
Abstract
Objective:
Surgical management of head and neck cancer (HNC) can result in significant functional deficits. Large tumors of the oral cavity may require extensive resection and the need for microvascular free-flap reconstruction involving the use of adynamic tissue. This may result in oral incompetence, drooling, and unsatisfactory esthetic outcomes. Maintenance of the orbicularis oris and function of the oral sphincter are important objectives in the reconstruction of large defects. When this cannot be accomplished, secondary local flaps can be employed to restore the orbicularis oris.
Methods:
We present 2 cases of oral incompetence following microvascular free- flap reconstruction for large resections of HNC.
Results:
All cases were managed with debulking of flap, modified Karapandzic flaps, and advancement of composite skin, muscle, and buccal mucosa to restore the function of the oral sphincter and improve oral competence. The surgical techniques demonstrated in our cases resulted in improvement in both functional and esthetic outcomes.
Conclusion:
Restoring continuity of the orbicularis oris muscle is a critical functional and esthetic consideration in microvascular free flap reconstruction where the lip is involved or disrupted. However, when this cannot be achieved, restoration of the oral sphincter and oral commissure can be achieved with a secondary reconstructive procedure.
Keywords
Introduction
Large tumors of the oral cavity can require extensive resection and the need for microvascular free flap reconstruction. 1 Single stage free flap reconstruction involves the use of adynamic tissue, and when used to replace the orbicularis oris, can result in oral incompetence, drooling, difficulties with speech, and unsatisfactory esthetic outcomes.2-4 Maintenance of the orbicularis oris and function of the oral sphincter are important objectives in the reconstruction of large defects. 5 However, when this cannot be accomplished, secondary local flaps can be employed to restore the orbicularis oris. We present 2 cases demonstrating reconstruction of the oral sphincter following free flap reconstruction for resections of head and neck cancer.
Case 1
A male patient in his 70s with a history of tobacco use presented with oral incompetence, drooling, and poor speech following osteocutaneous radial forearm free flap reconstruction after right oral composite resection including the buccal mucosa, and upper and lower lips. Orbicularis oris restoration was not possible during primary reconstruction with radial forearm free flap. Following primary reconstruction, the free flap made up one-fourth of the right upper lip, one-third of the right lower lip, and the oral commissure (Figure 1A). The patient completed adjuvant radiation therapy 1 year prior to revision. A composite flap of the native lower lip extending from the mental sulcus to the left melolabial fold was first elevated with preservation of the nerves and vessels supplying the orbicularis oris muscle. The highest portion of the microvascular reconstruction was debulked and de-epithelialized to allow inset of the modified Karapandzic over the flap. Advancing the modified Karapandzic over the de-epithelialized flap allowed for restoration of the oral sphincter without significant microstomia (Figure 1B and C). A full thickness incision was then made through the skin and subcutaneous tissue of the upper lip to create bilateral advancement flaps that were advanced and rotated to eliminate notching of the upper lip. Postoperatively, the patient had significant clinical improvement (Figure 1D). The patient underwent an additional modified Karapandzic flap of the right upper lip the following year with significant improvement to oral competence at 6-months. (Figure 1E-G).
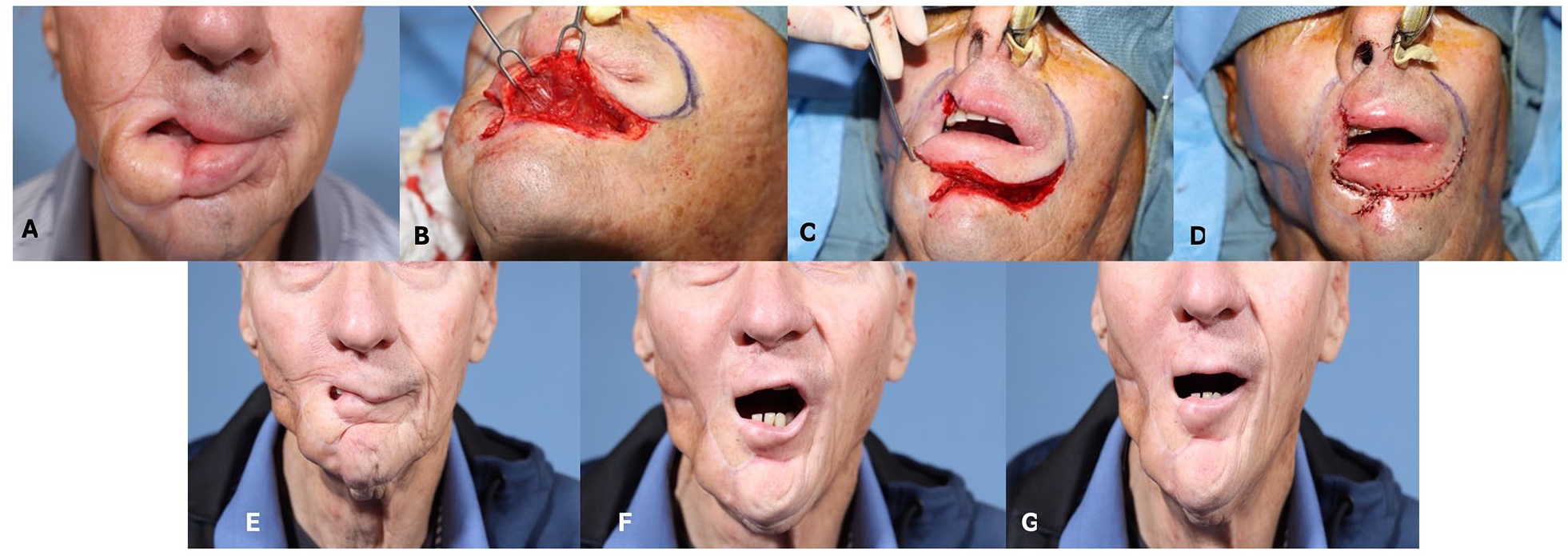
(A) Pre-operative photo following osteocutaneous radial forearm free flap for buccal and skin reconstruction with resulting oral incompetence. (B) and (C) modified Karapandzic flap advanced over free flap to establish neo-commissure for restoration of oral sphincter. (D) Immediate post-operative reconstruction of oral sphincter. (E) to (G) 6 months post-operative result following additional Karapandzic of the right upper lip.
Case 2
A 63-year-old patient presented with oral incompetence and dysphagia following anterolateral thigh (ALT) flap reconstruction for a left composite resection, resection of the buccal mucosa, oral commissure, lip, and cheek skin. The ALT was used for internal and external reconstruction in a folded fashion, and thus lacked the continuous muscular sphincter needed for oral competence (Figure 2A). The patient did not receive adjuvant radiation therapy. Following initial flap debulking, modified Karapandzics of the upper and lower lip were performed to mobilize the orbicularis oris muscle to restore the upper and lower lips and oral commissure. Skin incisions were made externally along the labiomental sulcus and nasolabial junction (Figure 2B). Mucosal incisions were made to mimic the external incisions to allow advancement of the flap. As much as possible, orbicularis oris fibers, nerves, and vasculature were preserved unless they greatly prohibited movement. The flaps were advanced laterally to form a neo-commissure. Postoperatively, the patient had significant clinical improvement.

(A) Pre-operative photo of patient following anterolateral thigh flap reconstruction after composite, buccal mucosa, and skin resection, which resulted in oral incompetence. (B) Post-operative photo following modified Karapandzic flap with resulting neo-commissure and restoration of muscular sling.
Discussion
Ideal reconstruction after oral cavity cancer involving the lip includes maintaining the oral commissure, optimizing the oral aperture’s size, preserving the orbicularis oris muscle, and maintaining the skin’s sensation.4,5 When continuity of the orbicularis oris muscle cannot be achieved, the oral sphincter and oral commissure can be restored with a secondary reconstructive procedure. The surgical techniques demonstrated in the cases above resulted in improvements in both functional and esthetic outcomes. Both patients reported a reduction in drooling and improved oral competence at 1 week, 6 months, and 1 year postoperatively. Thus, modified Karapandzic flaps can be used as secondary procedures for restoration of oral competence following reconstruction with a single-stage microvascular free flap.
Footnotes
Data Availability Statement
Data supporting this study cannot be made available due to protection of patient privacy
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved under a non-research exemption by the Institutional Review Board at Vanderbilt University Medical Center (IRB #241090).
Presentation Disclosure
This manuscript was presented in poster format at The Triological Society 2023 Combined Sections Meeting in Coronado, California, January 26 to 28, 2023