
Abstract
A survey of 148 family doctors attending a continuing medical education migraine update lecture was performed to assess whether family doctors like to treat migraine and other common disorders and the prevalence of migraine. Doctors were asked to respond to the following statement using a five-point Likert scale (from 1, strongly disagree to 5, strongly agree): ‘I like to treat patients with this disease or symptom’. The response rate was 53% with a mean age of 51.5 years. Doctors reported liking to treat general medical conditions more (mean = 4.40) than migraine (mean = 3.38) and other neurological diseases (mean = 3.20). Doctors reported a personal history of migraine in the prior 1 year of 22.8% and 45.6% lifetime, with 17% becoming aware for the first time that they personally had migraine after attending the lecture. Respondents with a personal history of migraine liked to treat migraine more than those without a history.
Introduction
Anecdotally, family doctors do not like to treat patients with migraines, dizziness, and low back pain. However, since little is formally known about whether family doctors like to treat these and other diseases and symptoms commonly encountered in practice, we performed a survey. An additional observation is that family doctors often diagnose themselves with migraine after attending a review lecture on migraine including diagnosis. The survey was also performed to provide more information on this observation, the prevalence of migraine in family doctors, and whether those with a personal history of migraine like to treat patients with migraine more than those without.
Primary care doctors provide most of the care for migraineurs, treating about two-thirds (1) and performing > 70% of the estimated 5 million office visits per year for migraine in the USA (2). Migraineur satisfaction with their care by family doctors has been reported as varying between 21% (3) and 74% (4). Could doctor dislike of or indifference to migraine, if present, be a factor in reducing patient satisfaction and resulting in patients not asking or returning for further treatment (5)?
Methods
One hundred and forty-eight family doctors attended a 1-h continuing medical education lecture, ‘Migraine update’ (reviewing epidemiology, pathophysiology, International Classification Headache Disorders, 2nd edition (ICHD-II) criteria, clinical manifestations, and treatment) at the ‘58th Annual Session and Scientific Assembly of the Texas Academy of Family Physicians’ in Corpus Christi, Texas on 28 July 2007 given by one of the authors (R.W.E.). Survey instruments (provided with registration materials) were submitted after the lecture.
The survey instrument asked 15 questions about the following topics in this order (the number of questions for each topic is included parenthetically): the likeability of various diseases (n = 10); doctors' personal history of migraine, if any, using ICHD-II criteria (n = 2); and demographics (n = 3). Doctors were asked to respond to the following statement for each of 10 diseases using a five-point Likert scale (1, strongly disagree; 2, disagree; 3, neutral/no opinion; 4, agree; and 5, strongly agree): ‘I like to treat patients with this disease or symptom’. Analysis of variance (
Results
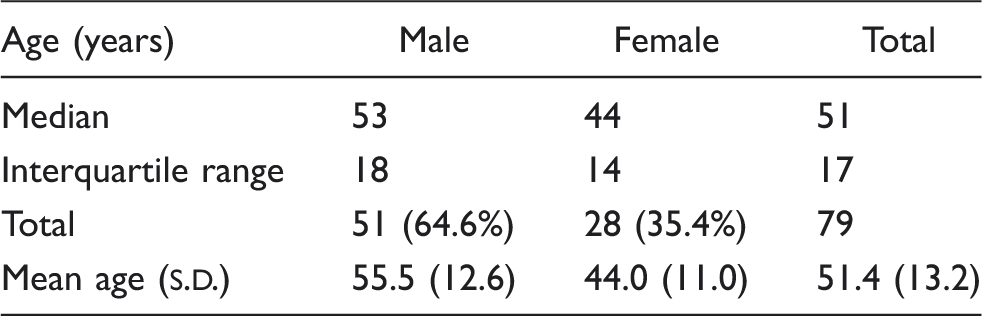
Age/sex distribution of respondents
Responses to statement, ‘I like to treat this disease or symptom’ (n = 79)

1–5 Likert scale (1 strongly disagree, 3 neutral/no opinion, 5 strongly agree).
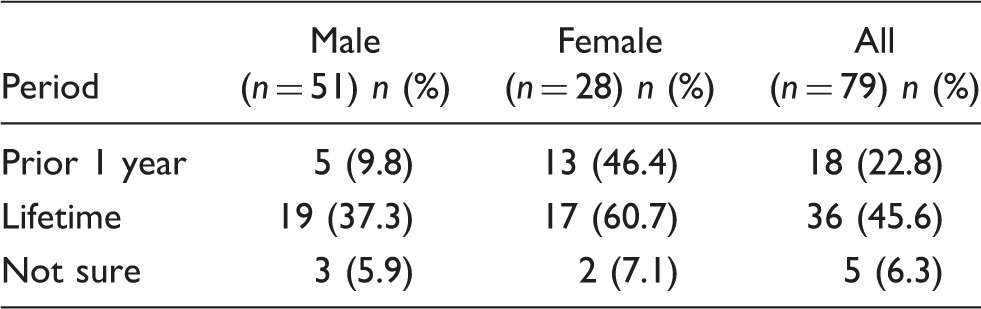
Prior 1 year and lifetime prevalence of ICHD-II migraine among survey respondents
Thirteen respondents became aware for the first time after listening to the migraine lecture that they personally had migraine (17.3% of the 75 respondents who answered this question). Of those made aware, there was an equivalent number of women and men (18.5% vs. 16.7%). There was no correlation between years in practice (greater or lesser) and this first diagnosis of migraine, r(73) = −0.074, P = 0.528. Doctors who became aware that they had experienced a migraine after listening to the lecture, on average, had no opinion about treating patients with migraine (mean = 3.23,
Discussion
The response rate for the survey was 53%, which is comparable to other doctor surveys (6). Previous studies have assessed primary care doctors' attitudes and beliefs about many of the disorders considered in this study (7–10), including migraine (11), but we are not aware that any have specifically considered whether family doctors like to treat the disorders.
As suggested by the anecdotal observation, the likeability of migraine was similar to dizziness and low back pain in the range of neutral/no opinion, similar to the two other neurological disorders, painful diabetic peripheral neuropathy and transient ischaemic attack. Fibromyalgia was considered distinctly less likeable to treat. The common medical conditions were all likeable.
There may be several explanations why the family doctors in our sample responded that they like to treat general medical conditions more than migraine and other neurological disorders and fibromyalgia. Medical students variably have neurology rotations (12) and family doctors may have little training in neurology with a 1-month half-time rotation during residency. Many non-neurologists including primary care doctors may be intimidated or uninterested in neurology during medical school, residency, and in practice (‘neurophobia’) (13–15).
Pain disorders may be considered subjective, time consuming, and difficult to treat, with fibromyalgia considered an extreme example where there is controversy over its legitimacy among some doctors. (In a French survey, fibromyalgia was considered as a disease by only 23% of rheumatologists and 33% of general practitioners (GPs) (16).) Alternatively, there might be cultural differences between doctors. In a survey of Spanish GPs, 69.8% reported very great or great interest in migraine. However, in another survey of Spanish GPs, there was less confidence handling neurological patients than patients with other common medical conditions that may produce responses as in this survey (17).
A greater prevalence of migraine in the previous 1 year and lifetime in men and women was reported compared with most general population studies, which find the following 1-year and lifetime prevalences in men and women, respectively: men, 6% and 8.4% (plus an additional 11.7% with probable migraine); women, 18% and 18.4% (plus 16% probable migraine) (18,19). Four other surveys have found an increased prevalence of migraine in GPs. In an English survey of 882 GPs, 13% of the men and 25% of the women reported having migraine in the previous year (20). The 1-year and lifetime prevalence of migraine, respectively, was 35% and 47% in a survey of 63 Canadian family doctors (21). A survey of 721 GPs in Spain reported a lifetime prevalence of 27.4% (19.3% in men and 37.1% in women) (22). A survey of 130 GPs in Germany found a lifetime prevalence of 24.6% (23). Surveys of neurologists in the USA and other countries have found even greater prevalences of migraine than the GPs (23). It is not certain why these doctor groups may have a greater prevalence of migraine than the general population.
It is possible that those with migraine might have preferentially responded to the survey. However, the first 10 items did not ask about their personal history of migraine. Interestingly, 17.3% of respondents became aware for the first time that they had migraine after they listened to the lecture and 5% were still not sure. This could be due to a lack of self-reflection about their own symptoms or lack of knowledge of migraine diagnostic criteria.
In this survey, doctor migraineurs reported that they liked to treat patients with migraine more than doctors without a personal history of migraine. Although not assessed, this likeability may result in greater patient satisfaction. In a French study of 711 GPs (325 with migraine, 227 without migraine but with a close family member with migraine, and 159 with neither), migraineurs' self-reported quality of life and feeling about medical support were highest when their doctors also had migraine and lowest amongst patients treated by doctors with no close family members suffering from migraines (24).
However, a doctor's personal experience with other diseases may not necessarily improve patient care or satisfaction. GPs' personal history of low back pain may influence patient management in not following guidelines (25). One study found that doctors with a personal or close diabetes experience did not have a more positive attitude towards diabetes than doctors without such experience (26).
Primary care doctors may not manage migraine (6) and other common neurological problems as well as they might. Primary care doctors in the USA and around the world misdiagnose migraine headaches as sinus or tension headaches in ≥ 25% of patients (27). Family doctors (who see nearly 45% of all dizzy out-patients (28)) may not routinely screen dizzy patients for vestibular impairment based on available recommended practices (29) or follow evidence-based guidelines for treatment of low back pain (30), which accounts for one out of 17 office visits. However, this survey does not address the importance of whether a doctor likes to treat a certain disease or not, which can include a doctor's depth and currency of knowledge and skills, time spent with a patient, empathy, and treatment. Future studies correlating likeability of diseases by doctors with patient satisfaction and management would be of interest. Until then, many patients might choose to see a doctor who likes to treat patients with their disease.