
Abstract
Occipital nerve stimulation (ONS) has been employed off-label for medically refractory head pain. Identification of specific headache diagnoses responding to this modality of treatment is required. Forty-four patients with medically refractory head pain and treated with ONS were invited to participate in a retrospective study including a clinical interview and, if necessary, an indomethacin test to establish the headache phenotype according to the International Classification of Headache Disorders, 2nd edn (ICHD-II). We gathered data from questionnaires before implantation, at 1 month after implantation, and at long-term follow-up. Twenty-six patients consented and were phenotyped. At 1 month follow-up and at long-term follow-up a significant decrease in all pain parameters was noted, as well as in analgesic use. Quality of sleep and quality of life improved. Patient satisfaction was generally high as 80% of patients had ≥ 50% pain relief at long-term follow-up. The overall complication rate was low, but revisions were frequent. After phenotyping, two main groups emerged: eight patients had ‘Migraine without aura’ (ICHD-II 1.1) and eight patients ‘Constant pain caused by compression, irritation or distortion of cranial nerves or upper cervical roots by structural lesions’ (ICHD-II 13.12). Overuse of symptomatic acute headache treatments was associated with less favourable long-term outcome in migraine patients. We conclude that careful clinical phenotyping may help in defining subgroups of patients with medically refractory headache that are more likely to respond to ONS. The data suggest medication overuse should be managed appropriately when considering ONS in migraine. A controlled prospective study for ONS in ICHD-II 13.12 is warranted.
Introduction
Headache is among the most common reasons for patients to seek medical care. Migraine, the most common form of disabling primary headache, has been estimated to be the most costly neurological disorder in the European Community (1). Although considerable developments have been made in understanding and treating primary headache, there remains a group of patients with difficult to treat headache problems, labelled generically as medically intractable headache (2). In general terms these patients have frequent, daily or near-daily headache unresponsive to medical therapy. Neuromodulation methods may offer an opportunity to address the needs of these highly disabled patients. In a landmark paper, Weiner and Reed described excellent outcomes with occipital neurostimulation (ONS) in 12 patients described as having occipital neuralgia (3). On clinical review of this patient cohort and using the International Classification of Headache Disorders, 2nd edn (ICHD-II) (4), it became clear that most of them had chronic migraine and one had hemicrania continua. A subsequent positron emission tomography study in those with chronic migraine (5) demonstrated persistent activation of the dorsolateral pons, as is seen in other imaging studies of migraine (6), and activation of thalamus structures when the device was activated.
Given that there has been off-label use of ONS on compassionate grounds in highly disabled patients, there is an opportunity to classify those patients using the ICHD-II in order to identify potential patient groups for systematic study. Recent experience with chronic cluster headache suggests that ONS may be help that disorder (7,8). Indeed, other modalities of stimulation have begun to be used in chronic cluster headache, specifically deep brain stimulation, and these are also proving highly promising (9). Data from the first randomized, controlled, prospective trial for ONS for the Treatment of Intractable Migraine headache (ONSTIM trial) have recently become available in abstract form (10). The results indicate that ONS may be a promising treatment for some intractable chronic migraine patients, and further controlled trials are required. Interestingly, given the hemicrania continua patient in Weiner and Reed's initial cohort (3), there are nine cases of hemicrania continua treated with ONS now reported in the literature, and seven benefited from the therapy (11–13). These cases are important, since hemicrania continua is an indomethacin-sensitive headache, which broadens still the range of headache types that may benefit from this approach. Results of ONS in primary headache disorders have recently been reviewed (14).
In this retrospective study a cohort of patients, implanted with occipital neurostimulators at a single site, were invited to attend clinical evaluation and, if necessary, to undergo an indomethacin test in order to clarify the diagnosis. We confirm other reports that chronic migraine patients can be treated with this approach, adding a note of caution around medication overuse, and identify a previously unreported group, Upper Cervical Neuropathic Pain (ICHD-II, 13.12), who have a promising outcome. This work was presented in preliminary form at the 10th Congress of the European Federation of Neurological Societies (Brussels, August 2008 (15)).
Methods
Forty-four patients had been consecutively treated with ONS for medically refractory headache between April 2000 and December 2006 at the AZ Nikolaas Pain Clinic (J-P.V.B, Fig. 1). ONS therapy was offered to these patients as part of the regular pain programme, and the decision to offer this treatment to the patient was made by the pain physician based on a working diagnosis of occipital neuralgia or cervicogenic headache, and after all patients had undergone a preoperative psychological evaluation. The Ethics Committees of the Ghent University Hospital in Ghent and the AZ Nikolaas in Sint-Niklaas approved the study (EC/2006/383). Informed consent was sought from all patients by letter to review their clinical data, including a pre-implantation questionnaire, a questionnaire at 1 month following trial stimulation (i.e. before the definitive implantation procedure), as well as technical details: implantation date and procedure; complications such as dislocations, lead fractures, electrical leakage at the connections and infection; and battery replacement. The patients were invited by letter to be interviewed by an independent and blinded headache neurologist at the Department of Neurology of the Ghent University Hospital (K.P.). If necessary to make a specific headache diagnosis, patients were invited to give their informed consent to undergo an indomethacin test, either intramuscular or oral. The indomethacin tests were performed by the treating physician at AZ Nikolaas Pain Clinic (J-P.V.B.). Patients who entered the study were finally invited to fill out the post-implantation questionnaire for a second time at their last visit at AZ Nikolaas Pain Clinic, to obtain long-term follow-up data.
Study outline.
Implantation technique
Initially, the implantation technique described by Weiner and Reed (3) was used. A subcutaneous lead was inserted towards the midline via a lateral incision close to the mastoid process. The procedure was done under propofol sedation with a wake up during the procedure in order to check the area of paraesthesia. With growing experience the technique was adapted and the ONS procedure is now performed under general anaesthesia with the patient in the prone position and the head in a horseshoe headrest. The incision was made close to the occiput, where there is more fat tissue that affords a subcutaneous pocket substantial enough for adequate fixation of the lead and leaving a loop. A curved needle (custom made by Medtronic Inc., Bakken Research Centre, Maastricht, the Netherlands) was pushed from the occiput towards the mastoid process in the subcutaneous tissue, to cross the greater, lesser and least occipital nerve. The position of the lead was checked with fluoroscopy after the needle had been pulled out. An intermediate incision was made in the suprascapular area, again creating a pocket, and a second loop was left behind. A third incision was made parallel to the spine at the high thoracic level to bury the connection between the lead and the temporary extension lead. The connection was fixated to the underlying tissue. The temporary extension lead was tunnelled laterally over the thoracic wall. After a successful trial period of at least 1 month, a pocket was created in the gluteal area for the implantable pulse generator, a new extension lead was tunnelled towards the connector and the new connector was secured to the underlying tissue. Stimulation parameters, including frequency, pulse width and voltage, were adjusted so that all patients experienced mild paraesthesia in the stimulated area.
Pain questionnaires
The pre- and post-implantation questionnaires were developed in 1997 by the Belgian Pain Society (the Belgian Chapter of the International Association for the Study of Pain). Pain data are gathered with a visual analogue scale (VAS), but the questionnaire has otherwise not been validated. These evaluation forms are required by the Belgian government for reimbursement of all patients with chronic pain treated with implantable devices (neurostimulators and intrathecal drug-delivery pumps). The questionnaires include data on regional distribution of the pain using a pre-printed drawing of the head and body, pain severity scores on a VAS from 0 to 10 indicating ‘pain at present’, ‘worst pain last week’, ‘lowest pain last week’, ‘average pain last week’, percentage pain-free time (0–100%), average daily number of analgesics used, quality of sleep on a scale from 1 to 5, influence of pain on activities of daily living, social activities, independence of others, hobbies and need for bed rest (all the five using VAS scores on a scale from 0 to 10). The post-implantation questionnaire was filled out by every patient after 1 month of stimulation and by 21 patients at long-term follow-up. This questionnaire included data on the subjective area of stimulation on a pre-printed drawing, perceived pain relief (‘worse’, ‘too little’, ‘moderate’, ‘largely’, ‘almost complete’, ‘complete’), patient satisfaction (‘excellent’, ‘very good’, ‘good’, ‘moderate’, ‘poor’, ‘no effect’ or ‘worse’), and the question whether the patient would undergo the procedure again for the same indication, but was otherwise identical to the pre-implantation questionnaire.
Clinical interview
During the clinical interview demographic data, analgesic use, all necessary information to make a headache diagnosis according to ICHD-II (4), as well as percentage of pain relief at long-term follow-up, were recorded. To make a diagnosis of medication overuse headache the Appendix Criteria were used (16). Patients were instructed not to discuss their pre-implantation diagnosis. All clinical data were made available to a second blinded headache neurologist (P.J.G.) before clinical diagnoses were assigned.
Indomethacin testing
To exclude a diagnosis of paroxysmal hemicrania or hemicrania continua an intramuscular indomethacin test was performed in some patients with strictly unilateral (attacks of) head pain (17). Intramuscular indomethacin tests were performed at the Pain Clinic of AZ Nikolaas. Patients had their stimulator turned off in the morning and recorded pain on a VAS from 0 to 10 for 3 h in a diary. If the head pain reached an intensity of ≥ 5/10 on the VAS, 100 mg indomethacin was injected intramuscularly. Pain scores were recorded each hour afterwards for the rest of the day. Afterwards the patients received instructions to switch the stimulator back on. If the head pain reached an intensity of < 5/10 during the 3-h observation period, instructions were given to perform an ambulatory oral indomethacin test. Patients would record headache intensity on an hourly basis in a headache diary while under indomethacin. Indomethacin was started at 25 mg three times per day for 3 days. If the patient was not pain free, the indomethacin dose was increased to 50 mg three times per day for 3 days. If the patient was not pain free, the indomethacin dose was further increased to 75 mg three times per day for 3 days. If the patient was not completely pain free at that point in time, the oral indomethacin test was deemed negative. Exclusion criteria for an indomethacin test were asthma, renal disease, allergy to acetylsalicylic acid or non-steroidal anti-inflammatory drugs, active peptic ulcer disease and pregnancy.
Data analysis
Statistical analysis of the data was performed by an independent statistician (G.V.M.) with R, a language and environment for statistical computing (18). Univariate comparison of unpaired groups was done with Fisher's exact test for categorical data and the non-parametric Mann–Whitney U-test for the comparison of continuous variables. The non-parametric Friedman two-way ANOVA test with Wilcoxon matched-pairs signed-ranks test as multiple range test was used to compare measurements over the three time intervals. The significance level was set at α = 0.05, two-tailed.
Results
All 44 patients consented to have their data used from the questionnaires pre-implantation and at 1 month post-implantation. Twenty-six patients consented to undergo clinical interview, which took place at the Neurology Department of the Ghent University Hospital between December 2006 and April 2007. Data from the questionnaire at long-term follow-up were additionally obtained from 21 of these 26 patients. One patient's records (including all three questionnaires) could not be retrieved, but the patient (no. 6) presented for the clinical interview.
Overall safety in all 44 patients
The mean age of all 44 patients at implantation was 48 years (range 29–75). All 44 patients had an occipital component to their head pain and 18 also had a trigeminal component. Twenty-one patients underwent unilateral neurostimulation, 10 on the left, 11 on the right, and 23 had bilateral neurostimulation, using one electrode in 19 and two electrodes in four. The mean duration of follow-up was 36 months (range 7–87 months). The total device time was 1592 months. Fourteen of the 44 patients had a total of 18 revisions. Eleven patients had to have a new lead put in place, in two patients because of dislocation, using the initial technique with a lateral incision (cf. Methods section), and in the other nine patients because of lead fracture, with four of these patients undergoing a second revision, again lead replacement. In three cases there was a problem with the connection, with pain due to local current leakage, requiring opening of the connection and cleaning it. There were two instances of infection, one at the level of the lead insert during the trial period, and one later after implantation at the level of the connector due to a small skin defect. Both infections were resolved with short-term antibiotic treatment.
Pooled results for the 26 phenotyped patients
Pooled results for the twenty-six phenotyped patients
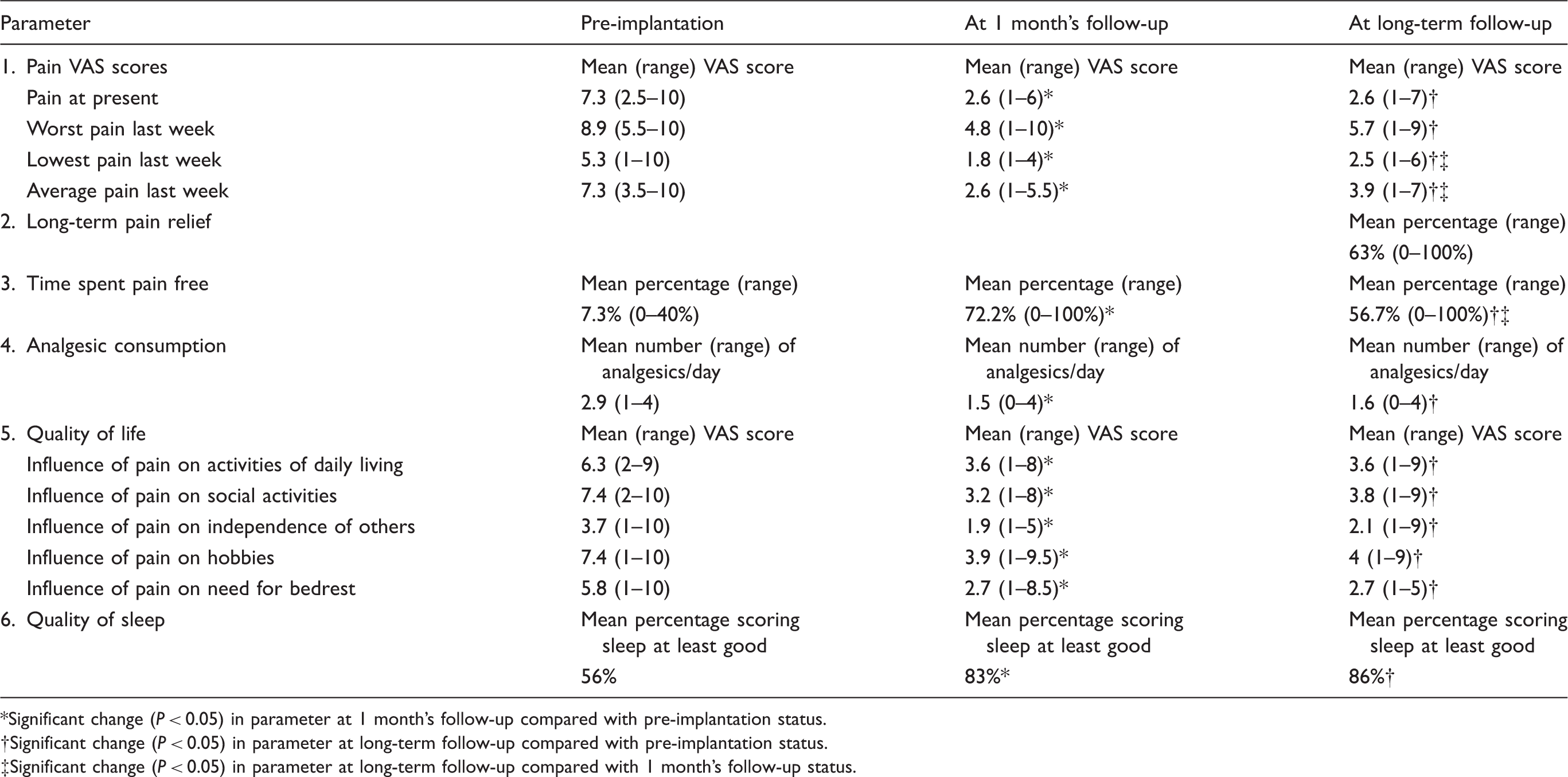
Significant change (P < 0.05) in parameter at 1 month's follow-up compared with pre-implantation status.
Significant change (P < 0.05) in parameter at long-term follow-up compared with pre-implantation status.
Significant change (P < 0.05) in parameter at long-term follow-up compared with 1 month's follow-up status.
Data from questionnaires on all available parameters were compared between patients who volunteered for a clinical interview (n = 26) and those who did not (n = 18) at baseline and at 1 month's follow-up. There were no significant differences except for the included patients being older (average of 51 vs. 44 years old), having less influence of pain on activities of daily living and hobbies at baseline, and having less influence of pain on hobbies at 1 month's follow-up.
Clinical phenotyping
The mean age of the 26 patients who were phenotyped was 51 years at the time of implantation (range 29–75). There were 14 women and 12 men in this group. An indomethacin test was proposed to six patients, of whom two refused. All four indomethacin tests, of which two were oral and two intramuscular, were negative. The clinical diagnoses for all 26 patients fell into nine ICHD-II categories (Fig. 1). Two main subgroups were identified: eight patients with migraine without aura (ICHD-II 1.1) and eight patients with ‘Constant pain caused by compression, irritation or distortion of cranial nerves or upper cervical roots by structural lesions’ (ICHD-II 13.12). All patients with migraine without aura had an additional diagnosis of medication overuse headache prior to implantation. All migraine patients failed at least four classes of preventive medicines, of which at least three were a β-blocker, anticonvulsant, calcium channel blocker or tricyclic antidepressant, thus fulfilling current criteria for medical intractability (2). We compared all available data between the two groups ICHD-II 1.1 and ICHD-II 13.12 and found that there were few significant differences, except that patients with ICHD-II 13.12 had significantly more pain relief (mean 80% vs. 47%; n = 8 in both groups) at long-term follow-up, and that migraine patients were more independent of others at 1 month's follow-up (n = 8 in both groups). The latter difference was not seen at long-term follow-up.
Patients with migraine
The eight migraine patients had a mean follow-up of 24 months following implantation (range 12–60 months). Patient satisfaction at 1 month's follow-up was rated excellent by one, very good by two and good by five. At long-term follow-up one patient indicated no effect, one only moderate effect, one a good effect, three very good and one excellent (missing data in one patient). At 1 month's follow-up every patient would undergo a repeat of the procedure, but at long-term follow-up two out of seven patients would not (missing data in one patient). Grouped data from the questionnaires at 1 month and long-term follow-up were compared with the data pre-implantation. There was a significant reduction on most pain parameters (‘actual pain’, P = 0.00557; ‘least pain last week’, P = 0.0118; ‘mean pain last week’, P = 0.00952; ‘% pain free’, P = 0.00298) except for the ‘worst pain in the last week’ (P = 0.0539). The absolute average value for ‘mean pain last week’ decreased from 7/10 VAS score pre-implantation to 2.4/10 and 4/10 at 1 month and long-term follow-up, respectively. Five out of seven patients (missing data in one) had at least a three-point drop in ‘mean pain last week’ at long-term follow-up. The use of analgesics was significantly diminished (P = 0.0469). Influence of pain on most activity parameters was not significantly changed, except for an increase in social activities (P = 0.0262). Quality of sleep was not significantly changed. There were no significant differences between the data at 1 month's follow-up vs. long-term follow-up, except for a decrease in percentage of time spent pain free at long-term follow-up, which decreased from 71 to 51% (P = 0.04983).
Details of migraine patient outcomes
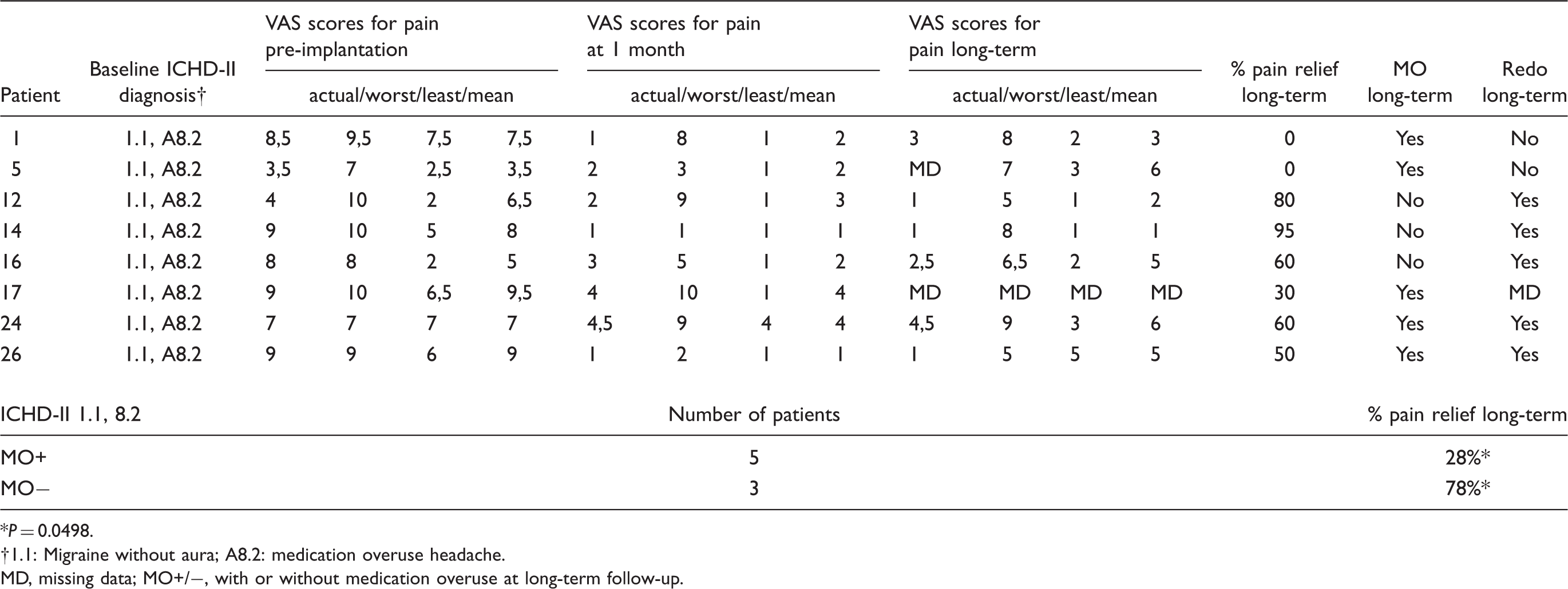
P = 0.0498.
1.1: Migraine without aura; A8.2: medication overuse headache.
MD, missing data; MO+/−, with or without medication overuse at long-term follow-up.
Head pain of cervical origin
Details of outcome of patients suffering from ICHD-II 13.12—Upper Cervical Neuropathic Pain

Not sign.
13.12: Constant pain caused by compression, irritation or distortion of cranial nerves or upper cervical roots by structural lesions.
MD, missing data; MO+/−, with or without medication overuse at long-term follow-up.
Other headache diagnoses
Outcome data for all other patients

1.2.1: Typical aura with migraine headache; 1.6.1: Probable migraine without aura; 3.1.2: Chronic cluster headache; 4.8: New daily persistent headache; 5.2.2: Chronic post-traumatic headache attributed to mild head injury; 5.4: Chronic headache attributed to whiplash injury; 13.12: Constant pain caused by compression, irritation or distortion of cranial nerves or upper cervical roots by structural lesions; A8.2: Medication overuse headache; NC, not classifiable; MD, missing data.
Discussion
The data presented suggest that for some subgroups of patients with relatively medically refractory headache ONS offers an effective, well-tolerated and comparatively safe approach to management. Certainly in this very disabled group such a development would be welcome. The data provide support for the further study of ONS in migraine and caution investigators to monitor carefully for the potential effects of medication overuse when studying ONS. Perhaps more important, a cohort of patients with what may be described as Upper Cervical Neuropathic Pain (ICHD-II, 13.12), is identified. This finding is important, first, because the patients did well, and second, because such patients may not always come to the attention of neurology and headache specialists thinking about this new treatment modality. An important feature of our cohort has been the very careful phenotyping of the cases, including indomethacin testing, to provide as clear diagnoses as possible. ONS is a promising therapy for a range of patients, with challenges both to identify candidates and to conduct appropriately blinded randomized controlled trials.
Peripheral nerve stimulation, which is a minimally invasive and reversible procedure, is increasingly employed in the treatment of certain forms of chronic neuropathic pain and certainly preferred over nerve ablation procedures (19). The mechanism of action is incompletely understood, but includes an inhibitory input within pain pathways, gate control of pain as well as modulation of neurotransmitters in the central nervous system (19,20). The technique of implantation of an occipital neurostimulator was pioneered by Weiner and Reed (3) to treat patients with pain that had an occipital focus. Off-label use of ONS has been employed on a compassionate basis for highly disabled patients with intractable headache, suffering from occipital neuralgia (21), chronic migraine (5) or transformed migraine (22), chronic cluster headache (7,8), hemicrania continua (12), post-traumatic headache and headache of C2 origin (23). ONS is considered a minimally invasive procedure and safety data are good (11). The rationale behind the technique in primary headache syndromes, such as migraine and cluster headache, is to modulate sensory traffic from the trigeminocervical complex (24,25), either at the level of the second-order neurons (26,27) or possibly in the thalamus (5). Given the loss of spatial specificity at the level of the trigeminocervical complex, electrical stimulation of the occipital nerve may have an anti-nociceptive effect in the territory of the trigeminal as well as the occipital nerves. Interestingly, stimulation of the greater occipital nerve in the rat reduces calcitonin gene-related peptide in the jugular blood, which is a biomarker of inhibition of the trigeminal system (28). In case of neuropathic pain in the occipital territory (ICHD-II 13.12), electrical stimulation of the sensory afferents may lead to suppression of Aδ- and C-fibres at the level of the spinal dorsal horn (29,30).
We embarked on this retrospective study to try to identify subgroups of patients with medically refractory headache with an increased likelihood of responding to ONS. Response to an occipital nerve block certainly is not useful in predicting the therapeutic effect of ONS (8,10,31). In this uncontrolled series all 44 patients had at least an occipital component to their head pain, and received uni- or bilateral ONS, mirroring the clinical distribution of the pain.
At 1 month's follow-up post implantation, patient satisfaction was generally high and all patients would theoretically undergo the intervention again for the same indication. Given the mean duration of follow-up of 3 years and a total device time of almost 1600 months, the overall complication rate of two infections is very low. However, at least one revision was needed in about 30% of patients because of technical problems, which included lead fracture, dislocation and connector current leakage. Some of these problems are due to the fact that the material used had not been designed for this purpose but for spinal cord stimulation. It is reassuring that not a single neurological deficit was created by the intervention. We only had two patients with a dislocated lead and not a single dislocation occurred after the technique was adapted by doing a medial incision, leaving loops at two stages and fixing the connector. These results are very favourable when compared with earlier results with lead dislocation in all patients after 3 years (11).
Twenty-six patients were phenotyped according to the ICHD-II criteria. At long-term follow-up 21 individuals indicated they experienced at least 50% pain relief. These 26 patients had a mean VAS reduction for ‘average pain last week’ of 4.7 at 1 month post implantation and of 3.4 at long-term follow-up. The overall satisfaction with the technique was high, except for three patients who had no pain relief at long-term follow-up. All three individuals, two migraine patients and one patient with new daily persistent headache, had ongoing medication overuse. When we compared available data from the 18 who were not phenotyped and the 26 who were, only few statistically significant differences were found, and these did not seem clinically important. For the rest of the discussion we speculate that our findings in the phenotyped patients are representative of the entire group.
After subanalysis, two main groups of patients were identified, i.e. migraine without aura and occipital neuropathic pain, coded in the ICHD-II under 13.12 ‘Constant pain caused by compression, irritation or distortion of cranial nerves or upper cervical roots by structural lesions’. Even though both groups consisted of only eight patients, and thus statistical power is low, some significant differences were found. It appears that ICHD-II 13.12 patients had a higher percentage pain relief at long-term follow-up. This result is influenced by two migraine patients with ongoing medication overuse headache who experienced no pain relief at long-term follow-up and who indicated they would not redo the intervention at that time. Indeed, the presence/persistence of medication overuse at long-term follow-up is associated with poor outcome in migraine patients, as the average pain relief for patients with medication overuse was much less than for those without at long-term follow-up. This finding is certainly consistent with the general concept that medication overuse renders migraine patients more resistant to prophylactic therapy. Thus, it appears that close monitoring of acute headache treatment is mandatory to ensure long-term benefit from the technique. Withdrawal of migraine patients from medication overuse is necessary prior to implantation, as it may account for a large part of the improvement by itself.
These findings need to be corroborated in randomized, blinded and controlled trials, as a placebo effect, regression to the mean and spontaneous improvement certainly may play a role in the observed effect. A prospective daily headache diary would certainly be desirable in future studies to avoid recall bias. Some individuals did not have long-term headache improvement after occipital neurostimulator implant, despite improvement in the temporary stimulator trial, as has previously been observed (11). Non-specific effects may have waned after permanent implantation. An important weakness of the study is that it is retrospective with regard to the pain aspects, although this is offset by the long-term follow-up and the careful approach to phenotyping the cases that has been employed. Due to the retrospective nature of the study, some data are missing. Fortunately, limited data are missing in the two main subgroups of patients, so that we are confident this does not affect the main conclusions of the study. Ideally, the questionnaires developed by the Belgian Pain Society would be validated for this kind of work.
Conclusion
Results of ONS for refractory headache are promising, although the concept of intractable headache itself needs to be refined further. The purpose of the definition of refractory must be clear, since the bar to a referral to an expert should be less than for a new therapy that is non-invasive vs. an invasive treatment. A number of issues need to be resolved to optimize ONS, including stimulus parameters, battery life, and the stimulator itself with regard to implantation techniques and associated side-effects, such as lead migration. An externally rechargeable battery would certainly be welcome. Moreover, patient selection criteria, as well as predictors for outcome, need to be further refined, and tested in clinical trials. Our retrospective study and a recent pilot study (23) generate the hypothesis that ICHD-II 13.12 may be an excellent indication for ONS, and a well-powered controlled trial would certainly be welcome. Careful clinical phenotyping will require close collaboration between pain specialists and neurologists, to assign diagnosis according to the ICHD-II. Many patients have been reclassified in this study, and it is clear that multidisciplinary collaboration is essential for the scientific evaluation of ONS. In particular, migraine patients need to be closely monitored for medication overuse, as is appears to be associated with poor long-term outcome in our study. ONS is promising and challenging for all concerned, although the prospect of finding therapies for our most disabled patients is a crucial and rewarding pursuit.