acetylated Hb and carbamylated Hb, which we encounter in clinical practice, did not interfere with the measurement of HbA1c. Likewise, labile HbA1c did not interfere. These outcomes prove that this measurement system is beneficial for patients who are taking aspirin or who are receiving dialysis as outpatients to control glucose levels as well as patients who have diabetes mellitus.
The interference of Hb variants was verified using 24 samples of Hb variants for correlation analysis with the Primus HPLC, which is not affected by Hb variants. Based on the results of the correlation analysis and the Wilcoxon test, we concluded that the BM Test HbA1c is not affected by Hb variants.
Conclusions
The development of BM6010/C with an on-board haemolysis system has optimized the tip position of sample probe and elimination of troublesome manual pre-treatment. These features are thought to immensely contribute to the shorter measurement time and better accuracy of measurement results.
In addition, since BM6010/C is a general automatic analyser, it also has an advantage in constructing a consolidated system if it simultaneously measures other assays such as glucose when using the BM Test HbA1c.
Considering such features and advantages, this measurement system will offer an excellent cost-and-time effective method to the patients and people who undergo medical screenings by providing the shorter measurement time and shorter turnaround time compared with the conventional HPLC method.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
None.
Guarantor
MK.
Contributorship
All authors contributed to the study and the writing of this manuscript.