
Abstract
Aim
Despite its frequency in tertiary headache centers, the International Classification of Headache Disorders, 3rd edition (ICHD-3) does not include refractory migraine. Multiple definitions have been proposed with a recent 2020 proposal for both refractory migraine and resistant migraine by the European Headache Federation (EHF). The aim is to reach an international consensus on the definition of refractory migraine.
Methods
This study is a Delphi consensus carried out by a group of international experts in headache medicine. Following a focus group, a panel of 20 experts and one facilitator reviewed the EHF proposed criteria to build upon their definitions. The Delphi consensus was conducted across five rounds. Questions with >70% consensus were deemed to have strong agreement, 60–70% consensus was deemed minor agreement, and <60% deemed no agreement. A final meeting was held to discuss any concerns and specific wording.
Results
The Delphi consensus led to the development of four key categories: refractory migraine, probable refractory migraine, resistant migraine, and treatment-responsive migraine. Similar to the EHF 2020 definitions, refractory migraine requires treatment failure of all evidence-based classes, and resistant migraine requires failure of at least three classes. Probable refractory migraine criteria were designed to account for situations where treatment access barriers may prevent trials of certain medication classes (e.g. pediatrics, low to middle-income countries, lack of insurance coverage). Finally, treatment-responsive migraine criteria were developed to allow for standardization in research studies comparing refractory or resistant migraine to migraine that is treatment-responsive.
Conclusions
These four categories may aid in enrollment for studies on pathophysiology, biomarkers, and new treatment targets. Clinically, the criteria for refractory and resistant migraine will help with clinical decision-making by reinforcing the need to try evidence-based treatments and by providing guidance regarding when to try more aggressive treatment approaches. These criteria may also increase attention to this population's disease burden to help advocate for them as a specific migraine subgroup. Field testing in diverse clinical settings will be needed, but it is recommended that ICHD-3 considers inclusion of these four categories in their appendix.
This is a visual representation of the abstract.
Keywords
Introduction
Migraine is a significant cause of disability worldwide, affecting 1.16 billion individuals (1). It predominantly affects younger populations and is a leading cause of disability among women under 50 years (2). While appropriate treatment can reduce the burden of migraine, not all preventive treatments are effective for everyone. There are individuals who do not experience improvement with most or any preventive treatments and are often seen in specialized headache centers caring for patients with high migraine burden and significant management gaps (3).
Most preventive treatments for migraine were initially developed for other medical conditions. The advent of treatments targeting the calcitonin gene-related peptide (CGRP) pathway marked a shift to migraine-specific prevention (4). CGRP-pathway inhibitors have high efficacy and tolerability, even for many who did not experience improvement from traditional, non-specific treatments (5–7). These medications have revolutionized migraine prevention, prompting a re-evaluation of refractoriness. Before migraine-specific treatments, several definitions of “refractory migraine”, “intractable migraine”, or “refractory chronic migraine” were proposed (8–10). In 2020, the European Headache Federation (EHF) consensus defined two distinct clinical entities: “resistant” and “refractory migraine”. They defined resistant migraine as requiring the failure of at least three preventive medication classes, while refractory migraine requires failure of all classes (11) (Tables 1 and 2).
European headache federation refractory migraine definition 2020 (11).

*Antidepressants (amitriptyline, venlafaxine), antiepileptic (topiramate, valproate), beta blocker (atenolol, metoprolol, propranolol, timolol), calcium channel blocker (flunarizine, cinnarizine), drug acting on the CGRP pathway (monoclonal antibodies, gepants), angiotensin pathway blockers (lisinopril, candesartan), onabotulinumtoxinA (chronic migraine only) and other pharmacologic preventive treatments with established efficacy in migraine (e.g. newly developed drugs).
CGRP = calcitonin gene-related peptide.
European headache federation resistant migraine definition 2020 (11).

*Antidepressants (amitriptyline, venlafaxine), antiepileptic (topiramate, valproate), beta blocker (atenolol, metoprolol, propranolol, timolol), calcium channel blocker (flunarizine, cinnarizine), drug acting on the CGRP pathway (monoclonal antibodies, gepants), angiotensin pathway blockers (lisinopril, candesartan), onabotulinumtoxinA (chronic migraine only) and other pharmacologic preventive treatments with established efficacy in migraine (e.g. newly developed drugs).
CGRP = calcitonin gene-related peptide.
Refractory migraine is common in tertiary care, where 46% of headache clinics report managing individuals in this category (3). It accounts for 5–10% of patients in these clinics (12). The care for these patients incurs high annual costs and healthcare utilization due to ineffective treatment trials (13). Although precise epidemiological data are lacking, its significant presence in headache clinics underscores the urgent need for focused research.
The EHF consensus emphasized distinguishing resistant from refractory migraine. Individuals with resistant migraine might still benefit from highly effective, migraine-specific preventive treatments, while those with refractory migraine likely have a mechanism not modifiable by currently available treatments (14). For the EHF consensus criteria for refractory migraine and resistant migraine, see Tables 1 and 2.
Migraine has clear diagnostic criteria defined by the International Classification of Headache Disorders, 3rd edition (ICHD-3) (15). Chronic migraine is based on headache frequency; resistant and refractory migraine are defined by treatment responsiveness. Inclusion of definitions for medication responsiveness in the ICHD-3 appendix may help identify patients who may benefit most from specialist consultation, aid in selecting patients for advanced therapies, highlight disease burden, and facilitate clinical studies (16).
Given the importance of defining, understanding and managing resistant and refractory migraine, there is a necessity for diagnostic criteria that differentiate these subgroups. The Delphi consensus methodology was chosen due to the lack of biomarkers to guide diagnosis. The present study aims to reach an international expert consensus on diagnostic criteria for refractory migraine and resistant migraine starting from the EHF consensus definition.
Methods
Criteria for the definitions were developed using the Delphi method (17). An initial focus group led to the formation of an international expert consensus group. No study funding was received. This study is not registered.
Focus group
An initial focus group (JR, MKS, FK, ML, MM, HO and LR) was formed by volunteers following discussion on refractory migraine definition at a special interest group meeting during an American Headache Society (AHS) conference in June 2022. Initial plans were discussed via email, followed by an in-person meeting in November 2022. The goal was to review prior criteria, determine the best methodology, and develop a working definition using the EHF criteria as a starting point (11). The EHF definitions for refractory and resistant migraine were provided to the group before starting the Delphi consensus process.
International expert consensus group
An international expert consensus group was formed with 21 panelists and one facilitator (JR). The group included members from multiple continents, academic and private practices, industry, primary care, pediatric headache and low-income countries. Members from AHS, International Headache Society (IHS) and EHF were included. The group also included a physician trained as a pharmacist, a nurse practitioner and a headache psychologist. Panelist members were invited by the facilitator (JR) via email.
Delphi methodology
The Delphi technique was used to reach consensus due to limited literature guiding the development of diagnostic criteria for refractory migraine. Twelve open-ended questions were formulated and pre-tested by the facilitator for survey length before being sent to panelists. Survey Monkey was used for distribution. The pre-test of round 1 took 12 minutes to complete. Invitations were sent via email, no reimbursement was provided for participation, and responses were kept anonymous. Round 1 was sent in December 2023. The facilitator formed anonymized reports summarizing responses and agreement levels after each round. A round was considered complete once more than 50% of panelists responded. There were five rounds, with the final round sent in June 2024. Questions for subsequent rounds were based on results from the prior rounds. Later rounds included agreement of draft diagnostic criteria. The threshold to define consensus varies widely in the literature ranging from 50% to 97% (18–21). The consensus threshold for this study was defined as strong agreement for 70% or greater consensus, minor agreement for 60–70% consensus, and no agreement for less than 60%. Rounds continued until a 60% agreement was achieved, which was deemed realistic given the large group and diverse opinions. Once a consensus was reached, it was used to finalize decisions unless further details or clarification were needed due to conflicts with responses from other questions or additional information requirements. Using the finalized responses, draft criteria were prepared.
Rounds 1–5
Round 1 comprised 13 open-ended questions exploring definitions, goals, barriers to care, handling of new medications, disease duration, headache frequency, disability, preventive versus acute treatment, and medication overuse. Round 2 had 48 questions, including multiple choice, ranking, select any/all, and free text. Round 3 had 13 questions, with four questions scoring the current criteria drafts out of 10. Round 4 had 15 multiple choice and one free text question. Round 5 had eight questions with a pair of questions (Likert scale on criteria and free text response) for each criterion. Thematic analysis of free text responses and level of agreement were used to formulate the summary statement for panelists and develop questions for subsequent rounds. The full list of questions is provided in the supplementary material (Doc. S1).
Final criteria development
After round 5, a group meeting was held to consider criteria wording and manuscript drafting.
Statistical analysis
Thematic analysis with a count of each occurrence was used for free text responses. Multiple choice questions were analyzed using percentages.
Results
Panelists
Twenty-one panelists were invited but only 20 participated. The group included 16 adult headache neurologists, one pediatric headache neurologist, one adult and pediatric headache neurologist, one nurse practitioner, one primary care physician and one pain psychologist. One of the headache neurologists has pharmacy experience and another works in industry. Countries represented were the USA (13), Australia (2), Italy (2), Honduras (1), South Korea (1) and Brazil (1).
Rounds 1–5
Eighteen of the twenty panelists (90.0%) responded to round 1, 15/20 (75.0%) to round 2, 16/20 (80.0%) to round 3, 15/20 panelists (75.0%) to round 4 and 13/20 (65.0%) to round 5. The full results are provided in the supplementary material (Doc. S2).
Final diagnostic criteria
The finalized criteria include four categories: refractory migraine, resistant migraine, probable refractory migraine and treatment-responsive migraine. They have been formatted and outlined in the style of ICHD-3.
Refractory migraine
The definition for refractory is based on an ICHD-3 diagnosis of migraine. Criterion A allows for episodic or chronic migraine, although criterion B does limit diagnosis to those with a high monthly migraine or headache day frequency. Criterion B has three subcriteria of which 2 are required: disability, constant background headache, and/or at least eight monthly migraine days. To standardize for research purposes a comment is added that a patient reported outcome (PRO) such as the Migraine Disability Assessment (MIDAS) with a score of severe to very severe should be used to define disability.
Criterion C requires failure of all medication classes where failure is less than 50% improvement in monthly migraine days, intolerable side effects, or absolute contraindications. Relative contraindications do not count. Eight medication classes were identified: CGRP-pathway inhibitors, onabotulinumtoxinA, antidepressants, beta blockers, angiotensin pathway blockers, calcium channel blockers, anti-seizure medications, NMDA receptor antagonist, and an other category. There is an additional comment that more than four medication class failures must be due to a true lack of response at correct dose and duration otherwise the diagnosis should be coded as probable refractory migraine. At least a CGRP-pathway inhibitor and onabotulinumtoxinA must have a true trial for ineffectiveness; otherwise, the diagnosis should be coded as probable refractory migraine. This criterion also lists all possible medications for each class with the recommended dose range and duration of trial length.
Criterion D is the standard caveat of “Not better accounted for by another ICHD-3 diagnosis”. In refractory migraine, this caveat is important because refractoriness to treatment could be due to an underlying secondary headache that has not been identified or treated. There is an added comment that medication overuse headache can be comorbid to refractory migraine. Resistant migraine can evolve into refractory migraine but cannot be diagnosed simultaneously.
Detailed criteria are provided in Table 3.
Criteria to define refractory migraine

Resistant migraine
While more controversial than refractory migraine, minor consensus was reached to keep resistant migraine as a diagnostic category at round 3. Resistant migraine continued to be considered as a diagnostic category because minor consensus (i.e. at least 60% agreement) was not reached in favor of keeping or removing it in rounds 1 and 2. Keeping both refractory and resistant migraine as distinct diagnostic categories is in alignment with the EHF definition.
Similar to refractory migraine, resistant migraine requires a diagnosis of episodic or chronic migraine for criterion A; two or three of disability, daily headache, or at least eight monthly migraine days for criterion B; and “Not better accounted for by another ICHD-3 diagnosis” for criterion D. The major difference between these two definitions is criterion C, which requires medication failure for at least three medication classes (but not all medication classes). The definition of failure and the medication class list is the same. More than one of the medication classes must be due to a true lack of response. Unlike refractory migraine, a CGRP-pathway inhibitor and onabotulinumtoxinA are not required for diagnosis. Similar to refractory migraine, resistant migraine and medication overuse headache can be coded together. Detailed criteria are provided in Table 4.
Criteria to define resistant migraine

CGRP = calcitonin gene-related peptide; ER = extended release; ICHD = International Classification of Headache Disorders; IV = intravenous; NMDA = N-methyl-
Criteria to define probable refractory migraine
CGRP = calcitonin gene-related peptide; ICHD = International Classification of Headache Disorders.
Criteria to define treatment-responsive migraine

CGRP = calcitonin gene-related peptide; ICHD = International Classification of Headache Disorders; NMDA = N-methyl-
Probable refractory migraine
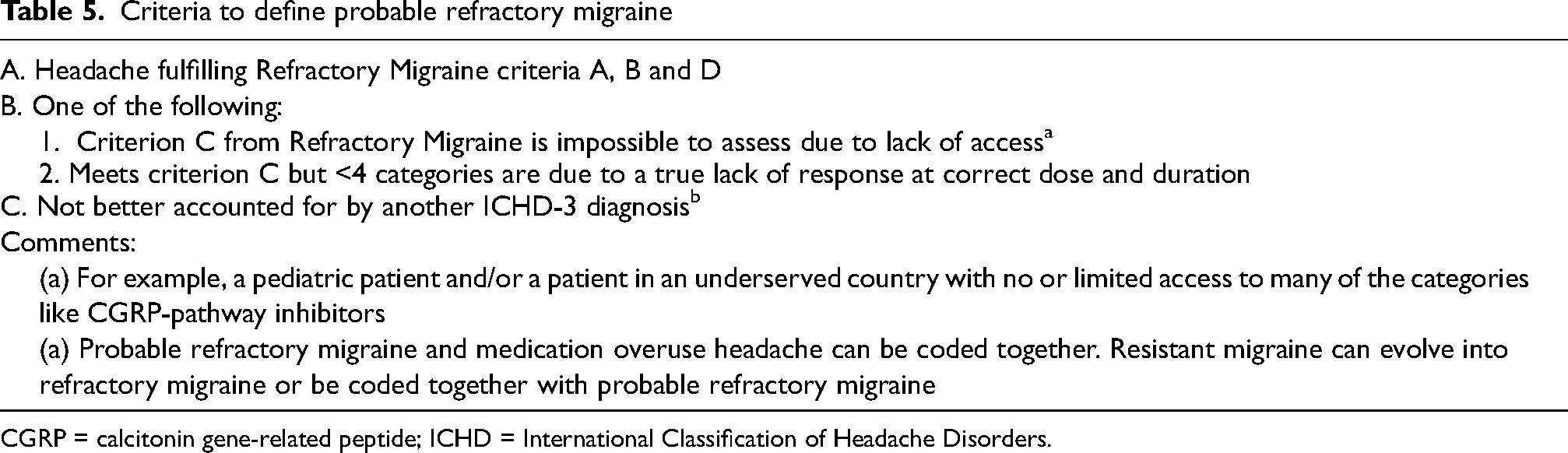
Probable refractory migraine was included as a mechanism to account for limited access to medication classes such as CGRP-pathway medications or onabotulinumtoxinA. It also provides an option for patients with extensive medication intolerances or absolute contraindications. Probable refractory migraine should meet criteria A, B and D from the refractory migraine definition. The main difference is that the refractory migraine criterion C cannot be met either due to inability to access and try all of the listed medication classes or due to four or less medication class failures being due to true lack of response. Criteria C specifies that resistant migraine and probable refractory migraine can be coded together, and that they can both evolve into refractory migraine (Table 5).
Treatment-responsive migraine
Treatment-responsive migraine is not meant for clinical use, but consensus was reached to formalize this definition for use in research as a standardized approach to comparing refractory migraine or resistant migraine experimental groups to a control group of treatment responsive migraine. Treatment-responsive migraine requires a current diagnosis of episodic migraine per criterion A. As a direct opposite to criterion B from refractory and resistant migraine, treatment-responsive migraine must not lead to any of disability, constant headache or at least eight monthly migraine days. A response in criterion C is considered at least a 50% improvement in monthly migraine days sustained for at least three months from a migraine preventive from the same medication class list. However, the final option is worded as “other” allowing for excellent response to a newly emerging treatment or even a non-evidence-based treatment. The criteria further specify that loss of treatment response without a better explanation does allow the diagnosis to be changed to resistant or refractory migraine. This diagnosis cannot be coded with refractory migraine, probable refractory migraine or resistant migraine (Table 6).
Discussion
Historical definitions of refractory migraine
Over time, multiple criteria for refractory migraine have been proposed. Previous criteria have faced limitations and barriers. As new treatments emerge, each set of criteria naming specific medications quickly becomes obsolete. Requiring new therapies such as CGRP-pathway inhibitors limits use of the criteria by certain groups, including pediatrics where these medications are not currently federally approved, or in low to middle-income countries where they may not be available. Opinions on the best definition have varied widely, with medication failure thresholds ranging from two categories to all categories (8–11,23–25). Similar to the 2020 EHF consensus, our group felt it was valid to differentiate those who did not experience improvement from several treatments (resistant migraine) from those who experienced treatment failure from all of them (refractory migraine) (11).
Strengths and challenges of this definition
Addressing global treatment variability
Available pharmacological therapies vary between countries and age groups, which the EHF acknowledged in the comments but not within the criteria themselves (11). The EHF refractory migraine criteria include the calcium channel blockers flunarizine and cinnarizine. These are not available in the United States, and our group decided to include verapamil in this category. European criteria does not include memantine, whereas our group included it per the American Headache Society (AHS) 2021 Consensus statement (26). Our group consensus continued the trend of a specific medication list rather than deferring to regional guidelines. The concept of refractory migraine has not been well-studied in low-income countries that may not have access to treatments such as CGRP-pathway inhibitors. While many in our group felt that access to treatments should be considered, overall, the group felt that biology should drive the criteria. Until studies develop biology-driven criteria, our international consensus supports the EHF's approach of three treatment failures for resistant migraine and all categories for refractory migraine. However, this study includes criteria for probable refractory migraine to account for those with limited access to all categories.
Pediatric populations
The data for preventive treatment of pediatric headache are limited (27). Given that evidence differs for pediatrics, and treatments such as CGRP-pathway inhibitors are not yet approved for this age group, it was debated whether there should be separate pediatric criteria. Ultimately, as was done for low-income countries, the group felt that the use of probable refractory migraine was best. Pediatric treatment access allows for more than three treatment categories, which is sufficient for a diagnosis of resistant migraine where appropriate. This approach allows for resistant or probable refractory migraine in children without compromising the intent of the refractory migraine criteria.
Acute versus prophylactic refractoriness
Many of the previously proposed criteria have included lack of response to acute medications, assuming that refractoriness denotes a poorer response to acute treatment. The EHF criteria do not specifically include acute response, but their expanded explanation indicates that a debilitating headache requires failure of at least two triptans (11). Our group questioned whether a patient can be in a chronic refractory disease state while still maintaining reasonable control over individual migraine attack. Inclusion of acute medication failure would require delineating which medication categories and how to define failure, which would further complicate the criteria. The overall group consensus was that being acutely refractory during an attack may be different from being chronically refractory, though this opinion needs further study.
Use of medication categories over individual medications
Medications are grouped into categories but there may be different mechanism within one category. EHF did note this issue but felt that their drug categories were appropriate (11). Our group felt there was low likelihood of response to a different medication within the same category despite some categories such as anti-seizure medications (topiramate and divalproex/valproate) having diverse mechanisms. Ultimately, the group agreed upon standard categories to reduce criteria complexity. As part of this discussion, the group did not agree to differentiate CGRP-targeting monoclonal antibodies and gepants, or to differentiate erenumab, which targets the CGRP receptor, from the three ligand-targeting antibodies. Against this decision, we commonly see patients experience improvement with a CGRP-targeting monoclonal antibody after being failed by one or two prior CGRP-targeting monoclonal antibodies (28). As research on this topic becomes clearer, medication categories may need to be reconsidered.
Approach to treatment intolerance and contraindications
EHF allowed any ineffective treatment, intolerance, or contraindication to define resistance or refractoriness. An ineffective treatment trial has the expectation of an appropriate duration and dose. Extensive medication intolerances are not allowed in the proposed definitions as intolerance to a medication does not indicate it would not work at an appropriate dose and after an appropriate duration. For contraindications, the group allowed absolute but not relative contraindications as a treatment failure. Early medication trials often use relative contraindications to access newer medications sooner, but as a patient has more treatment failures, their risk-benefit ratio may change, making the prior contraindications less of a barrier. For example, asymptomatic low blood pressure may lead to initial avoidance of an anti-hypertensive medication, but a patient with nearly refractory migraine may be comfortable trying these cautiously. Furthermore, some contraindications may be transient, such a divalproex during pregnancy. To account for these common circumstances, strong consensus was reached that at least five categories must be truly ineffective. In the future, this criterion may need to be re-evaluated.
Medication overuse
The inclusion of medication overuse and medication overuse headache was widely debated. Ultimately, strong consensus was reached to allow both because by the time a patient's disease meets criteria for refractory migraine, there is a greater likelihood of medication overuse. While medication overuse is common, medication overuse headache is likely over-diagnosed (29). While a trial off a potentially offending medication may be reasonable to consider at this stage, many such patients have comorbid pain conditions that also need daily analgesia, limiting feasibility. Furthermore, there is evidence that migraine can improve with preventive treatment in the setting of medication overuse headache (30).
Relationship to headache frequency
The next consideration is whether refractoriness relates to headache frequency. Many proposed criteria have allowed for episodic or chronic migraine. EHF required at least eight monthly migraine days. It is unknown whether a patient with episodic migraine can be refractory to treatment. From thematic analysis of round 1, the group reached early consensus that eight monthly migraine days should be a cut-off and already half of the group felt that refractory migraine should include both chronic migraine and high-frequency episodic migraine. Ultimately, there was strong agreement to include monthly migraine days as a non-mandatory option with chronic daily headache and disability. As the goal of these criteria is to identify non-responders as a distinct subgroup from headache frequency, this relationship will need field testing.
Relationship to headache severity
Whether a persistent low-severity headache denotes refractoriness versus refractoriness being limited to migraine days was controversial. Some members of the panel felt strongly that a chronic daily unremitting headache meant that a patient was still refractory even if the background pain is mild. There was no consensus to require patients have a daily headache. Ultimately, strong consensus was reached to have both chronic daily headache and a threshold for the number of migraine days as non-mandatory options, but field testing will be needed to validate this approach. Pain severity other than including the option of at least eight monthly migraine days in criteria B was not extensively discussed.
Keeping criteria up to date
A recurring issue with all proposed criteria is that as new guidelines emerge, the criteria become obsolete. Our group was faced with how to specify the required treatment trials while ensuring that newly emerging treatments are accounted for. To compensate for this issue, EHF included the category of “other” treatments.1 Consensus was reached to keep this approach, acknowledging criteria need to be dynamic and evolve in the ICHD either as direct criteria additions or as new appendix diagnoses.
Changes in diagnoses over time
The definitions of resistant migraine, refractory migraine, and treatment-responsive migraine might apply to the same patients at different times. By definition, all patients with refractory migraine met criteria for resistant migraine at some point. Conversely, some patients with resistant or refractory migraine may become treatment responders after the successful trial of further preventive treatments. The change in diagnosis over time should be explored with periodic reassessment.
Comorbidities on patients with refractory migraine
Patients with refractory migraine often present with a high burden of comorbid conditions including psychiatric disorders (e.g. depression, anxiety), sleep disturbances, chronic pain syndromes (e.g. fibromyalgia) and cardiovascular risk factors (31). These comorbidities can significantly influence clinical management and pose diagnostic and therapeutic challenges. Whether and how these comorbidities play into diagnosis and treatment need further study.
Inclusion of treatment-responsive migraine
Success criteria to define preventive treatment as effective have been previously discussed (32). Puledda et al. (32) consider treatment to be effective if any of the following are true: ≥50% decrease in monthly migraine days, subjective or PRO-based clinically meaningful improvement, or a clinically meaningful improvement in MIDAS or Headache Impact Test (HIT-6) scores. They also note that in patients with chronic migraine, ≥30% responder rate is sufficient to continue treatment beyond three months. In this Delphi consensus process, round 1 queried the group on their definition of treatment response using free-text response resulting in wide-ranging answers. In round 2, almost three-quarters agreed that a definition for treatment-responsive migraine should be included, and by round 5, almost 85% of the group felt a finalized definition had been achieved. This definition will require field testing and may require further refinement to ensure optimization. At this time, the definition requires a higher standard of response than the standard clinically meaningful improvement used to continue a treatment. The International Headache Society position statement from 2025 is also pushing for more ambitious standards (33). Our proposed criteria state that a patient must have less than eight monthly migraine days, no background headache, and no disability to ensure research study enrollment captures patients with excellent response. This definition is not meant to inform reimbursement policies or when to continue a treatment with a clinically meaningful response.
Research versus clinical usage of the diagnostic criteria
The first ICHD (ICHD-1), published in 1988, constituted a significant achievement in headache medicine, lending much needed credibility to our field (34). Previously, headache diagnosis was inconsistent and based only on expert opinion. ICHD-1 spurred major steps forward in epidemiological, pathophysiological and treatment research, as well as being an invaluable aid for headache diagnosis. It has evolved across multiple editions as the understanding of conditions such as migraine has improved.
Creating criteria for refractory migraine may help address care gaps for this vulnerable population, characterized by individuals whose disease characteristics would have excluded them from clinical trials. These criteria may also support research on epidemiology, pathophysiology, and treatment of patients with refractory migraine. Further research is also needed to clarify medication trial thresholds, therapeutic targets, and what is sufficient to diagnose treatment response. As a starting point for appendix diagnoses, our international consensus reached agreement with EHF on a less stringent threshold of three categories called resistant migraine and a stringent diagnosis called refractory migraine but added criteria to standardize the diagnosis of a treatment responder.
Clinically, these criteria will aid in the identification of patients who do not improve with current evidence-based treatments, and thus consideration should be given to offering treatments that may be more aggressive, expensive, and even experimental. These advanced treatments are often denied by medical insurance or health service payers, but a diagnosis of refractory migraine may be sufficient to allow them for appropriate patients even when outside of their standard migraine guidelines. Furthermore, considering global and age equity in access to treatment, a diagnosis of probable refractory migraine will allow patients without access to all evidence-based treatment to still receive a probable diagnosis that may open the door to more advanced treatment options.
Use of the Delphi method
Developed by the Rand corporation in the 1950s, the Delphi research technique is a qualitative method that uses iterative expert opinion via survey to establish consensus that can then be tested in more quantitative ways (17,19). It allows participants to explore the group's opinions in a non-adversarial manner using anonymous responses. The technique does not require face-to-face contact, which increases study feasibility (35).
The Delphi method does have some weaknesses. A right or wrong answer cannot be expected; rather a testable hypothesis is the best outcome. The technique does not allow for discussion or debate. To account for this issue, we included a virtual final meeting. The process is time consuming, and so participant numbers may dwindle, reducing study validity. Fortunately, we maintained at least a 65% response rate throughout the process. In some cases, consensus was not reached despite multiple rounds, so two tiers of consensus were used: minor (60–70% agreement) and strong (>70% agreement) consensus. Using a consensus threshold of 70–75% would be more rigorous but was not feasible within the diverse opinions of the group and there is no official guideline on the best consensus threshold to use in the Delphi method. Bias may also be introduced by the facilitator who summarizes responses and develops questions. The process can have limited perspectives, but we included an international group and built on the European consensus to help address the over-representation of Americans in this group.
Conclusions
The consensus process has established four key diagnostic categories: refractory migraine, resistant migraine, probable refractory migraine, and treatment-responsive migraine. These criteria are crucial for accurately categorizing patients’ disease based on burden and treatment response, as well as for advancing research on pathophysiology, biomarkers, and future treatment targets for refractory migraine. Clinically, they provide a structured framework for decision-making, reinforce the importance of evidence-based treatments, and help guide the use of more aggressive treatment strategies when necessary. The validation of these criteria in diverse clinical settings is still needed. We recommend that these 4 diagnostic criteria be included in the appendix of the next edition of the International Classification of Headache Disorders to allow field testing and validation.
Article highlights
Based on international consensus, four definitions have been proposed: refractory migraine, probable refractory migraine, resistant migraine and treatment-responsive migraine.
Refractory migraine is defined as migraine with at least two of the following: disability, eight or more monthly migraine days, and/or constant headache with lack of response to all categories of evidence-based preventive treatment.
Resistant migraine is similar to refractory migraine, but has lack of response to three or more categories of preventive treatment
Probable refractory migraine is included to account for patients who lack of access to all categories of preventive treatment or for those with extensive adverse effects and/or contraindications that limit trials for true efficacy.
Treatment-responsive migraine is intended as a standardized research definition for studies that need to compare refractory or resistant migraine to a control group of treatment responders.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251367767 - Supplemental material for Reaching international consensus on the definition of refractory migraine using the Delphi method
Supplemental material, sj-docx-1-cep-10.1177_03331024251367767 for Reaching international consensus on the definition of refractory migraine using the Delphi method by Jennifer Robblee, Fawad A. Khan, Michael J. Marmura, Hope L. O’Brien, Lawrence D. Robbins, Marielle Kabbouche Samaha, Morris Levin, Simona Sacco, Raffaele Ornello, Stephanie J. Nahas, Heike Hesse, Annika Ehrlich, Adam S. Sprouse-Blum, Christina Sun-Edelstein, Bronwyn Jenkins, Elizabeth K. Seng, Shivang Joshi, Meredith J. Barad, Mi Ji Lee, Sheena K. Aurora and Mario Fernando Prieto Peres in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024251367767 - Supplemental material for Reaching international consensus on the definition of refractory migraine using the Delphi method
Supplemental material, sj-docx-2-cep-10.1177_03331024251367767 for Reaching international consensus on the definition of refractory migraine using the Delphi method by Jennifer Robblee, Fawad A. Khan, Michael J. Marmura, Hope L. O’Brien, Lawrence D. Robbins, Marielle Kabbouche Samaha, Morris Levin, Simona Sacco, Raffaele Ornello, Stephanie J. Nahas, Heike Hesse, Annika Ehrlich, Adam S. Sprouse-Blum, Christina Sun-Edelstein, Bronwyn Jenkins, Elizabeth K. Seng, Shivang Joshi, Meredith J. Barad, Mi Ji Lee, Sheena K. Aurora and Mario Fernando Prieto Peres in Cephalalgia
Footnotes
Author contributions
Dr Jennifer Robblee participated in conceptualization, data curation, formal analysis, investigation, methodology, project administration, validation, visualization, writing (original draft) and writing (review & editing). Dr Fawad Khan participated in conceptualization, investigation, methodology, writing (review & editing). Dr Michael Marmura participated in conceptualization, investigation, methodology, writing (review & editing). Dr Hope O’Brien participated in conceptualization, investigation, methodology, writing (review & editing). Dr Lawrence Robbins participated in conceptualization, investigation, methodology, writing (review & editing). Dr Marielle Kabbouche Samaha participated in conceptualization, investigation, methodology, writing (review & editing). Dr Morris Levin MD participated in conceptualization, investigation, methodology, validation, writing (original draft), writing (review & editing). Dr Simona Sacco participated in investigation, methodology, writing (review & editing). Dr Raffaele Ornello participated in investigation, methodology, writing (original draft), writing (review & editing). Dr Stephanie Nahas participated in investigation, writing (review & editing). Dr Heike Hesse participated in investigation, writing (review & editing). Dr Annika Ehrlich participated in investigation, validation, writing (review & editing). Dr Adam Sprouse-Blum participated in investigation, validation, writing (review & editing). Dr Christina Sun-Edelstein participated in investigation, validation, writing (review & editing). Dr Bronwyn Jenkins participated in investigation, validation, writing (review & editing). Dr Elizabeth Seng participated in investigation, writing (review & editing). Dr Shivang Joshi participated in investigation, writing (review & editing). Dr Meredith Barad participated in investigation, writing (review & editing). Dr Mi Lee participated in investigation, validation, writing (review & editing). Dr Sheena Aurora participated in investigation, writing (review & editing). Dr Mario Peres participated in investigation, writing (review & editing)
Declaration of conflicting interests
Dr Jennifer Robblee discloses grant support from Barrow Neurological foundation, investigator support from Eli Lilly and Abbvie, as well as paid Editorial relationship with MedLink Neurology and Neurodiem. Dr. Robblee has received personal compensation for serving on advisory boards for Tonix and Allergan/Abbvie. Dr Robblee also discloses that a family member has partial ownership of Scottsdale Providence Recovery Center.
Dr Fawad Khan discloses receiving institutional research support from Marinus, Biohaven, Teva, Lundbeck and UCB; advisory fees from Eisai, Neurelis, Marinus, Epitel, Pfizer; honorarium for speaker engagements from Amgen, UCB, SK Life Science, Lundbeck, Allergan, Lilly USA, Impel Pharmaceuticals, AbbVie; honorarium for educational programs from Natus and Stratus. He serves on the Louisiana State Medical Advisory Board in a non-paid position. In non-compensated roles, and he is a board member of the Deccan Alumni Association of North America, a non-profit professional society.
Dr Michael Marmura discloses receiving institutional research support from AbbVie and Teva, and advisory fees from Lundbeck, Theranica,
Dr Hope O’Brien discloses participating in a speaker bureau for AbbVie, Eli Lilly, Pfizer, Biohaven (past), BDSI (past) and Scimed; participating on an advisory board for AbbVie, Eli Lilly, Pfizer, Biohaven (past), BDSI (past); participating as a consultant for Medscape and Guidepoint; Editorial Royalties for UpToDate, Research Funding from AbbVie, Eli Lilly and Vector Psychometric Group. She also reports being the American Academy of Neurology Vice-chair MMC and an Invited Speaker; American Headache Society committee member, past chair for Underrepresented committee and an invited Speaker; United Council of Neurological Subspecialties accreditation committee member; National Headache Foundation Board member; UC Master of Health Administration Program Advisory board member; Cincinnati Eye Institute Foundation Board member; and Medscape Migraine Center of Excellence Faculty consultant.
Dr Lawrence Robbins discloses being a speaker for Abbvie, Impel and Idorsia
Dr Marielle Kabbouche Samaha discloses investigator support to the institution for research studies from Eli Lilly, Abbvie, Teva, NIH and PICORI direct pay to her institution. Dr Kabbouche has received direct pay as a speaker from Theranica in the last two years and as a consultant for Merz pharmaceutical.
Dr Morris Levin discloses an advisor role in one-day advisory board meetings with AbbVie, Biohaven, Theranica, BDSI and Linpharma; he serves as a consultant for Percept and Neurolytics. He is a member of no speakers’ boards and has no stock shares or options in any biomedical company.
Dr Simona Sacco discloses personal fees as speaker or advisor for Abbott, Allergan-Abbvie, AstraZeneca, Bayer, Boheringer, Eli Lilly, Lundbeck, Pfizer and Teva. Other roles include President for the European Stroke Organisation, editor-in-chief for Cephalalgia and Cephalalgia Reports, and assistant editor for Stroke.
Dr Raffaele Ornello discloses personal fees for presentations or Advisory Boards from AbbVie, Eli Lilly, Lundbeck, Novartis, Organon, Pfizer and Teva. He is an Editorial Board Member for The Journal of Headache and Pain and Associate Editor for Frontiers in Neurology.
Dr Stephanie Nahas discloses receiving honoraria for consulting from AbbVie, Amneal (ended June 2024), Axsome (ended May 2024), Eli Lilly (ended November 2024), Lundbeck (ended October 2023), Pfizer and Tonix (ended November 2023). She has received honoraria for work in education or publishing from American Academy of Neurology, American Headache Society, Diamond Headache Clinic Research and Educational Foundation, MedLink Neurology, Springer, WebMD/Medscape and Wolters-Kluwer.
Dr Heike Hesse reports no disclosures.
Dr Annnika Ehrlich discloses serving as a consultant, on an advisory board and on a speaker bureau for Abbvie. She has consulted for Pfizer, and served on advisory boards for eNeura, Lundbeck and Theranica. She is the advance practice provider representative to the American Headache Society board. She received an honorarium for serving on the Headache Cooperative of the Pacific board. She serves as President of the Alliance for Headache Disorders Advocacy and The Headache Alliance.
Dr Adam Sprouse-Blum discloses serving as a consultant for Guidepoint.
Dr Christina Sun-Edelstein discloses honoraria for speaking and consulting/advisory board participation from Teva, Lundbeck, Lilly and Pfizer. She also receives royalties from UpToDate.
Dr Bronwyn Jenkins discloses educational honoraria and advisory fees from Abbvie/Allergan, Eli Lilly, Teva, Lundbeck and Pfizer; with travel grants from Care Pharmacy and Pfizer. Other roles include being Immediate Past President of the Australian and New Zealand Headache Society (ANZHS) and on the subcommittees of ethics and education for IHS.
Dr Elizabeth Seng discloses serving as a consultant or on an advisory board for GlaxoSmithKline, Click Therapeutics, Theranica and Abbvie, and received research funding from the NINDS (NS096107 Principal Investigator [PI]: Seng), National Center for Complementary and Integrative Health (R01AT011005-01A1 Multiple PIs: Seng and Shallcross), the Veteran's Health Administration (the Headache Center of Excellence Research and Evaluation Center and VA HSR&D, IRP 20-002 PI: Damush) and the American Heart Association.
Dr Shivang Joshi discloses honoraria for speaking from Abbvie, Scilex and Lundbeck. He has been an advisor for Abbvie, Lundbeck, Lilly, Axsome and Sermo.
Dr Meredith Barad discloses consultant work for Abbvie–Migraine and Eli Lilly.
Dr Mi Lee discloses personal fees as speaker or advisor from Abbvie, Eli Lilly, Lundbeck, Pfizer, Teva, Organon, CKD, SK Chemical, YuYu and NuEyne; research supports from Abbvie, Pfizer, Eli Lilly, Pfizer, Lundbeck, Novartis, Teva, Otsuka, BioHaven, Ildong, Yuhan, NuEyne, Teva and YuYu; research grants from National Research Foundation of Korea(NRF), Medical Device Development Fund grant funded by the Korea government, Korean Headache Society and Seoul National University. She is an associate editor for Cephalalgia and Headache and Pain Reports.
Dr Sheena Aurora discloses being the VP for C2N diagnostics.
Dr Mario Peres discloses personal fees from Ache, Allergan/AbbVie, Eli Lilly, Eurofarma, Libbs, Lundbeck, Novartis, Pfizer, Sanofi and Teva, and has received research support from Allergan/AbbVie, Eli Lilly, Eurofarma, Janssen-Cilag, Libbs, Natura, Novartis and Teva.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.