
Abstract
Logistic regression was used to evaluate the relationship between self-reported medical diagnosis of migraine, self-reported depressive symptomology (RDS) and self-reported anxious symptomology (RAS) in the National Health Interview Survey (n = 30 852). Semipartial squared correlations evaluated the population-level variability between RDS, RAS and migraine impairment. Migraine prevalence was 15.2% (overall), 20.5% (women) and 9.4% (men). Migraine risk was higher in participants with RAS [odds ratio (OR) 2.30, 95% confidence interval (CI) 2.09, 2.52), with RDS (OR 2.23, 95% CI 1.93, 2.58), who smoked (OR 1.19, 95% CI 1.09, 1.30), or who consulted a mental health provider (OR 1.45, 95% CI 1.27, 1.65). Although migraine risk was increased in both women (OR 1.93) and men (OR 2.42) with RAS (P < 0.001), men with RAS had a higher migraine risk than did women with RAS (P < 0.001). Only 7% of the variability in migraine impairment (population level) was predicted by variability in RDS and/or RAS.
Introduction
Migraine is a common and disabling disorder (1–3). The American Migraine Study I and II and the American Migraine Prevalence and Prevention (AMPP) studies reported that the 1-year prevalence of migraine was approximately 18% for women and 6% for men (1,2). The World Health Organization Report 2001 listed migraine as the 19th leading cause of years lived with disability (YLD); for women of all ages, it is the 12th leading cause of YLD (3). Unipolar depressive disorders were ranked first in both sexes and across all ages.
Migraine has physical and emotional ramifications for individual sufferers and economic ramifications for both individuals and society. Migraine may have a substantial impact on occupational or academic performance, social activities and family life (4–7). Migraineurs are affected not only during attacks but perhaps also between attacks (i.e. interictal burden) (8). Migraine sufferers have reduced health-related quality of life relative to their peers (9). Interictal burden may lead to anxiety and feelings of hopelessness and helplessness.
Epidemiological studies have shown that migraine is comorbid with a number of psychiatric disorders, including generalized anxiety disorder (GAD), major depressive disorder (MDD), panic disorder, bipolar disorder and personality disorders (10–18). A recent Canadian health survey reported that MDD, social phobia and panic disorder were significantly more common in migraineurs than in non-migraineurs, with odds ratios (OR) of 2.3 [95% confidence interval (CI) 1.9, 2.8], 2.3 (95% CI 1.9, 2.9) and 2.8 (95% CI 2.2, 3.6), respectively (18). Other data confirm that depressive symptoms (17) or anxiety disorders (16,17,19) are more common in migraineurs than in non-migraineurs. The economic impact of migraine is significantly compounded in patients with comorbid psychiatric and medical conditions (20).
Patients with comorbid psychiatric disorders may be less likely to respond to pharmacological and behavioural therapies (21) and may experience greater headache-related functional impairment (22). Chronic migraine and comorbid psychological conditions appear to be more strongly associated than episodic migraine and psychological comorbidities (23,24), raising the question of whether comorbid depression and/or anxiety predispose to the development of chronic migraine or chronic tension-type headache (23).
Migraine has a bidirectional relationship with MDD and GAD (14,15). Approximately one-half of patients with MDD reported headache worsening during or after a depressive episode (25). Even with evidence of an association between migraine and these psychiatric disorders, it is still unclear whether the severity of one predicts the severity of the other(s) and whether severity affects the causal direction of the interaction.
In addition to psychiatric comorbidities, demographic factors such as age (i.e. peak risk during mid adulthood) (1,18) and sex (approximately threefold higher prevalence in women) influence migraine risk (1). In women with migraine, migraine risk is highest during their childbearing years (1), with approximately 50% of female migraineurs (26,27) experiencing migraine attacks that are closely tied to their menstrual cycle (i.e. menstrual migraine). During the cycle days −2 to +3 days (menses start = day 1), there is a twofold higher risk of migraine, which is thought to be induced by the low oestrogen levels during this period (28). The presence of psychiatric comorbidity and migraine can be particularly influential in women. For example, one study found that female migraineurs, especially those with depression, were more likely to be absent from work than women without migraine, or without migraine and depression (29). Thus, female migraineurs experience substantial negative economic consequences caused by migraine and psychiatric disorders.
The goals of the current analysis of the National Health Interview Survey (NHIS) dataset were threefold. The first was to examine the prevalence of self-reported medical diagnosis of migraine in a large US population sample from the 2003 NHIS (n = 30 852). The second was to evaluate the association between self-reported depressive symptomology (RDS), self-reported anxious symptomology (RAS) and migraine in this sample. The third goal was to assess the variance that was shared at the population level between RAS, RDS and migraine impairment using semipartial squared correlations; this type of analysis determines the overlap in the population-level variance between multiple variables.
Methods
Study design
The NHIS, conducted by the Centers for Disease Control and Prevention, National Center for Health Statistics, Division of Health Interview Statistics, is a comprehensive epidemiological survey to determine the health of non-institutionalized Americans (30). NHIS uses a three-stage cluster probability sampling design, with planned oversampling in the black and Hispanic populations to obtain reliable overall population estimates. It is composed of the Basic Module (includes the Family Core, Sample Adult Core and Sample Child Core) and supplements. The Family Core collects socioeconomic data for all family members, including family composition, demographics, health status, activity limitations, injuries, health insurance coverage and use of health services.
Participants and survey questions
Trained interviewers administered the NHIS questionnaire to all family members for the Family Core and to selected sample individuals. One randomly selected individual aged ≥ 18 years from each family completed the NHIS Sample Adult Core questionnaire. Participants were questioned about whether a doctor had diagnosed a wide range of health-related conditions. These conditions included having migraine within the past 90 days or RAS, RDS, or emotional problems within the past 30 days. Adult sample data from the 2003 NHIS (n = 30 852) were screened for participants who indicated that they had migraine. Participants with missing data on migraine were excluded. RAS and RDS were assessed using the following questions: ‘During the past 30 days, how often did you feel “restless/fidgety” or “nervous?” ’ (for RAS) and ‘During the past 30 days, how often did you feel “that everything was an effort” or “hopeless” or “worthless?” ’ (for RDS). These items were scored on a categorical scale (1, all of the time; 5, none of the time). The item responses were reverse scored before the present analysis so that lower scores reflected greater impairment.
Analyses
Demographic data for the NHIS population were summarized using descriptive statistics for age and sex. Migraine prevalence was weighted to arrive at the national estimate using sampling weights from the NHIS. These sampling weights reflect the probability of selection and adjustment for non-response and were calibrated to the 2000 Census for age, race/ethnicity and sex of the US population. These sampling weights allowed the results to be generalized to the entire population of the USA. Logistic regression modelling was performed to evaluate the relationship between self-reported migraineur status and sex, age, RDS, RAS and different interactions between these factors. Age was categorized in the model to account for an apparent non-linear relationship with the migraineur status. The age cut-offs were determined by a multivariate adaptive regression spline model; these estimates were not sex stratified (Figure 1). Semipartial squared correlations (sr2
) were computed and used to evaluate the associations between the variability, at the population level, in RDS, RAS and migraineur status (yes/no) in the NHIS population. As such, semipartial squared correlations are not measures of the prevalence of comorbidity; instead, they represent the correlation between two variables while holding a third variable constant (e.g. correlation between depression and anxiety while holding migraine constant for depression but not anxiety). Semipartial squared correlations are used to determine the overlap of variance between multiple variables in population studies (graphically displayed in Venn diagrams).
Using data from the National Health Interview Survey, age thresholds* were established using multivariate adaptive regression spline models, which plotted age (abscissa) against migraine prevalence (ordinate). *Each point on the figure is the prevalence of migraine at that specific age. The curved line is the spline and the two vertical lines are the inflection points of the curve that determined the age cut-off levels.
All evaluations of the NHIS data were performed using Stata® version 9.2 (StataCorp LP, College Station, TX, USA; NHIS and DTT menstrual migraine study) or R version 2.3 (R Foundation for Statistical Computing, Vienna, Austria; NHIS data only).
Results
Demographics
The 2003 NHIS included 35 921 households, which contained 92 148 people in 36 573 family units. Data for migraine were assessed from 30 790 individuals from the Sample Adult Core. Missing data on migraine status were minimal (n = 62) and were excluded. More women (n = 17 394) than men (n = 13 396) were in the sample, representing approximately 212.7 million non-institutionalized civilian US adults. The mean age for women and men with migraine was 41.3 years (95% CI 40.7, 42.0) and 41.1 years (95% CI 40.0, 42.1), respectively, compared with 47.4 years (95% CI 47.0, 47.8) and 44.7 years (95% CI 44.3, 45.1) for non-migraineur women and men, respectively.
Association between age, sex and migraine (NHIS)
Prevalence of migraine from NHIS survey by sex and overall

Migraine prevalence was weighted to arrive at the national estimate using sampling weights from the NHIS. These sampling weights reflect the probability of selection and adjustment for non-response and were calibrated to the 2000 Census for age, race/ethnicity and sex of the US population.
NHIS, National Health Interview Survey.
Risk factors for migraine in NHIS population using a single model that includes all variables*

Model was adjusted for age, sex and age by sex interactions.
Suggests that RAS is less of a risk factor for migraine in women than in men.
NHIS, National Health Interview Survey; OR, odds ratio; RAS, reported anxious symptomology; RDS, reported depressive symptomology; S.E., standard error; t, t statistic.
Risk factors for migraine in the NHIS population using sex-specific individual models
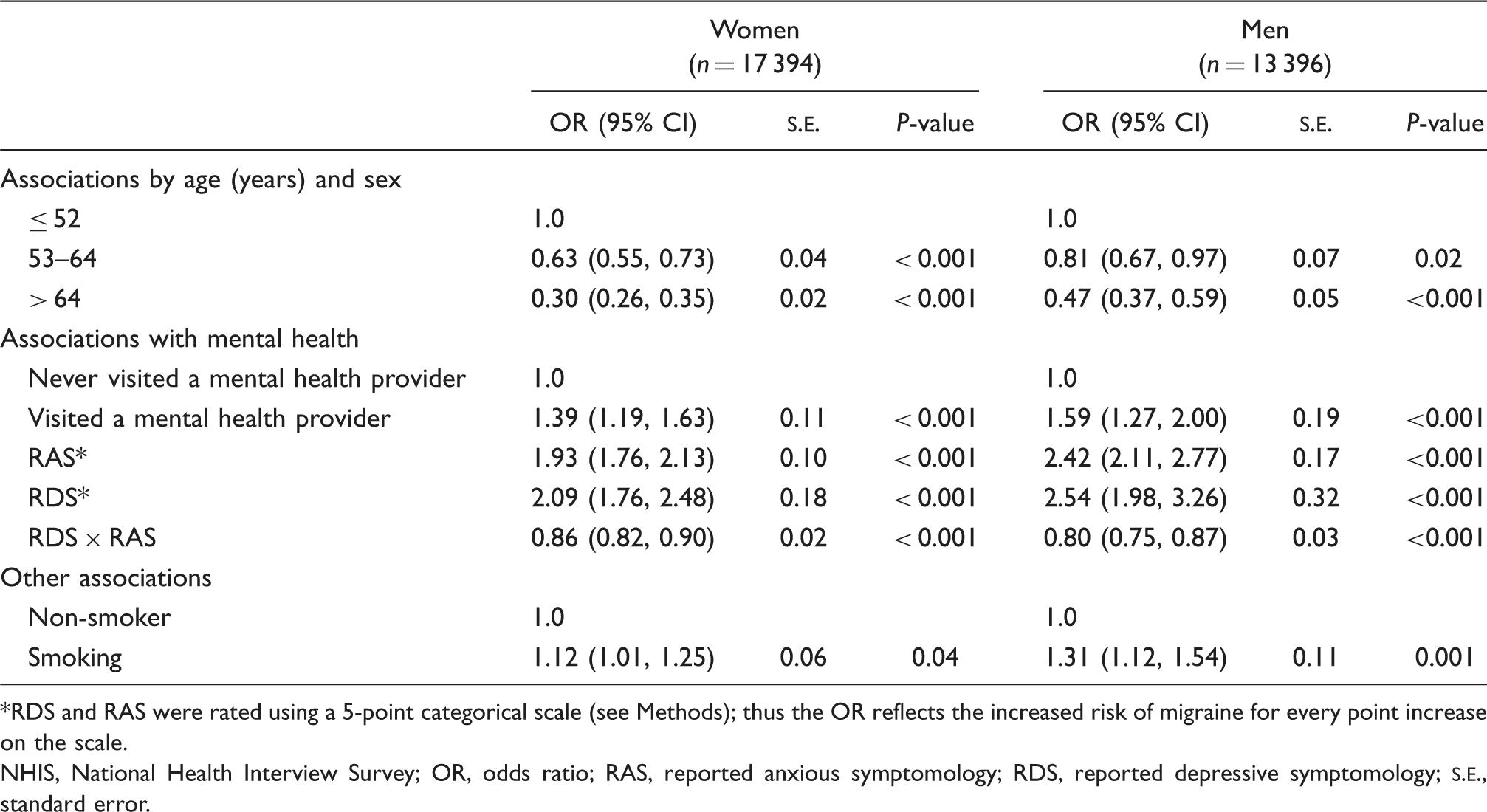
RDS and RAS were rated using a 5-point categorical scale (see Methods); thus the OR reflects the increased risk of migraine for every point increase on the scale.
NHIS, National Health Interview Survey; OR, odds ratio; RAS, reported anxious symptomology; RDS, reported depressive symptomology;
Association between RAS, RDS and migraine
When the NHIS population was evaluated using the single model to compare the associations of all covariates (model included both sexes), RAS (OR 2.30, 95% CI 2.09, 2.52), RDS (OR 2.23, 95% CI 1.93, 2.58), smoking (OR 1.19, 95% CI 1.09, 1.30) and having consulted a mental health provider in the past year (OR 1.45, 95% CI 1.27, 1.65; adjusted for RAS and RDS) increased the risk of having migraine (Table 2). Similar findings were noted when using sex-specific modelling (Table 3). In both sexes, RDS, RAS, visiting a mental health provider and smoking all increased the odds of migraine (all P < 0.001; Tables 2 and 3). Men had higher ORs for RAS (OR 2.42, 95% CI 2.11, 2.77) and RDS (OR 2.54, 95% CI 1.98, 3.26) than women (OR 1.93, 95% CI 1.76, 2.13; OR 2.09, 95% CI 1.76, 2.48, respectively, Table 3). RAS increased the probability of migraine in men (130%) when compared with women (98%). This is confirmed by the single model (Table 2) anxiety × women interaction (OR 0.86), which shows that women with RAS had lower risk for migraine than men with RAS.
From the NHIS population, RAS and RDS had an antagonistic interactive relationship on the risk for migraine, which can be noted by the OR < 1 [Table 2 (sex-combined model): OR 0.84, 95% CI 0.80, 0.84; Table 3 (by sex models): women, OR 0.86, 95% CI 0.82, 0.90; men, OR 0.80, 95% CI 0.75, 0.87]. Graphically, this is displayed in Figure 2, in which the level of self-reported depression (abscissa) is plotted against the odds of migraine (ordinate) for each level of RAS (Anxiety = 1–5). As the severity of RAS increased, the effect of RDS on the odds of migraine decreased. For example, in the individuals with the highest RAS (Anxiety = 5), the negative slope of the line suggests that as the level of RDS increased, the odds of migraine decreased, indicating an antagonistic relationship. Explained another way, the most anxious individuals (Anxiety = 5) had increased odds of migraine regardless of whether they also had significant depressive symptoms. In contrast, lower RAS scores (e.g. scores ≤ 3) with higher RDS scores showed a more linear increase in odds of migraine (i.e. steeper sloped lines). For each increase in RAS score, the slope of the line decreased, indicating less effect of increasing RDS scores on the odds of migraine, most notably seen with RAS scores of 4 (low slope) or 5 (negative slope).
The simultaneous relationship of reported depressive symptomology and reported anxious symptomology [grade 1 (mild) to grade 5 (severe)] relative to the odds of migraine from the National Health Interview Survey population.
In the NHIS, semipartial squared correlations show that approximately 7% of the variation in migraine impairment at the population level was predicted by RDS or RAS alone or in combination (Figure 3). The combination of RAS and RDS shares 4.3% of the variability in migraineur impairment. In looking at both comorbidities individually, RAS had a larger unique association (2.1%) to migraineur status than RDS (0.7%) at the population level (Fig. 3). As a reminder, squared semipartial correlations (sr2
) represent the unique amount of shared variance between two variables while controlling for the third variable; they are used to determine the overlap of variance between multiple variables in population studies and are graphically displayed using Venn diagrams. They do not represent overlapping prevalence rates.
Venn diagram of the semipartial squared correlations between migraine, reported depressive symptomology and reported anxious symptomology from the National Health Interview Survey. Semipartial squared correlations are not measures of the prevalence of comorbidity; rather, they represent the correlation between two variables while holding a third variable constant (e.g. correlation between depression and anxiety while holding migraine constant for depression but not anxiety).
Discussion
Our analyses of migraine, RAS and RDS in the NHIS sample support previous findings indicating that MDD and GAD (14,15) are common comorbid disorders in persons with migraine. In the analysis of the NHIS data, important correlates of migraine, in addition to RAS and RDS, include female sex (OR 3.43), smoking (OR 1.19) and prior consultation with a mental health provider (OR 1.45). Age was also an important risk factor; migraineurs were younger than non-migraineurs, and odds of migraine were substantially reduced in people > 52 years old (52–64 years, OR 0.80; > 64 years, OR 0.46). Although comorbid RDS and RAS were associated with migraine in both sexes (P < 0.001 for both), the effect was greater for men with RAS than for women with RAS (P < 0.001), with the probability of migraine increasing by 130 and 98%, respectively, in each sex.
For perspective, studies evaluating psychiatric disorders in migraineurs (11,18) have reported a higher prevalence of anxiety and depression than in the general population. For example, McWilliams and colleagues reported a 12-month prevalence of 28.5% for depression and 9.1% for GAD in US migraineurs (11). In contrast, in the general US adult population, the National Comorbidity Survey Replication study showed that the 12-month prevalence for MDD and GAD is approximately 7.0 and 3.1%, respectively (31,32). Our analysis provided additional information by showing that that RDS and RAS contribute to the risk of migraine (OR 2.23; OR 2.30, respectively); thus, they exhibit a high level of comorbidity. Nonetheless, our analysis, using semipartial squared correlations (Venn diagrams), suggests that > 90% of the variability in migraine impairment, at the population level, is wholly independent of variability in RAS or RDS. Only 4% of the variability (in the population) for all three outcomes was shared. Less than 3% of the variability in migraine impairment was uniquely shared with RDS (or RAS). These data suggest that other factors (e.g. different pathological mechanisms), outside of RDS or RAS, may contribute to the variability of migraine impairment at the population level.
Our analysis of the variance in psychiatric comorbidities and migraine at the population level is supported by other research. The Canadian Community Health Survey (CCHS) found that MDD had a substantially higher lifetime prevalence in migraineurs (18.8%) than in non-migraineurs (9.8%) (18) or in those with other chronic illnesses (33). Nevertheless, in studies in people with MDD, although comorbid migraine increased anxiety scores, it accounted for only 5–11% of the variance of the total scores on three psychometric depression scales (25). Our data, taken together with other research (25), suggest that additional factors, outside of depressive or anxious symptomology, contribute to the variability of migraine impairment within the population.
There are some possible limitations of the current analyses. First, the NHIS relies on self-reported physician diagnosis of migraine, which could possibly lead to under-ascertainment and misclassification. This limitation is partly mitigated by a 2008 study that found that 90% of general practitioners (n = 705) accurately diagnosed migraine (34). Physician diagnosis of migraine is reasonably specific, but not sensitive (35). Our estimation of migraine prevalence from men (9.4%), women (20.5%) and the total population (15.2%) from the 2003 NHIS was slightly higher than that reported by other epidemiological analyses, such as the AMPP study, which used the International Classification of Headache Disorders, 2nd edn criteria (5.6%, 17.1% and 11.7%, respectively) (1) and the 2002 CCHS (men 6.1%; women 15.2%; total not listed), which used respondent self-report (i.e. methodology similar to the NHIS). There were differences in the sampling populations between these studies; compared with the NHIS (92 148 individuals), the overall person count sampled was higher in the AMPP study (162 576 persons) and lower in the CCHS (36 984 individuals). Furthermore, the NHIS (30) and CCHS surveys (18) used different interviewer questions regarding the migraine diagnosis, and Canada and the USA have fundamentally different healthcare systems; these differences might explain the differences in prevalence rates between the two similarly designed studies. Despite the slight differences in overall prevalence, all studies clearly show that women experience migraine at two to three times the rate of men and that women in their reproductive years are most susceptible (1,18).
Another limitation to note is that the NHIS does not incorporate a validated screening instrument for anxiety and depression, but instead uses self-report questions that assess depressive and anxious symptomology. Thus, the methodology used is not validated and the criteria not as comprehensive as the Diagnostic and Statistical Manual of Mental Disorders, 4th edn criteria for anxiety and depression. The criteria used to measure RDS and RAS in the NHIS were developed by the Centers for Disease Control and Prevention to measure anxious and depressive symptoms on a population level. Even so, no research has directly correlated the results from the NHIS single screener questions with the Diagnostic and Statistical Manual of Mental Disorders 4th edn criteria, and consequently, our results need to be confirmed.
Another potential limitation of the current analyses was that the NHIS survey did not evaluate a causal relationship between migraine and either RAS or RDS, mainly because the NHIS was a cross-sectional study. Consequently, no inference can be made as to whether one disorder predisposes the person to the other disorder(s). In the current analyses, we could only determine that there is a strong association, but not the causal direction of that relationship. In controlled cohort trials, which are better suited to addressing these questions, a bidirectional association was found between depression and migraine (36,37) as well as anxiety (e.g. panic disorder) and migraine (38). The data from the NHIS study also do not permit us to assess how migraine's associated symptoms contribute to either RDS or RAS, another possible limitation. Some research suggests that it is the associated symptoms (e.g. dizziness, weariness, back pain, palpitations) that truly contribute to the comorbidities of depression and anxiety, not the headache pain itself (39). The degree of migraine-related functional impairment is also likely to mediate depression and anxiety. Nonetheless, these analyses provide pertinent information on the association between migraine impairment, RDS and RAS. Overall, these study limitations are balanced by strengths associated with the analysis. The NHIS has tremendous breadth of coverage, with a high respondent rate and extensive sampling procedures, so that the data are broadly applicable to the whole US population and the study has potentially less bias than smaller clinical samples. The small amount of overlap in the variability at the population level between migraine impairment, RAS and RDS was interesting and deserves further study.
Conclusions
The current analysis of migraine prevalence in the USA confirms that (i) migraine mainly affects adults aged ≤ 52 years and (ii) that migraine disproportionately affects women (OR 3.43 vs. men aged ≤ 52 years; OR 5.03 vs. men aged ≥ 65 years; P < 0.001 for both). Furthermore, this analysis found that although RAS or RDS were risk factors for migraine in both sexes (P < 0.001 for both), men with RAS or RDS were at higher risk of migraine (OR 2.42; OR 2.54, respectively) than women with RAS (OR 1.93) or RDS (OR 2.09). Nonetheless, although data from the NHIS suggest that RDS, RAS and migraine are highly comorbid, our data (from the semipartial squared correlations) suggest that only around 4% of the variability in the outcomes, at the population level, was shared by all three disorders. A slightly higher percentage (7%) of the variability in migraine impairment was predicted by either RAS or RDS, alone, or in combination. Because this analysis found that > 90% of the variability in migraine impairment, at the population level, is wholly independent of the variability in RDS and RAS, it suggests that although migraine, depression and anxiety are highly comorbid, some of the pathological mechanisms behind these disorders might not be commonly shared among the three and that other factors are contributing to the variability in migraine impairment (outside of depression or anxiety) in the population. Enhanced physician knowledge about these complex interactions will enable them to offer appropriate treatment to migraineurs for both pain and comorbid psychiatric issues.
Footnotes
Competing interests
T.W.V. and R.E.W. were employed by Endo Pharmaceuticals Inc. at the time the research was conducted. All authors are either employed by Endo Pharmaceuticals, Inc., or have served on advisory boards and speakers bureaus, conducted research and received educational grants in association with various companies. D.C.B.: Allergan Pharmaceuticals, Endo Pharmaceuticals Inc., GlaxoSmithKline Pharmaceuticals, Merck Pharmaceuticals and OrthoMcNeil Neurologics Inc. R.B.L.: Advanced Bionics, Allergan Pharmaceuticals, AstraZeneca, Boehringer-Ingelheim, Bristol Myers Squibb, Cierra, Endo Pharmaceuticals Inc., GlaxoSmithKline Pharmaceuticals, Minster, Merck Pharmaceuticals, Neuralieve, Novartis, OrthoMcNeil Neurologics Inc., Pfizer, Pozen, ProEthics and St Judes Children's Research Hospital.
Acknowledgements
The authors would like to acknowledge the editorial support and manuscript preparation assistance provided by Kristine W. Schuler, MS and Kevin Ryder, PhD, of Complete Healthcare Communications, Inc. (Chadds Ford, PA, USA). Endo Pharmaceuticals Inc. (Chadds Ford, PA, USA) financially supported the research and the development of this manuscript. The sponsors were responsible for study design and statistical analyses of the data. The authors were responsible for the interpretation of the data and the preparation, review and final approval of the manuscript before submission. With the exception of R.B.L. and D.C.B., all authors are employees or former employees of the sponsors. All co-authors contributed scientifically to the manuscript, but T.W.V., as primary author, exercised editorial control with final responsibility for content decisions and conclusions.