
Abstract
Whether the prevalence of migraine is increasing is controversial. We conducted annual surveys in 1999-2001 to investigate migraine prevalence among a nationwide sample of 13 426 adolescents aged 13-15 years. Participants from five junior high schools around different regions of Taiwan completed self-administered questionnaires. The diagnosis of migraine was based on the classification criteria proposed by the International Headache Society, 1988. Data for 23 433 person-years were collected and analysed for trends in prevalence and incidence. The 1-year prevalence of migraine increased 42% during 1999-2001 (from 5.2 to 7.4%, P < 0.001). This increasing trend was demonstrated in both sexes, all ages, and all but one studied regions of Taiwan. Of note was the biggest increment of prevalence (79%) among 7th graders (students aged 13 years) through these 3 years. Annual incidence rates did not differ between 1999 and 2000 and 2000 and 2001 (6.1% vs. 5.7%; P = 0.4). One-year persistence rates of migraine diagnosis, surrogates of migraine duration, did not differ between 1999 and 2000 and 2000 and 2001 (34.2% vs. 41.2%; P = 0.1). Our study found that the prevalence of migraine was increasing in our sampled adolescents, which results from an increment starting at age 13 or younger. The prevalence of migraine in Asians might be increasing, although previous studies showed lower prevalence in this region. Children or adolescents may be more vulnerable to the environmental or societal change.
Introduction
Migraine prevalence starts to rise in puberty, especially in girls. It is a common headache disorder among adolescents, in whom it frequently causes disability and absence from school (1, 2). Recent epidemiological studies have adopted the migraine classification criteria proposed by the International Headache Society (IHS) in 1988 (3), though several groups have suggested revisions for children and adolescents (2, 4, 5). The International Classification of Headache Disorders, 2nd edition (6), does not substantially change these diagnostic criteria for children and adolescents. These standards make comparisons between different studies possible. However, the prevalence is still discrepant among studies. For example, two studies in Europe revealed 1-year prevalence rates of 2.9 and 19% in adolescents aged 13–15 years (2, 7).
Trends in the prevalence of migraine among adolescents have not been fully described. An important but controversial issue is whether the prevalence is increasing in children or adults (8–12). Although some study results support an increase, methodological artefacts have been suggested (12, 13). We previously validated a headache questionnaire and performed a pilot migraine survey in adolescents aged 13–15 years from four junior high schools (14). Using the same paradigm to diagnose migraine, we examined data from a large representative sample of 7th to 9th graders in five junior high schools for three successive years to determine if the prevalence of migraine is increasing or not.
Methods
We conducted population-based questionnaire interviews in all students from five public junior high schools in 1999, 2000, and 2001. Because our study focused on trends in migraine diagnosis, we surveyed the 1-year prevalence of migraine, i.e. the headache profile of the previous year. The study protocol was approved by the Institutional Review Board of the Veterans General Hospital.
Target population
To obtain national representative data, we chose schools from different geographical regions: two in northern Taiwan (Shi-Pai, Ta-Chi), one in central Taiwan (Yun-Lin), one in southern Taiwan (Nei-Pu), and one in eastern Taiwan (Yu-Li). Ta-Chi and Shi-Pai, which were in Taipei, represented the urban regions. Because the population density was higher in the north and because 69% of Taiwanese inhabitants live in the cities, we sampled two schools in northern Taiwan. Students from these two schools represented about one-half of the total sample. In contrast, Yun-Lin, Nei-Pu and Yu-Li were rural areas. About 25% of the students of the Yu-Li Junior High School were of aboriginal origin and accounted for 3% of the total sample population, although the percentage of aboriginal people is 1.9% of the total population in Taiwan.
In Taiwan, education is obligatory from the ages of 6 to 15 years. Students aged 6–12 years attend elementary school, and those aged 13–15 years attend junior high school. More than 90% of the latter are enrolled in pubic schools, with the remainder attending private ones. Among 867 junior high schools in Taiwan, only 107 are private and they represent 9.4% of the total students. All junior high schools in Taiwan are required to adopt the same curriculum. The Ministry of Education prescribes specific standards for the curriculum and instructional materials for schools under its jurisdiction. Therefore, the most obvious difference among the schools is their location: rural or urban.
Sampling method and questionnaire survey
All students from the five schools were invited to participate. To evaluate trends in migraine prevalence and incidence, we used identical methods and questionnaires for three consecutive years. We first sent letters describing our study objectives and methods to the school principals for their approval. Then, all students were asked to answer the self-administered questionnaire. We analysed data from the completed questionnaires by using a computer algorithm.
Headache questionnaire and diagnosis of migraine
We modified a validated self-administered questionnaire developed in our previous study to diagnose migraine from the previous year (14). The questionnaire was based on the 1988 IHS diagnostic criteria for migraine in adolescents (3); part of the questionnaire has been published elsewhere (14).
Diagnoses were made according to the criteria for migraine without aura (IHS code 1.1) (3). Students had migraine if they had a headache attack lasting 2–48 h and if the attack had any two of the following pain characteristics: unilateral location, pulsating quality, moderate to severe intensity, and aggravation by routine physical activity. Moreover, the attack had to be associated with at least one of the following symptoms: nausea, vomiting, or photophobia plus phonophobia. The criterion of ‘at least 5 attacks’ was not mandatory in this study (14). We did not attempt to diagnose migraine with aura because the validity of the questionnaire was not satisfactory for this purpose (14).
Statistics
Sex-, grade-, and region-specific 1-year prevalence of migraine were reported as the number of cases per 100 students with 95% confidence intervals (CIs). Incidence rates were based on the data from students who participated in at least two consecutive surveys. Students who did not have a diagnosis of migraine during the first survey were assumed not to have had migraine before the survey. The annual incidence was calculated by using a direct method, i.e. newly diagnosed cases of migraine per 100 students who did not have migraine in the previous survey. Student t and χ2 tests were used for comparisons when appropriate. Trend analysis was used to test changes in migraine prevalence for different calendar years. A P-value of < 0.05 was considered statistically significant. All statistical analyses were performed using SAS software version 8.2 (SAS Institute Inc, Cary, NC, USA).
Results
Participants
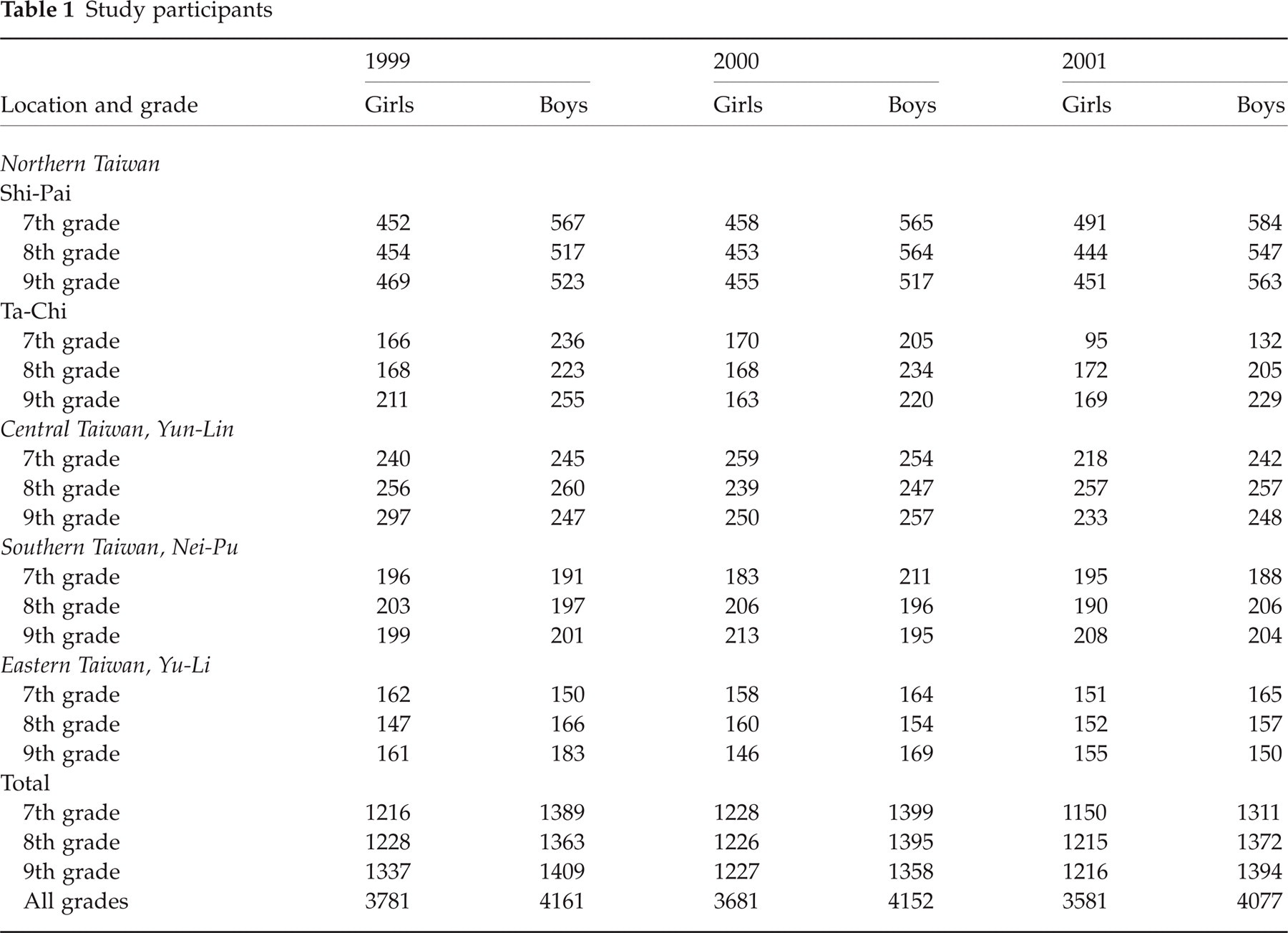
During the study period, 23 433 questionnaires were completed in the five schools: 7942 in 1999, 7833 in 2000, and 7658 in 2001 (Table 1). Response rates over the 3 years were 97%, 98% and 99%. Absence on the day of data collection was the primary reason for non-participation. Of the total 13 426 students, 5833 were surveyed once, 5179 were surveyed for two consecutive years, and 2414 were surveyed for three consecutive years. Based on the results of the 3-year survey, the overall percentage of school change per year was 3.3% for transference into these five sampled schools and 2.7% for transference out.
Study participants
Boys accounted for 52%, 53% and 53% of the participants for the 3 years. For girls, frequencies of having menstrual periods did not differ in the three surveys, with rates of 88.6%, 89.7% and 90.4%. Among 7th grade girls, the frequency of menstruation was increased slightly but non-significantly, with rates of 75.9%, 77.9% and 78.7% through the three surveys.
One-year prevalence of questionnaire-diagnosed migraine
Table 2 shows that the prevalence of migraine was higher in girls than in boys for all calendar years and grades. Prevalence increased from the 7th to the 9th grade in both sexes. Of note, the prevalence increased with time from 5.2% in 1999 to 7.4% in 2001 (P < 0.001; test for trend). This trend was found in both girls and boys. The increasing prevalence was most obvious in 7th graders of both sexes from 1999 to 2001, with the increments of prevalence as follows: both sexes, 3.0% (79% increment), P < 0.001; girls, 3.8% (86% increment), P < 0.001; and boys, 2.4% (75% increment), P = 0.003 (all test for trend). This increasing trend was observed in all three grades if data from both girls and boys were combined. Except for the Yu-Li Junior High School in the Eastern region, the trend was demonstrated in all other regions in Taiwan (Table 3).
One-year prevalence of migraine

Data in parentheses are 95% CIs.
Test for trend.
Region-specific prevalence of migraine
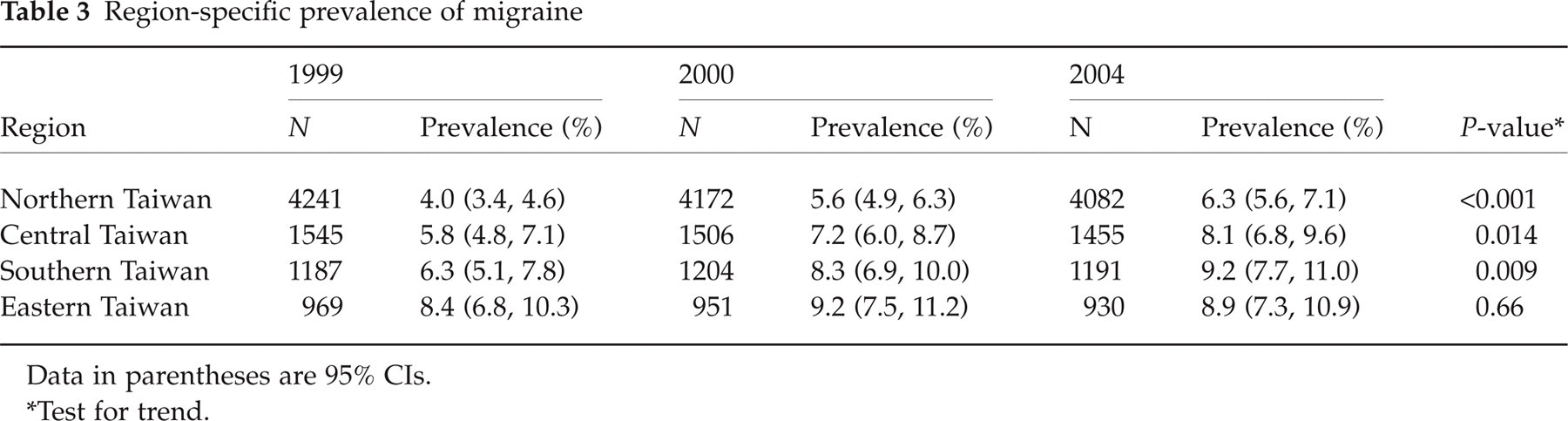
Data in parentheses are 95% CIs.
Test for trend.
Annual incidence of migraine
Annual incidence rates of migraine were based on data from students who participated in the survey for at least two consecutive years. Table 4 shows the incidence rates and corresponding 95% CIs by region, year, and sex. Annual incidence rates of migraine were in the range of 3.0–12% and were significantly higher in girls than in boys. Students in southern Taiwan had the highest rates. However, incidence rates did not differ between 2000 and 2001 (6.1% vs. 5.7%; P = 0.4). Likewise, sex- and region-specific incidence rates did not differ between 2000 and 2001.
Sex-, year- and region-specific annual incidence rates of migraine

Persistence of migraine diagnosis in 1999–2000 and 2000–2001
Among the 228 students in whom migraine was diagnosed in 1999, 78 (34.2%) continued to have migraines, as diagnosed in the 2000 survey. In comparison, the 1-year persistence rate of migraine diagnosis in those identified in 2000 was 114 (41.6%) of 274 through the year 2001. The rates for these two calendar years did not differ significantly (P = 0.1).
Discussion
This large-scale, nationwide, 3-year study enabled us to observe trends in the prevalence of migraine in Taiwanese adolescents. The 1-year prevalence of migraine increased 42% from 5.2% in 1999 to 7.4% in 2001. Incremental increases in the prevalence were observed in both boys (from 4.5% to 5.9%) and girls (from 6.0% to 9.1%). These increments were demonstrated in all areas of Taiwan except for the eastern region. Although the increase occurred in all grades, the biggest change in migraine prevalence was noted in 7th graders (79% increase from 3.8% to 6.8%) in boys and girls from 1999 to 2001.
Compared with previous studies (8–10), our study had several strengths: (i) we used identical questionnaires and methods for three consecutive years, preventing bias derived from case-finding and ascertainment; (ii) we used a large-scale, population-based, systematic annual survey rather than clinic-based studies; and (iii) a standardized IHS migraine diagnosis was used.
The increase in prevalence depends on increases in either incidence rates or disease duration. In this study, the persistence of migraine diagnosis, a surrogate of migraine duration, did not differ significantly from 1999 to 2000 (34.2%) or from 2000 to 2001 (41.2%). Incidence rates were also similar from 1999 to 2000 and from 2000 to 2001, suggesting that the occurrence of the new-onset migraines was stable when the participants became 8th or 9th graders. Therefore, the increase in migraine incidence must have occurred during or before the 7th grade. However, those incidence rates were not obtainable with our study design. The exact cause of this increase in prevalence among 7th graders is unknown. We do not know if the increasing academic competition as early as in the elementary schools (i.e. before junior high schools) might have contributed to this phenomenon. A Finnish study showed that starting school was also associated with an increase in the incidence of headache in children, independent of other factors (15). In this survey, it is also noted that the prevalence of migraine was highest in eastern Taiwan, but a trend of increasing prevalence was not shown here. Compared with other areas in Taiwan, this region has the lowest socioeconomic status and the highest proportion of aboriginal people. We are not sure whether ethnic, socioeconomic or environmental factors play a role in the change of migraine prevalence in adolescents.
The data on the increment of migraine prevalence among different surveys in children or adults seem conflicting (8–12). Sillanpaa and Anttila (8) evaluated the prevalence in two independent cohorts of 7-year-old children evaluated 18 years apart. In both studies, they interviewed children who were starting school in Turku, Finland, using a structured questionnaire and the Valquist criteria for diagnosing migraine (16). They found an alarming three-fold increase in the prevalence of migraine from 1974 to 1992. Reviewing data for medically recognized migraine in Olmsted County (Minnesota, USA), Stang et al. (9) reported that the incidence of migraine increased 34% in women and 100% in men under age 45 from 1979 to 1981. In the same catchment area, Rozen et al. (10) reported that the incidence significantly increased in both women and men over 11 years (1979 through 1990). Increments were 99% in girls and 46% in boys (aged 0–9 years) and 68% in female adolescents and 89% in male adolescents (aged 10–19 years). In contrast, two methodologically identical national surveys in the USA conducted 10 years apart (1989 and 1999) showed that the prevalence of migraine had remained rather stable over the last decade (11). Two surveys done in Hong Kong Chinese aged 15 or older showed a marked increase in the prevalence of migraine between 1992 and 1998 (12). We do not know the exact reasons for the discrepancy among these studies besides methodological differences. We postulate that racial and socioeconomic differences among different countries might be responsible (16). Similar to the development of Asian countries like Taiwan, the prevalence of migraine in Asians might be gradually catching up with Western countries when their societies become more westernized and competitive. In addition, children and adolescents might be more vulnerable to this influence.
Our study had some limitations. First, migraine was diagnosed by means of questionnaire survey rather than person-to-person interviews, although our questionnaire was validated. This limits comparisons of our results with those of other studies. Second, the criterion of ‘≥ 5 attacks in the lifetime’ was neither used as a questionnaire item nor considered a requisite for the diagnosis of migraine without aura in this study. This might overestimate migraine prevalence and underestimate the persistence rates at follow-up. We do not know the exact percentage of those with migraine without aura in our study, who had fewer than five attacks in their lifetime. However, we consider this proportion minor (about 4–6% through the 3 years) by calculating those with migraine without aura, who reported both frequency of less than one attack per month and onset after the 5th grade. In addition, since we used the same paradigm to diagnose migraine without aura for three consecutive years, the findings of the increment of migraine prevalence were still valid. Third, a learning effect and an awareness of the illness are inevitable biases in repeated surveys; however, they do not account for our finding that the most noticeable increase in prevalence occurred in 7th graders. Fourth, this annual-survey study spanned only 3 years, as opposed to previous studies (8, 10). Longer longitudinal studies are needed to confirm the trend of increasing migraine prevalence in adolescents. Fifth, ethnic and cultural diversity in migraine prevalence has been reported between Asian and Western populations; this should be taken into consideration in extrapolating our data (17). Sixth, to calculate incidence rates, we assumed that the students without migraine during the initial survey had had no previous migraine. Because some students might have had migraine before our survey, we may have overestimated the incidence rates.
Footnotes
Acknowledgements
This study was supported by grants from the National Science Council (NSC 90-2314-B-010-026).