
Abstract
Intravital microscopy on a closed cranial window allows one to measure change in the diameter of cranial blood vessels after intravenous (i.v.) administration of pharmacodynamic substances. Putative targets being pursued in migraine are large vasodilating peptide molecules such as calcitonin gene-related peptide (CGRP) and pituitary adenylate cyclase polypeptide (PACAP)-38. High i.v. doses are required to study their craniovascular pharmacology. Unfortunately, this leads to a drop in blood pressure (BP) that subsequently causes blood vessels to dilate by autoregulation. Hence it is difficult to decipher what effect is caused by direct receptor agonist interaction or contributed by autoregulation. In the present study we infused substances with an ingenious indwelling catheter in the common carotid artery in rats. Intracarotidly seven-, 12- and 17-fold lower doses of CGRP, PACAP-38 and capsaicin were required, respectively, compared with i.v. infusion to induce the same dilation in dural artery. Dilating intracarotid (i.c.) doses caused no or a minimal fall in BP, whereas equi-responsive i.v. doses caused a marked BP reduction. The CGRP blocking potential of olcegepant was amplified by > 20 times on i.c. infusion. Pial artery responses to CGRP did not change with i.c. infusion, demonstrating that dilations after i.v. CGRP are mediated by autoregulation rather than through specific receptors. We applied CGRP topically, which induced concentration-dependent dural vasodilation, but no effect on pial artery or on BP. In conclusion, this new approach offers an improvement of the existing model by allowing more accurate assessment of effects of pharmaca on the cranial vasculature without inducing significant systemic effects.
Introduction
The closed cranial window model in rats was developed by Williamson et al. (1) and monitors the change in dural artery diameter and was extended to include pial artery by Petersen et al. (2). In 1940 Ray and Wolff (3) reported that stimulation of meningeal as well as large pial/cerebral vessels induced referred pain of throbbing quality in patients undergoing brain surgery. Dilation of cranial vessels may be involved in migraine and is at least a biomarker for some other actions during the migraine attack, because almost all migraine-provoking agents known so far are vasodilators. Intravital microscopy on closed cranial window involves thinning of parietal bone to make it transparent, thus allowing continuous monitoring of cranial arteries without opening the skull. This model has led to better pharmacological understanding of mechanisms such as trigeminal activation (4) and dural vasodilation (5,6). An array of endogenous neuropeptides that have been implicated in migraine pathogenesis are predominantly large vasodilating peptides, such as calcitonin gene-related peptide (CGRP) (7,8) and pituitary adenylate cyclase polypeptide (PACAP)-38 (9,10). In this model, signalling molecules are administered in high doses in the femoral vein, as these agents have to trek systemically all the way to the cranial arteries and thus in the process get diluted in blood. However, this leads to a significant drop in blood pressure (BP), which activates autoregulatory mechanisms (11) leading to cranial vasodilation, which is also the experimental readout; thus it is not clear what amount of dilation is caused by direct action on receptor at cranial level and what part is contributed by autoregulation.
Intracarotid (i.c.) administration offers the possibility of delivering pharmaca nearer to the cranial vasculature, the site of interest, in much higher concentrations because of less dilution. Due to safety and ethical concerns, i.c. infusion is not possible in humans, but we have now explored this possibility in rats. We compared the effect of i.c. with that of intravenous (i.v.) infusion of various compounds on dural and pial arteries in the closed cranial window model. Besides CGRP, we studied capsaicin, which stimulates endogenous CGRP release (12) through activation of transient receptor potential cation channel V1 (TRPV1). We also studied PACAP-38, which has been recently shown to provoke migraine-like attacks in patients suffering from migraine without aura (10). We also investigated the effect of topical application of CGRP on the cranial vessels in the model. This approach, we believe, would mimic more closely the physiological state, as the pharmacon approaches the blood vessel abluminally in a similar fashion to that of molecules released endogenously from perivascular nerves, rather than molecules administered systemically.
Materials and methods
Surgical preparation
All the experimental procedures were performed in accordance with domestic
guidelines and regulations for animal care and treatment. The study protocol was
approved by The Danish Animal Experimentation Inspectorate (file: 2001/561-850).
Male Sprague-Dawley rats (362–461 g) were used and were
purchased from Taconic Europe (Tornbjergvej, Ejby, Denmark). They were housed
under a standard light–dark cycle and given free access to food and
water. Rats were anaesthetized with an intraperitoneal injection of
60 mg/kg sodium pentobarbital followed by
20 mg kg−1 h−1.
A tracheotomy was performed and the animals were artificially ventilated
(Abovent 7025; Ugo Basil, Milan, Italy) with a 30/70% air mixture of
O2/N2O (stroke rate 60–65/min and a stroke
volume of 3.5–4.0 ml). The body temperature was kept at
36.5–37.5°C using an automatic regulated heating plate
(Letica HB101; Panlab, Barcelona, Spain). The left carotid artery was then
exposed and a 2-cm part of the artery was secured with two bull dog clamps, one
towards heart and one towards brain. Then in the artery a very fine catheter
(outer diameter 0.3 mm) was introduced towards the heart (Fig. 1) and secured with tissue glue (3M™
Vetbond™ Tissue Adhesive; 3M Center, St Paul, MN, USA). This
ingenious technique allows the catheter to flow freely in the carotid artery
without compromising the circulation to meninges or brain, in contrast to
conventional cannulation, which blocks the blood supply completely through the
vessel after cannulation. Figure 1 shows the devised
catheter and standard polythene catheter to appreciate the size difference. By
removing the bull dog clamps, blood supply was restored after the cannulation
procedure within 10 min. The femoral artery and vein were cannulated
bilaterally with polythene catheters (Portex polyethylene catheters, internal
diameter 0.4 mm; Astratech, Tåstrup, Denmark) for
measurement of arterial BP (Transducer TCM4-7; World Precision Instruments Inc.,
Sarasota, FL, USA), collection of arterial blood samples, infusion of
anaesthetics and test substances. All data were continuously displayed on a
computer monitor by the data acquisition and analysis software Perisofts
(Perisofts for Windows 2.0; Perimed AB, Järfälla,
Sweden). Three to four samples of blood were withdrawn to analyse blood gases
(ABL520; Radiometer, Brønshøj, Denmark), which were kept
within physiological range (pH 7.35–7.45; pCO2
35–45 mmHg; pO2
90–120 mmHg). The rat was then placed in a stereotaxic
frame and the bone overlying a segment of the middle meningeal artery was
carefully drilled thin while constantly applying ice-cold saline until the
artery was clearly visible. The drilling of the skull induces vasodilation as a
result of mechanical stimulation. The animal was allowed to recover for
1–1.5 h before proceeding with the experimental
protocol. Upper panel shows the two cannulae, the upper cannula (external
diameter of 0.8 mm) used for femoral arteries and
femoral veins. Lower cannula used for indwelling cannulation of
carotid artery (external diameter of 0.3 mm) and each
small division on the scale represents 1 mm. Lower panel
shows cannula in the rat carotid artery oriented towards heart.
The drilled area was covered with mineral oil in order to prevent drying and facilitate the visualization of the cranial arteries (dural or pial artery). The artery was captured with an intravital microscope (model MZ 16; Leica Microsystem Ltd., Heerbrugg, Switzerland) using a cold source of light and a camera, to display images on a standard television monitor. The artery under study was continuously monitored and changes were measured with a video dimension analyser (Living Systems Instrumentation Inc., Burlington, VT, USA). The effects of CGRP, PACAP-38 and capsaicin were studied as detailed below.
Experimental protocols
In all experiments 150 µl of vehicle was infused (i.c. or i.v.) at the rate of 50 µl/min. Each dose was constituted in a volume equivalent to one-eighth of the weight of the animal; for example, a 416-g rat received 52 µl of drug solution. This was done to minimize the volume being injected into the animal and yet maintain enough volume to inject accurately. Each infusion was followed by 100 µl of saline to rinse catheters. We chose to infuse various pharmacological agents rather than giving a bolus injection in order to measure responses in more steady state and also eliminating variability due to differences in rate/method of injection. Intracarotid bolus injections induced transient change in the dural artery baseline value, and this disturbance could be minimized with infusion over 1 min. The successive gap between each dose was minimum 10 min or the time it took for the artery to return to baseline. The peak increase in arterial diameter and peak decrease in arterial BP were measured after every dose, within 1–2 min of drug administration. This protocol was followed throughout the study except when stated otherwise.
Intracarotid vs. intravenous administration
αCGRP infusion
Rat-
To evaluate how antagonists behave with change in route of administration we used 0.1–50 µg/kg olcegepant, a potent CGRP antagonist (13), to evaluate blockade of CGRP (0.10 µg/kg)-induced dilations. This dose of CGRP was chosen as it produced submaximal dilation of the dural artery on i.c. administration. Intracarotid olcegepant was administered over 1 min and 3 min later i.c. CGRP was infused.
Capsaicin infusion
Capsaicin was administered in increasing doses from 0.1 to 20 µg/kg. All the i.v. doses were administered over 20 s, whereas all i.c. doses were administered over 1 min. This was done based on the pilot experiments, where infusion over 1 min did not cause any change until 20 µg/kg and larger doses led to extreme changes in BP and prolonged dilations.
In the present study multiple doses of CGRP and capsaicin were given and previous studies in this model have already shown that repeated administration (three to seven times) of αCGRP and capsaicin produce reproducible changes in dural vessel diameter and BP in this model (2,12). We also used increasing dose of olcegepant (1–30 µg/kg) against i.c. capsaicin 1 µg/kg to block the dilatory responses. Similarly, i.v. olcegepant (10 and 30 µg/kg) was used to block the dilations induced by i.v. capsaicin 20 µg/kg. The protocol used for olcegepant vs. capsaicin was similar to that described for olcegepant vs. CGRP.
PACAP-38 infusion
Of the two endogenous analogues PACAP-38 and PACAP-27, we chose the predominant form in rat brain tissue, PACAP-38 (14), for our experiments. PACAP-38 was infused in doses ranging between 0.03 and 10 µg/kg.
Topical application
For the topical application experiments we used synthetic interstitial fluid (SIF, composition in mM: 108 NaCl, 3.48 KCl, 3.5 MgSO4, 26 NaHCO3, 11.7 NaH2PO4, 1.5 CaCl2, 9.6 sodium gluconate, 5.55 glucose and 7.6 sucrose; pH 7.4) as a vehicle for CGRP. The solution was aerated with carbogen for 10 min before addition of NaHCO3. In pilot experiments we first applied drug solution on the closed window with a syringe, but it distorted imaging of the vessels and care had to be taken while applying solution as even slight mechanical stimulation induced vasodilation. Therefore, in this series of experiments a polythene cannula was placed on top of the cranial window in contact with the skull without obstructing the view. Throughout the experiment a uniform flow of 20 µl/min of SIF was maintained. This ensured not only smooth tracking of dural/pial artery but also that the window did not dry up. CGRP was used for the topical experiments in concentrations from 0.01 to 10 µg/ml.
Compounds
Rat-
Data analysis
The diameter of the artery was measured in arbitrary units. Peak increase in the
artery diameter was expressed as per cent increase as calculated from the
prestimulation level. Prestimulation levels are defined as the average
measurement 60 s preceding the pharmacological intervention. The
dose–response curves were analysed to establish the maximum response
(
Results
A total of 60 rats were used for the study. However, six animals with abnormal blood gas parameter and pH reading, which could not be brought to normal physiological range, were excluded. We successfully used i.c. techniques for acute administration of signalling molecules to cranial vasculature.
Intracarotid vs. intravenous administration
Effect of αCGRP
Vehicle, 0.9% saline, did not induce any significant changes in measured
parameters. CGRP induced dose-dependent dilations in dural arteries on i.v.
as well as on i.c. infusion, as shown in Fig. 2. CGRP
ED50 values were
41.1 ± 7.7 and
298.3 ± 39.6 ng/kg for i.c.
and i.v., respectively. A representative trace of CGRP effect on BP and
dural artery diameter is shown in Fig. 3. There was
dose-dependent decrease in BP (Fig. 2). The
dural artery diameter increased significantly compared with control
(diameter after vehicle infusion) at 30 ng/kg and
300 ng/kg doses onwards intracarotidly and intravenously,
respectively. CGRP induced significant dilation of pial arteries at 3000 and
10 000 ng/kg (Fig. 4).
ED50 of CGRP for pial artery dilatation was found to be
882 ± 262 ng/kg. Significant
changes in MABP in case of i.c. administration were observed only at
300 ng/kg, the dose at which maximum dilation has been already
achieved. There were no significant differences observed in per cent change
of MABP between i.v. and i.c. CGRP doses. Effect of increasing doses of rat-α calcitonin
gene-related peptide (CGRP) on dural artery diameter (upper
panel), and blood pressure (BP) (lower panel) by intracarotid
(i.c.) and intravenous (i.v.) infusion.
* A representative recording of effect of calcitonin gene-related
peptide (CGRP) 50 ng/kg on blood pressure (BP)
(upper panel) and dural artery diameter (lower panel) after
intravenous (i.v.) and intracarotid (i.c.) infusion for
1 min. Effect of increasing doses of rat-α calcitonin
gene-related peptide (CGRP) on rat pial artery diameter (upper
panel), and blood pressure (BP) (lower panel) by intracarotid
(i.c.) infusion.
#


Olcegepant did not significantly alter dural artery diameter Effect of increasing doses of olcegepant on rat dural artery
diameter by intracarotid (i.c.) infusion.
#
Effect of capsaicin
Infusion of capsaicin vehicle was free of any significant effects on dural
artery diameter as well as BP. Capsaicin produced a characteristic response,
immediate vasoconstriction followed by sustained vasodilation. For
uniformity in statistical analysis we only compared the dilatory phase of
response between the two routes of administration. I.c. infusion produced a
significantly higher response at much lower doses (Fig. 6).
ED50 was 475 ± 64 and
8175 ± 1026 ng/kg with i.c.
and i.v. infusion, respectively. There was a significant increase in dural
artery diameter at doses of 500 and
≥ 10 000 ng/kg,
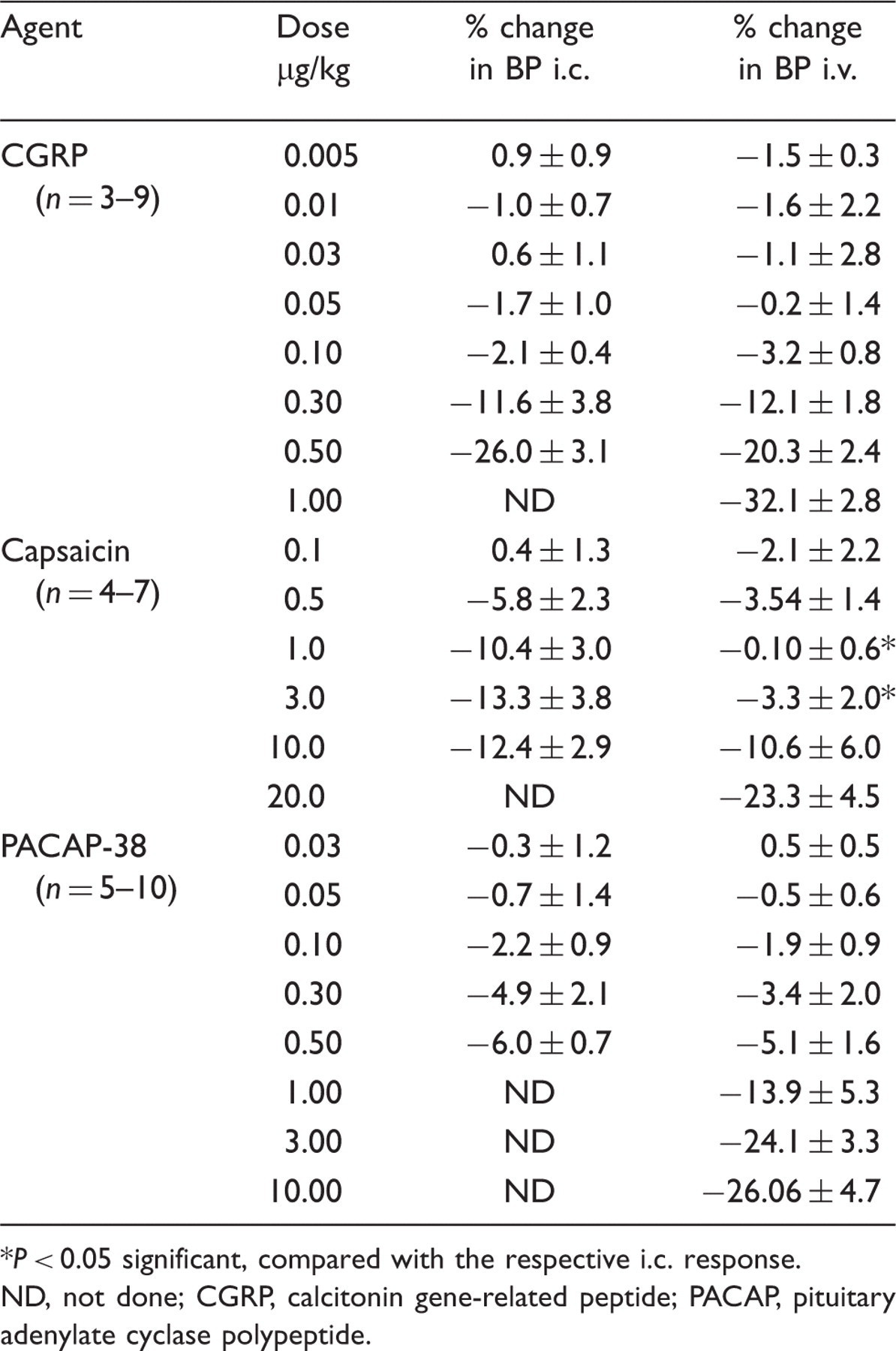
intracarotidly and intravenously, respectively. A dose-dependent decrease in
BP was observed, which was more marked in case of i.c. infusion compared
with i.v. infusion at lower doses (Table 1). There was a
significantly higher drop in MABP with 1 and 3 µg/kg
i.c. doses than the respective i.v. doses. Effect of increasing doses of capsaicin (upper panel) by
intracarotid (i.c.) and intravenous (i.v.) infusion.
* Effect of various agents and doses on blood pressure (BP) with
intracarotid (i.c.) and intravenous (i.v.) administration in
male rats
ND, not done; CGRP, calcitonin gene-related peptide; PACAP,
pituitary adenylate cyclase polypeptide.
Olcegepant significantly blocked the dilations induced by i.c. capsaicin 1 µg/kg (middle panel, Fig. 6). Olcegepant could block 50% response of capsaicin even in the highest dose of 30 µg/kg, the dose at which i.c. CGRP 0.1 µg/kg was almost totally blocked in the same experimental group (middle panel, Fig. 6). The dilations elicited by i.v. capsaicin were blocked in a dose-dependent fashion by olcegepant (lower panel, Fig. 6). In contrast to i.c. responses of capsaicin, i.v. responses were almost completely blocked with 30 µg/kg olcegepant (lower panel, Fig. 6).
Effect of PACAP-38
PACAP-38 produced a significant increase in the dural artery diameter (Fig. 7) from i.c. 50 ng/kg and i.v.
3000 ng/kg. I.c. infusion of PACAP-38 caused significantly more
potent dilations (ED50
134 ± 64 vs.
1624 ± 291 ng/kg) and
elicited higher maximal responses ( Effect of increasing pituitary adenylate cyclase polypeptide
(PACAP)-38 on dural artery diameter by intracarotid (i.c.) and
intravenous (i.v.) infusion.
*
Topical application
CGRP induced concentration-dependent dilations on the dural artery, as shown in
the sigmoid curve in Fig. 8. The Effect of increasing concentration of rat-α calcitonin
gene-related peptide (CGRP) on rat dural and pial artery diameter
(upper panel) and on blood pressure (BP) (lower panel) by topical
application on the closed cranial window.
#
Discussion
The closed cranial window model is one of the most prevalent preclinical migraine models (1,2) where drugs are administered intravenously to observe the effect on the cranial arteries. However, these dilating doses also cause a simultaneous fall in BP, which subsequently, due to autoregulatory mechanisms and circulatory reflexes, affect the diameter of cranial arteries. To circumvent this problem we decided to use the i.c. instead of the i.v. route. To achieve the same dilating effect we found that 7–17-fold lower i.c. doses were required than i.v. doses, the former causing no or only minimal decrease in BP.
The carotid arteries in dogs and pigs are sufficiently large to cannulate either approaching through a branch of the carotid artery or just by sticking an infusion needle into the common carotid artery. The rat artery, however, is too small, and conventional cannulation by ligation would occlude the blood supply to brain, not desired in this model. Therefore, we devised an extremely thin cannula (0.3 mm in external diameter, Fig. 1) and secured the cannula with tissue glue rather than with a suture, to retain unhindered blood supply. We cannulated towards the heart so that infused molecules were uniformly distributed in the blood supply to brain. To our knowledge, this is the first time that this technique has been utilized in rats for drug administration.
We validated the i.c. model using CGRP as a model molecule. This potent vasodilating peptide has been implicated and extensively investigated in migraine pathogenesis (8,15). I.c. CGRP 30 ng/kg produced a significant increase in dural artery diameter, whereas the corresponding i.v. dose was 300 ng/kg (Fig. 2). Dilating i.c. doses of CGRP did not decrease BP, whereas dilating i.v. doses decreased BP by 30%.
Even with i.c. infusion, pial artery diameter increased in the same dose range as
reported earlier by i.v. administration (2), implying that these responses
must be mediated by autoregulation rather than by direct receptor interaction. These
results are in line with those of Petersen et al. (16) showing that abluminal but not
luminal application of CGRP dilated rat pial arteries by using an
A 17-fold lower dose of i.c. capsaicin was required to induce a similar increase in dural diameter to an i.v. dose. Besides the lesser dilution of capsaicin in blood with i.c. infusion, another main factor is the hydrophobic nature of capsaicin (17), causing its preferential distribution into extravascular tissues after i.v. infusion. This is also evident from the fact that a bolus injection of i.v. capsaicin elicited an increase in dural artery diameter from ≥ 3 µg/kg dose (6), whereas infusion in the present study gave significant responses only from 10 µg/kg. Hence, a small change in the rate of administration of drug even by the same route can have a significant impact on the observed responses. The increase in potency of capsaicin cannot be attributed to lesser metabolism, as capsaicin has a long half-life (> 24 h) (17). Interestingly, at lower doses there was significantly more change in BP with an i.c. compared with the same i.v. dose, indicating central action of capsaicin on BP. This is probably because of capsaicin's hydrophobic nature, which may allow it to permeate across the blood–brain barrier and activate TRPV1 receptors (18) along with other receptors present in rat brain, and not only the receptors on blood vessels.
Capsaicin-induced dural dilations were significantly blocked by olcegepant at 3 µg/kg, but increasing its dose further did not produce more than 50% blockade. This is probably because capsaicin releases not only CGRP (19) but also substance P (20), PACAP (19) and neurokinin (21). However, in the same model Akerman et al. (12) found > 90% blockade of i.v. capsaicin responses with a less potent CGRP antagonist, CGRP8–37. In line with that study (12), when we administered i.v. capsaicin, its responses were almost completely blocked with the same dose of olcegepant (30 µg/kg), which inhibited only 50% of i.c. capsaicin responses. This, we believe, is because of systemic liberation of CGRP by i.v. administration and release of non-CGRP vasodilators by i.c. administration. Thus, i.c. administration of signalling molecules presents a more realistic insight into craniovascular pharmacology. Furthermore, Petersen et al. (2) have shown that olcegepant could block the response to transcranial electrical stimulation by > 80%, which shows responses are predominantly mediated by endogenous CGRP release. Thus, taken together, these studies indicate that to study the effect of local release of CGRP at dural level, transcranial stimulation is a better approach than capsaicin.
Recently it has been shown that PACAP-38 provokes migraine-like headache in migraineurs (10) and, expectedly, i.c. PACAP-38 dose-dependently dilated the dural arteries as shown earlier with i.v. administration (9). I.c. infusion of PACAP-38 not only induced dilations at 12-fold lower dose but also led to significantly higher maximal response in dural arteries compared with i.v. administration. This is probably because decrease in BP not only induces autoregulation but also activates other reflex/compensatory mechanisms that can modulate vasculature, such as the sympathetic nervous system. It has been shown earlier that a BP decrease of ≤ 30 mmHg (11) makes the dural baseline diameter erratic. In that study hypotension was induced by withdrawing blood, and in the present study dural artery diameter was affected not only by massive hypotension but also by direct receptor–agonist interaction by i.v. infusion.
In human migraine provocation studies signalling molecules are administered
intravenously. The drop in BP induced by these agents is the dose-limiting factor in
such studies. However, the effective doses in humans do not usually reduce BP as
drastically as observed in animal models, probably because unlike humans, animals
are anaesthetized. Therefore, the i.c. infusion model in rats with minimal effects
on BP comes closer to the experimental human model and, more importantly, to the
physiological state of migraineurs. As BP is not affected
We have demonstrated concentration-dependent dilations of dural arteries with topical application of CGRP without any change in BP. Topical application simulates release of perivascularly stored signalling molecules around blood vessels. In a similar study in rats with human-CGRP 10−4 M (378.9 µg/ml), topical application on dura, exposed by removal of parietal bone, increased dural blood flow by 15% (22). Exact comparison with our study is difficult since only a single concentration of human-CGRP was studied whereas we used rat-CGRP, which is around eight times more potent on rat CGRP receptors than its human counterpart (23). However, our observations suggest that the thin layer of parietal bone left in our model does not present a significant diffusion barrier even to large hydrophilic molecules to the dural vasculature. Both topical and systemic administration of CGRP dilated dural arteries in our study, whereas pial arteries did not respond to topical CGRP in the model. This shows that CGRP molecules do not permeate into pial arteries, as earlier studies have shown that abluminal application of CGRP can induce dilation in perfused rat arteries (16). Thus, for studying the responses in pial arteries abluminally, signalling molecules need to be applied on the open cranial window model (24).
In conclusion, both i.c. and topical administration of drugs represent useful methodological advances, and with these modifications the closed cranial window model is highly suitable to study and characterize the effects of molecules on the cranial vasculature.
Footnotes
Acknowledgements
This study was supported by The Lundbeck Foundation as part of the Lundbeck Foundation Centre for Neurovascular Signalling (LUCENS) and by Copenhagen County's Research Council, Danish Agency of Science, Technology and Innovation. We gratefully acknowledge Professor Lars Edvinsson for providing olcegepant and Michael Baun for the photographs for this manuscript.