
Abstract
Our aim was to determine the prevalence of right-to-left shunt (RtLS) in patients with chronic migraine (CM), and to correlate the presence and grade of RtLS with aura and neurological symptoms, and duration and severity of disease. The prevalence of RtLS in migraine without aura is similar to that of the general population (between 20 and 35%). In migraine with aura, the prevalence is much higher (approximately 50%). The prevalence in CM, with or without aura, is unknown. Consecutive patients between the ages of 18 and 60 years with CM attending a tertiary care specialty headache clinic over an 8-week period were eligible. There were 131 patients in the study. A structured diagnostic interview was performed. Bubble transcranial Doppler with Valsalva manoeuvre determined RtLS presence and grade. Sixty-six percent (86/131) of patients had RtLS, a statistically significantly greater rate than those reported in the general population and in migraine with or without aura (P < 0.001). There was no difference in RtLS rate or grade between those with and those without aura. Specific headache features and the presence of neurological symptoms were similar between those with and those without RtLS. Compared with both the general population and the episodic migraine population (with and without aura), patients with CM, with or without aura, are more likely to have RtLS. The clinical implications of our findings need to be determined.
Keywords
Introduction
Chronic migraine (CM), as defined in the International Classification of Headache Disorders, 2nd edn (ICHD-II) (1), is a disorder of ≥ 3 months' duration characterized by headaches occurring ≥15 days/month with ≥ 8 days/month of headache meeting criteria for migraine without aura (MoA) or responding to migraine-specific medication. It affects 2–3% of the population and often is disabling and refractory to a wide variety of medical and non-pharmacological treatments (2,3).
Right-to-left shunt (RtLS) is about twice as common in migraine with aura (MA) compared with both MoA and the general population (approximately 50% vs. approximately 25%) (4–7). Whether this association is coincidental, representative of shared genetics, or causal has not been determined. Causality may be implied if correction of RtLS leads to improvement in migraine. Although observational evidence supports this notion (8–17), a double-blind, placebo-controlled trial failed to show efficacy for closure of patent foramen ovale with RtLS (18). In addition, if a causal link is present, the burden of migraine disease may be greater in those with RtLS. A barrage of microemboli passing through a RtLS into the cerebral circulation could lead to a greater number/intensity of migraine attacks (19). This has not been apparent thus far, but an important subset of the population of migraineurs has not been examined: those with CM. We therefore determined the headache characteristics and prevalence of RtLS in patients with CM.
Methods
Participants
Patients attending a specialty care headache clinic at a university hospital between June and August of 2008, with a diagnosis (made by a specialist at the centre) of CM in the electronic medical record, were eligible. Upon screening or interview, patients were excluded if the diagnosis was inaccurate, if medication overuse was deemed the sole cause of daily headache, if transcranial Doppler (TCD) or transoesophageal echocardiogram (TEE) had been done previously to detect the presence of RtLS, or if they were pregnant. All participants provided written informed consent and were counselled regarding the potential implications of the presence of RtLS prior to enrolment. This study was approved by our Institutional Review Board.
Instruments and definitions
Visual aura rating scale items
A score of ≥ 5 is 91% sensitive and 96% specific for visual aura as defined by International Classification of Headache Disorders, 2nd edition criteria in patients with episodic migraine.
Transcranial Doppler
Patients were fitted with a headframe system connected to the TCD machine (Terumo PMD150 Digital Transcranial Doppler system, Marc1500 Transcranial Doppler Probe Fixation Headframe; Terumo Cardiovascular Systems Corporation and Spencer Technologies, Seattle, WA, USA), and both middle cerebral arteries were insonated. An intravenous catheter (IV) (20 or 22 G) was inserted into the median cubital vein (preferred) or any other accessible vein in the arm or hand, flushed with saline, and clamped.
Contrast was prepared with 8 cm3 saline, 1 cm3 air, and 1 cm3 of the participant's blood for bubble stabilization (22). Once agitated between two syringes via a three-way stopcock (18 exchanges), the contents were injected into the participant's vein over 8 s. Once 5 cm3 of contrast was injected, the patient performed a metered Valsalva manoeuvre, maintaining a pressure at or slightly above 40 mmHg for 10 s, as the remainder of the bolus was injected. Participants were in a seated position during the procedure.
The TCD machine recorded blood flow in the middle cerebral arteries prior to the initial injection until at least 30 s after the final embolic track was recorded, or for 3 min post Valsalva if no embolic tracks were seen. Shunts were graded according to the Spencer Logarithmic Scale:
Grade 1: 1–10 embolic tracks Grade 2: 11–30 embolic tracks Grade 3: 31–100 embolic tracks Grade 4: 101–300 embolic tracks Grade 5: > 300 embolic tracks.
Participants were monitored for adverse events (AEs) for 15 min if no RtLS was detected, or for 30 min if RtLS was detected.
Statistical considerations
This sample of 131 yielded sufficient power (80%) for an estimated effect of 0.30 and α of 0.05. Univariate analyses were conducted first comparing the groups with and without RtLS. Based on these results, and considering potential clinical predictors related to theories of the pathophysiology of migraine and RtLS, exploratory multivariate analyses were conducted subsequently. A forward likelihood-ratio logistic regression was conducted on RtLS status (present or not) with the presence of five clinical predictors: throbbing quality of baseline daily headache, vomiting with baseline daily headache, blurry vision, language dysfunction (difficulty with word-finding, speech production, or comprehension), and allodynia. Forward likelihood-ratio logistic regression analysis is a data-driven method considered useful for exploratory purposes. This method determines automatically which variables to add or drop from the model. To evaluate any relationships between RtLS and aura, allodynia, severity of migraine, and current migraine frequency (fewer than, or greater than or equal to 15 days/month), a series of four contingency table analyses were conducted. To ascertain whether the presence of RtLS may influence the emergence, persistence or progression of migraine, five independent samples t-tests were conducted to detect differences between patients with and without RtLS on the following dependent temporal variables: (i) age of onset of episodic headache; (ii) age of onset of daily headache; (iii) time to transformation to daily headache [defined as (ii) minus (i); and (iv) duration of total headache illness [current age minus (i)], and duration of daily headache illness [current age, or age when migraine was last ≥ 15 days/month, minus (ii)]. These tests were conducted at α of 0.01 (0.05/5) based on the Bonferroni rationale to maintain the α level of 0.05.
Results
Participants consisted of 131 patients (115 women and 16 men, age 18–60 years; mean = 42.71, S.D. = 11.23; 94% White) who had at any time been diagnosed with CM (or transformed migraine). Thirty-five of the 131 patients (27%) were, at the time of the study, experiencing migraine < 15 days/month, while the rest (n = 96, 73%) continued to experience headache on ≥ 15 days/month (P < 0.001 based on a two-tailed z approximation test). Fifty-three of the patients (41%) had aura.
Sixty-six percent of patients (86/131) had RtLS. This is statistically significantly greater than an estimated general population proportion of 25% (P < 0.001 based on a two-tailed z approximation test), and an estimated episodic MA population of 50% (P < 0.001 based on a two-tailed z approximation test). The prevalence was similar among those with and without ICHD-II aura (64% in those with aura vs. 67% in those without). RtLS presence and size failed to correlate with any aura symptom, VARS score, and each individual VARS item.
Of the 86 shunts identified, 36.0% were Grade I, 20.9% were Grade II, 17.4% were Grade III, 7.0% were Grade IV, and 18.6% were Grade V. Grades did not differ significantly among those with or without aura (Fig. 1). Grade did not correlate with age of onset of disease, duration of disease, cardinal features of migraine, associated neurological symptoms, allodynia, or current headache frequency (data not shown).
Presence of aura for each right-to-left shunt (RtLS) grade. Shunt grades are similar for those with and without aura. Percent represents the proportion of cases in each grade with or without aura.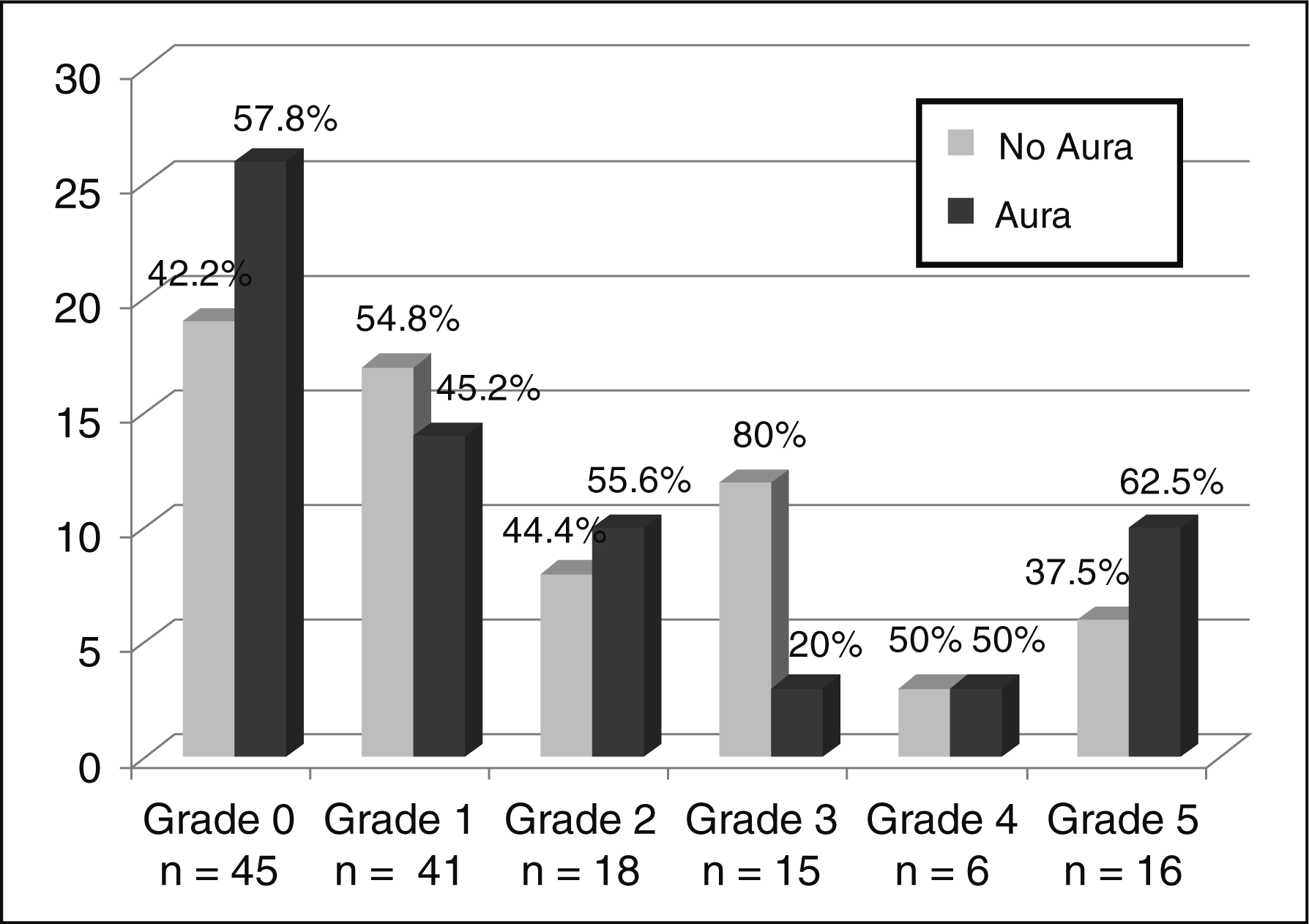
Table 2 depicts the clinical features of the headache disorder among those with and without shunts. Two statistically significant differences were seen with language dysfunction and vomiting with baseline headache. These two variables, along with three other clinical features (throbbing, blurry vision, and allodynia) were included in the forward likelihood-ratio logistic regression. These other variables were chosen because of their strong clinical association with migraine. Results of the forward likelihood-ratio logistic regression indicated that the two-predictor model provides a statistically significant improvement over the constant-only model, χ
2 (2, N = 131) = 9.79, P = 0.007. Those with RtLS were 2.28 [95% confidence interval (CI) 1.06, 4.84] times more likely to have language dysfunction and 3.86 (95% CI 1.05, 14.17) times more likely to have vomiting with baseline daily headache (Fig. 2). The Nagelkerke pseudo R
2 indicated that the model accounted for 10.0% of the total variance. Additionally, the Hosmer and Lemeshow test suggested an acceptable model fit (discrimination between the groups) based on the two predictors, χ
2 (2, N = 131) = 1.178, P = 0.56. A finding of non-significance, as in this report, indicates that the model adequately fits the data. This Hosmer and Lemeshow test is preferred over classification tables when assessing model fit. However, the accuracy of the overall model was 66.4% with a sensitivity of 73.3% and specificity of 53.5%.
Right-to-left shunt (RtLS), language dysfunction, and vomiting with baseline daily headache. Those with RtLS are more likely to experience language dysfunction and vomiting with baseline daily headache. RtLS and clinical features of the headache disorder Right-to-left shunt (RtLS) is not strongly associated with any clinical feature of migraine.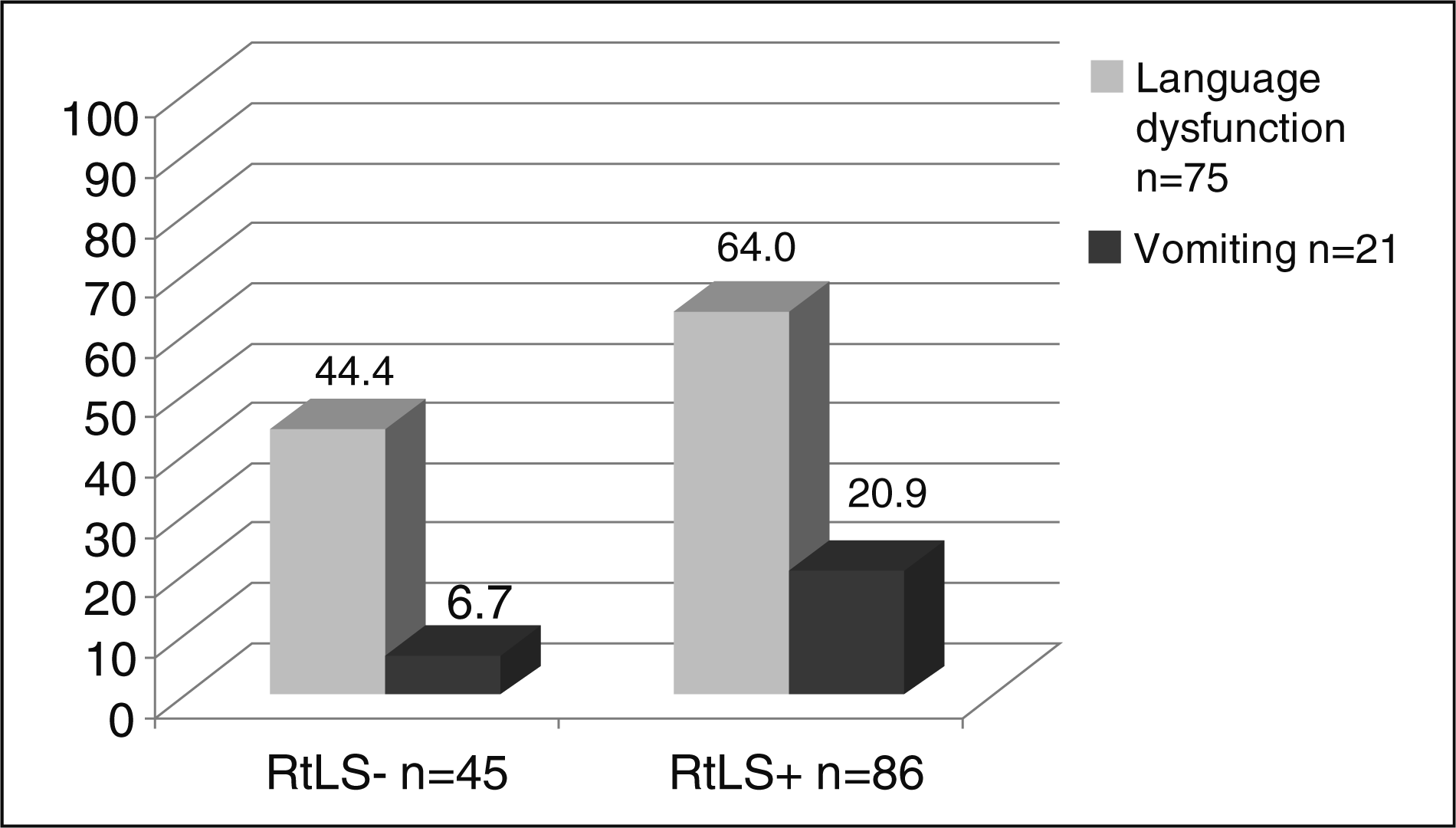

Results of the contingency table analyses indicated that only current migraine frequency achieved a significant effect, χ
2 = (1, N = 131) = 4.36, P = 0.037, Cramer's V = 0.18. Of the 35 patients currently with < 15 headache days/month, 28 (80%) had RtLS (Fig. 3). Aura was no more common in those with RtLS in this subset, nor was there a difference in aura in the two headache frequency groups.
Status of current headache frequency and presence of right-to-left shunt (RtLS). RtLS was detected more often in those experiencing migraine < 15 days/month at the time of study.
RtLS and temporal features of the headache disorder

Right-to-left shunt (RtLS) is not associated with earlier onset of disease, faster rate of progression from episodic to chronic form, or total disorder duration.
Of 131 patients tested, 109 had an accessible vein in the arm. RtLS was detected in 77 of those 109 (70.6%), and in nine of the remaining 22 tested by hand IV (40.9%). In other words, of the 86 patients with RtLS, 77 (89.5%) were detected by arm IV, whereas only nine (10.5%) were detected by hand IV. A χ2 test indicated a significant effect, χ 2 = (1, N = 131) = 7.17, P = 0.007, Cramer's V = 0.23.
Few AEs occurred. One patient complained of pain from IV insertion, six patients developed a headache after the procedure, six patients became lightheaded upon venepuncture or blood draw, and six patients became lightheaded during or after the procedure (one of these also developed headache). Despite counselling before and after the procedure, several patients found to have RtLS brought concerns regarding this to their headache physician, primary physician, or a cardiologist.
Discussion
We found that RtLS was present in 66% of CM patients, which is statistically significantly greater than an estimated general population proportion of 25% and an estimated episodic MA population of 50%. In contrast to prior studies, we found no association between the presence of aura and RtLS.
RtLS detection rates by TTE, TEE, or TCD in various populations

Right-to-left shunt (RtLS) rate is higher in patients with migraine with aura and in stroke patients. Transthoracic echocardiography (TTE) is less sensitive than transoesophageal echocardiography (TEE) and transcranial Doppler (TCD).
MA, migraine with aura; MoA, migraine without aura.
The mechanism of association between migraine and RtLS is still uncertain. Persistence of RtLS and migraine susceptibility may be determined by the same or linked underlying gene(s). RtLS may contribute to migraine by allowing waste products, metabolites, or other substances that may trigger migraine headache (such as serotonin or microemboli) to pass into cerebral arterial circulation instead of being filtered out or metabolized in the lungs (19).
Are there certain defining characteristics of those migraineurs with RtLS or the features of the headaches from which they suffer? In our study, age of onset of episodic and daily headache, and the time to chronification from episodic to daily headache, did not differ between those with and those without RtLS. Aura was no more common in those with RtLS compared with those without. This is true when defining aura according to ICHD-II criteria, when applying VARS score, for each individual item in the VARS, and even for aura-like symptoms that may not conform strictly to ICHD-II criteria. One neurological symptom, language dysfunction, and one cardinal feature of migraine, vomiting with daily headache, weakly correlated with the presence of RtLS. Given that a plausible pathophysiological link is lacking, this could be due to chance. These findings are similar to those reported by Anzola et al. in episodic migraineurs with aura. Those with RtLS were slightly younger, more often had family members with migraine, and had a slightly higher frequency of somatosensory symptoms of aura (51% vs. 41%) (35). In our study, shunt size also had no relation to any of the above. Indeed, CM with and without RtLS seem nearly indistinguishable, except that RtLS was statistically significantly associated with a current headache frequency of < 15 days/month. Perhaps the presence of RtLS provides an organic substrate more responsive to treatment, or is a marker for a subset of the disorder that is somehow more readily amenable to currently available treatments.
There were limitations to our study. We did not include a control group, instead relying on established RtLS prevalences (4–7). Our subject pool consisted predominantly of White women, which is different from the demographic make-up of chronic migraineurs reported in epidemiological studies (50–60% White, 50–75% female), decreasing generalizability to a non-clinical, non-headache-centre population at large. It would have been interesting to evaluate pure medication overuse headache patients; however, time and resources did not allow for an expanded study of this type. Depending on the accessibility of participants' veins, the IV location varied. When the IV was placed in the hand, there was a significantly lower detection rate compared with when the IV was placed in antebrachial or antecubital veins. Considering that most RtLS TCD studies utilize antecubital IVs, our study may underestimate the rate of RtLS in the CM population.
In conclusion, RtLS is common in CM. The only characteristics statistically associated with RtLS in patients with CM were headache frequency of < 15 days/month at the time of study and having symptoms of vomiting and language dysfunction with baseline headache. In contrast to the episodic migraine population, aura is not associated with RtLS in CM, suggesting differing mechanisms for these associations. Although RtLS may be present quite frequently in those with CM, these data do not support the hypothesis that it plays a pathogenic role. Further studies are needed to verify these findings and elucidate possible mechanisms of association.