
Abstract
Recurrent limb pain (RLP) is a well-known entity in childhood. It is considered a precursor of migraine. The temporal relationship of RLP with headache in childhood is lacking in the literature. However, there are many cases with limb pain in a close temporal relationship with migraine headache in adults. We report six female patients with RLP and migraine and delineate the temporal relationship between the two. Three patients had a history of RLP in childhood and developed migraine headache after many years. Conversely, two patients had a long history of migraine headache and later developed RLP. One patient developed RLP and migraine headache at the same age. Isolated limb pain was frequent in all six patients. It was mild to severe, for a few minutes to a few days, and predominantly located in the upper extremities. Only one patient reported allodynia. The patients showed response to preventive measures (all six patients) and abortive therapies (four patients), even in those attacks of RLP that were not associated with headache episodes. We also review the clinical profiles of the patients in whom RLP and migraine were related to each other, and speculate on the possible mechanisms for RLP in the patients with migraine.
Introduction
Headache and musculoskeletal symptoms frequently co-exist in the general population. The prevalence of chronic headache is reported to be more than four times greater in individuals with chronic continuous musculoskeletal symptoms than in those without (1). Epidemiological data regarding recurrent limb pain (RLP) in adults (and its relationship with headache) have not been explored in the literature. However, RLP has been extensively investigated in children, and about half of children with RLP are reported to have recurrent headaches (migraine). There is a suggestion of a common pathogenesis of RLP and childhood migraine (2). In fact, several authors have reported limb pain in a close temporal relation with migraine and cluster headache (CH) (3–7). There are only few cases of isolated independent episodes of limb pain or body pain (without migraine headache) in known migraine patients in the literature (3, 8). The literature is silent regarding the specific management of RLP (especially in children). There are a few case reports in which preventive and abortive treatments of migraine were effective in relieving RLP (having a temporal relation with headaches) (3, 5, 7, 8). Here we report six patients (collected over 2.5 years) with migraine headache in whom many attacks of RLP were not in a temporal relationship with headaches. We also review the clinical profile of the patients where limb pain and migraine headache were claimed to relate to each other.
Case reports
The main characteristics of the headache and limb pain of all six patients are summarized in Table 1. Two patients are described in detail. Written informed consent was taken from the patients to publish this report.
Main features of patients with recurrent limb pain

LL, lower limb; MoA, migraine without aura; UL, upper limb; f, fasting; ma, massage; mi, mild; mod, moderate; nt, not tried; pr, pressing the affected limbs; se, severe; si, sleep irregularities; sl, sleep; st, stress; su, sun exposure; t, tiredness.
Case 1
A 12-year-old girl had had episodic spontaneous limb pain since the age of 9 years. On average, she had two to three episodes a month. In a typical attack, the limb pain was described as diffuse (within muscle), of a tearing or burning quality, moderate to severe (had to leave school on many occasions), and lasting 2–8 h (occasionally < 30 min). The distribution of pain was variable and could be located in any of the four limbs. The upper limb (UL) (especially arm) was the most common site to be affected. At times more than one limb was involved, including the combination of one arm and contralateral leg. The involvement of two or more limbs usually occurred in a marching fashion (i.e. in a sequence). Most of the times the pain started spontaneously; however, she noted a change of weather (including sun exposure) and stress as precipitating factors for an attack. The use of the affected limbs exacerbated her symptoms. She used to have some relief after tying some cloth around the affected part. She denied the presence of allodynia and localized tenderness in the affected limbs. The patient did not remember any other associated symptoms (such as nausea, vomiting, headache, photophobia, phonophobia, etc.).
The patient had a history of recurrent abdominal pain since the age of 8 years. The character of the abdominal pain fulfilled the International Headache Society (IHS) criteria for abdominal migraine. Its frequency was four to six episodes a year. The patient also had a history of migraine headache without aura (fulfilling the IHS criteria) with a frequency of one episode in a month for 1 year. A few attacks of limb pain were associated with headache and other migraine symptoms. Her mother (case 2) was a migraineur and had a history of RLP. There was no relief of limb pain with any analgesic. The patient had never been treated with any migraine prophylactic agent.
Physical examinations and laboratory tests were normal. The clinical impression was periodic syndrome of childhood linked to migraine. We decided to give propranolol 20 mg twice daily (with the informed, written consent of the parent). In the next 6 months she had only one attack of limb pain. Hence, we planned to stop the drug. However, it was not successful as she had three attacks of limb pain of moderate to severe intensity in the next 3 weeks. Propranolol was restarted in the same dose. During the next 10 months' follow-up, she had one attack of limb pain. In the same period, she had only one episode of abdominal migraine and two attacks of migraine headache.
Case 4
A 19-year-old woman presented with a 1-year history of recurrent spontaneous limb pain, which was perceived as a pressing sensation and poorly localized. It was always located in one limb (usually UL). However, it could be located in any of the four limbs. The pain was not localized to the joint. Attacks were moderate to severe in intensity (interfering with routine activities), increased with physical activity, with one to three attacks per month, lasting for about 2 h to 3 days. The patient denied the presence of cutaneous allodynia. The limb pain was occasionally (in about one-quarter of the attacks) accompanied by headache, nausea, photophobia and phonophobia. The headache was described as unilateral (usually ipsilateral to the limb pain), pulsatile, and mild to moderate (rarely severe). She did not remember any episode of isolated headache (i.e. without associated limb pain). Sleep irregularities, stress, fasting and exposure to sunlight were noted as precipitants for limb pain. Routine activities aggravated her symptoms. However, massage or pressing of the affected limb provided some relief. Her mother was a migraineur. There was marked improvement in her symptoms with paracetamol and ibuprofen if she took the drug at the beginning of her symptoms (usually within 2 h of the onset of limb pain). Physical examinations and laboratory tests were normal. The patient did not have any isolated attack of headache. However, the headache associated with the limb pain fulfilled the IHS criteria of migraine without aura. The patient was given sodium valproate (500 mg b.i.d.) as a preventive measure and sumatriptan 50 mg as prophylactic therapy for moderate to severe attacks of limb pain, after obtaining informed, written consent. After 6 months, she reported three attacks of limb pain and used sumatriptan in one of these three attacks (taken when the limb pain became severe). She did not have any relief with sumatriptan. She used paracetamol (at the beginning of symptoms) in another two episodes and gained complete relief within 60 min. After 6 months' treatment, valproate was gradually withdrawn (over 6 weeks). In the next 3 months' follow-up, she had only one episode of limb pain.
Discussion
Migraine is classically known as a type of primary headache disorder. However, a variety of symptoms may precede, accompany or follow the headache attacks (9). About 20% of migraineurs may experience various symptoms in the absence of any headache. These isolated symptoms are termed ‘acephalgic migraine’, ‘migraine variants’ or ‘migraine equivalents’ (9). There is a suggestion that migraine should be considered as an aetiology in any periodic symptom complex, but the diagnosis should be made only after all other causes have been excluded (9).
Limb pain associated with the attacks of headache has been described by many authors for hundreds of years. However, a temporal relation of limb pain with headache or causal relation of limb pain with headache has been noted only recently (3, 4). There are only a few case reports of RLP in a close temporal relation with headache attacks of migraine (3–7). There is no universally accepted terminology for this condition and it is labelled as ‘migrainous limb pain’ or ‘migrainous corpalgia’ (4, 7). All of our cases fulfilled the IHS criteria of migraine without aura. Three patients reported RLP during childhood. These patients developed migraine headache later on (one during later childhood and another two during adolescence), and a temporal relation of RLP with migraine headache was noted during this period only. The reported prevalence rates of RLP of unknown aetiology (or growing pain) in children range from 2.6 to 33.6% (depending on the method and diagnostic criteria used) (2). About one-third to one-half of children with RLP have a history of headaches and other periodic syndromes (2, 10). However, a temporal relation of limb pain with headache in children is very rare. In review of the literature, we found only two patients with RLP with a temporal relation with headache (3, 5). However, similarities between RLP and migraine in the factors triggering the attacks, associated symptoms during the attacks, relieving factors, the family history of migraine, and the associated recurrent problems suggest a common pathogenesis (2). How many children with RLP will have this symptom in adulthood is unclear, but it is probably not rare. There is a suggestion that as years go on the RLP may convert into different forms of periodic syndromes (especially migraine), but no supporting data are available in the literature (10). The appearance of one symptom frequently coincides with the disappearance or reduced severity of another (6, 10). Saito et al. have reported a familial case series of limb pain in more than 10 individuals in whom limb pain subsided during adolescence, when they began to suffer from typical migraine. However, the headache and limb pain attacks did not show a temporal relation with each other (6). Two of our cases (cases 2 and 6) had a history of RLP in childhood and the onset of headache in adulthood. The frequency of limb pain decreased in adolescence and adulthood. However, it persisted and a few attacks showed a temporal relation with migraine headache.
The age of onset of migraine headache was prior to the onset of RLP in two cases (cases 3 and 5). All the reported case series in the literature have this type of onset (migraine onset followed by RLP) (3, 4, 7). In one of our patients (case 4) RLP and headache started at the same age.
A temporal relation between headache and limb pain is defined as the occurrence of one or more episodes of limb pain in one or more limbs immediately preceding or following the onset of headache, present during it, or shortly after it (3, 5). The limb pain was in a temporal relation with headache in all of our cases in at least a few attacks. The frequency of both isolated limb pain and isolated headache was equally common in four patients. In one patient (case 4), the headache episodes were always associated with limb pain. She did not have a history of isolated headache, although isolated limb pain was common. In contrast to this, case 5 had no attacks of isolated limb pain. Guiloff et al. have reported isolated independent episodes of limb or body pain in 11 patients with headache (also including patients with CH) (3). Piovesan et al. have reported a case of recurrent stabbing and burning pain all over the body in a patient of migraine without a temporal relationship with migraine head pain (8). However, two other case series did not report isolated limb pain in any patients (5, 7) (Table 2).
Main features of patients with recurrent limb pain associated with migraine in the literature
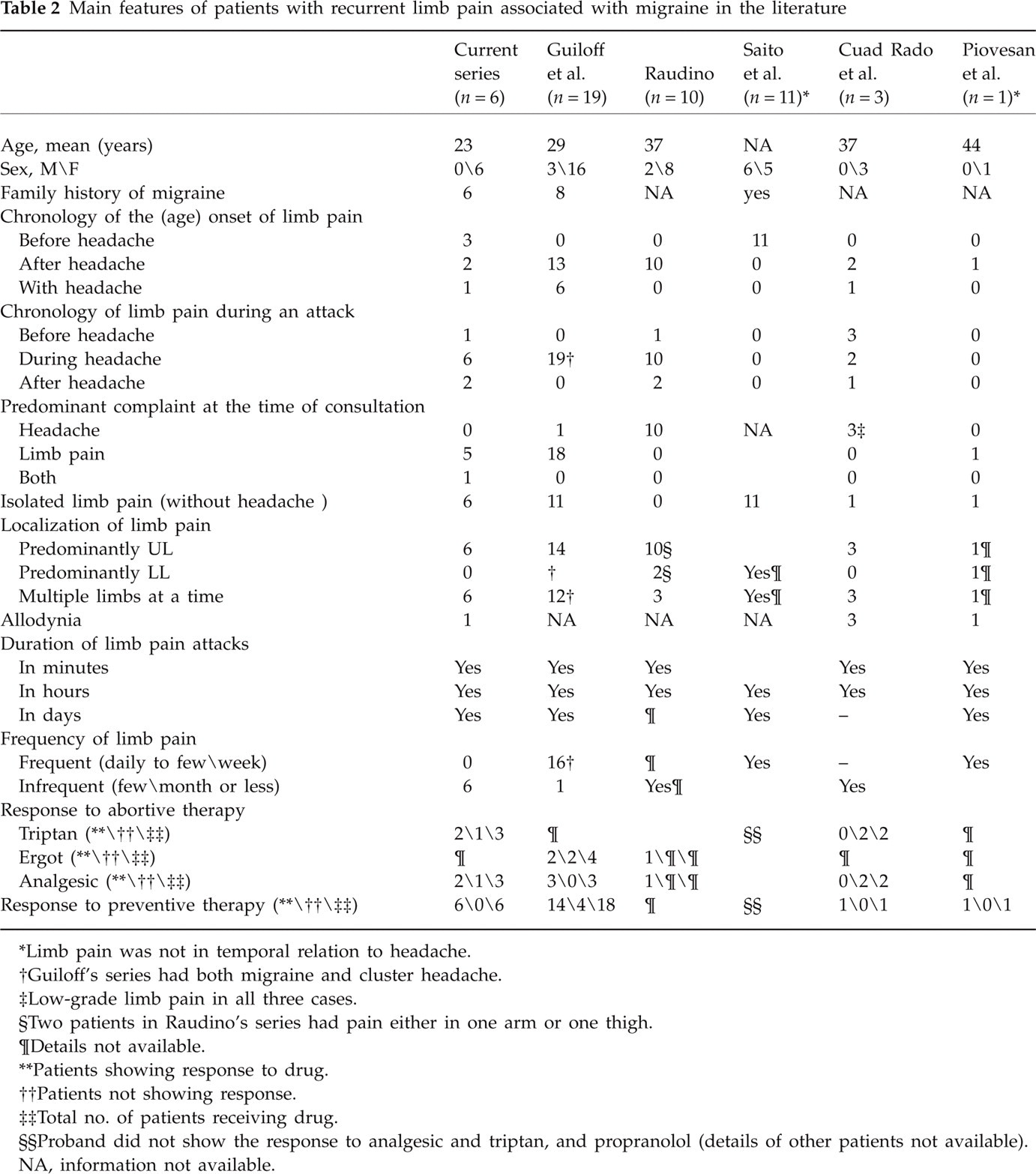
∗Limb pain was not in temporal relation to headache.
†Guiloff's series had both migraine and cluster headache.
‡Low-grade limb pain in all three cases.
§Two patients in Raudino's series had pain either in one arm or one thigh.
¶Details not available.
∗∗Patients showing response to drug.
††Patients not showing response.
‡‡Total no. of patients receiving drug.
§§Proband did not show the response to analgesic and triptan, and propranolol (details of other patients not available).
NA, information not available.
The localization of limb pain was variable. The UL was involved in all six cases. Although involvement of the lower limb (LL) was reported by five patients (only one patient denied it), the overall frequency of UL involvement was much higher than LL involvement. The arm of one side was the most common site to be involved. It was usually ipsilateral to the headache (if headache was one of the accompanying symptoms). Isolated LL involvement (i.e. without UL involvement) was not common. Four patients had a history of involvement of more than one limb at a time, and any type of combination was possible (including one arm with contralateral leg and all four limbs at the same time). Involvement of more than one limb usually occurred in a marching pattern (i.e. in sequence). None of our patients reported pain in the trunk. There are just two case reports in the literature that have trunk pain (with limb pain) in a temporal relation with headache. The UL is the most common site to be involved in this type of patient. In fact, UL was involved in almost all the case reports in the literature where limb pain was in a temporal relation with headache and, in many cases, UL was the only site to be involved (3, 5, 7). This observation is the opposite to RLP of unknown aetiology (or growing pain) of childhood, in which limb pain is usually localized to the LL. Isolated UL pain was a very rare entity even in the many large case series of RLP of unknown aetiology in childhood. Few case series have reported RLP of childhood as a disease exclusive to the lower limbs (2, 10, 11). In the case series of Saito et al. (where limb pain in early childhood was suggested as a precursor of migraine headache), the pain was predominant in the LL. However, none of these patients showed a temporal relation with headache. This observation (LL involvement in RLP of childhood and predominantly UL involvement in patients with limb pain with a temporal relation with headache) may suggest that only a small subset of children with RLP represent an expression of migraine or that the expression of migraine symptoms (including limb pain) may change with subject's age or associated symptoms.
The onset of limb pain in a particular attack used to coincide with the onset of headache (if the headache was the accompanying symptom) in all our cases. It rarely preceded (case 5) or followed (cases 5 and 6) the onset of headache. This observation was similar to the findings of other case series (3, 5, 7).
The limb pain was of tearing, burning or pressing type. No patient reported a pulsatile or throbbing type of pain. However, throbbing, shooting, stabbing, etc., types of pain are well reported in the literature. Triggering factors reported by our patients were sun exposure, change of weather, stress, tiredness, fasting and sleep irregularities. The use of the affected limbs aggravated the symptoms in a few patients. A few of our patients reported some relief by sleep, massaging or tying something around the affected limb.
A usual attack of limb pain would occur for a few hours in all six cases. However, the range was highly variable (a few minutes to 3 days). This finding was consistent with other case series. However, a few cases had limb pain only for a few seconds (3, 8). There are insufficient data in the literature regarding the frequency of episodes of limb pain. The available data range from one a day to one a month (3). The average frequency in our patients was one to three episodes per month. Two of our patients had a history of isolated limb pain for many years in childhood. The frequency of limb pain in these two patients had decreased markedly in adulthood.
The intensity of limb pain is variable in the literature. In the series of Guiloff et al., 20 patients (out of 22, few with CH) had limb or body pain as a main or prominent complaint. No patients had limb pain as the chief complaint in Raudino's series of limb pain and headache (10 patients). In all of our cases, limb pain was a prominent complaint.
One of our patients did not have a history of isolated headache. All other patients claimed that the intensity of headache with the limb pain was less than their usual isolated headaches. This observation was not noted in the previous case series. However, this type of observation is frequent in patients with migrainous vertigo (MV). Patients with MV usually have an attenuated or absent headache with their vertigo compared with their usual migraine headache (12). Our observations (frequent episodes of isolated limb pain and attenuated headache with limb pain) suggest that migraine and limb pain may be related to each other, as are vertigo and migraine. It is possible that a small subset of patients with recurrent unexplained limb pain (with attenuated or no headache) represent an expression of migraine (like patients with MV). There is a need to search for this group of patients. In Raudino's series of limb pain and headache, not a single patient reported spontaneously about the presence of limb pain, which was revealed only in response to a direct leading question (5). The reverse (no spontaneous report of headache during the attacks of limb pain) may also be true. In this type of patient the links (or temporal relation) between migraine and limb pain will be evident only after prospective monitoring of symptoms in a diary. There are many symptoms that may accompany limb pain. Paraesthesia, numbness, cutaneous allodynia, and even weakness have been reported by patients with limb pain with migraine (3, 7, 8).
All six patients were female, consistent with other case series. In fact, we found only five male patients (in the literature) who had limb pain with migraine. Two of our cases (cases 1 and 2—daughter and mother) provide evidence of inheritance. Autosomal dominant inheritance has been suggested in a few case reports (5, 6).
The treatment of limb pain in temporal relation with headache currently parallels that of migrainous headache. A majority of the patients in Guiloff's series (a few of them had associated CH) showed partial to good response to preventive therapy. One patient showed significant relief with preventive therapy in Cuadrado's series. Raudino did not mention the use of any preventive measure in his case series. We advised preventive measures in five cases, which provided a significant reduction in the frequency of limb pain. We did not use any preventive measure in case 2, as she had had very few attacks in the previous few years. However, she reported a decrease in the frequency of limb pain (even of isolated limb pain) with the drugs used for migrainous headache in the past on many occasions.
The preventive measure showed equal efficacy in reducing the frequency of isolated attacks of limb pain in all of our patients. A similar type of response was noted by Piovesan et al. in their case report of a migraineur, where recurrent stabbing and burning pain in the limbs (but not in temporal relation with headache) showed response to propranolol.
Various analgesics and ergotamines were used for acute therapy with variable success in the previous series. There are just a few cases in the literature where sumatriptan was used for limb pain as an abortive therapy. However, it did not provide any effect on the limb pain attacks (6, 7). We used sumatriptan in three patients, all of whom used sumatriptan twice. Two patients noticed a significant effect on the limb pain attacks on both occasions. One patient noted improvement even in the isolated attack of limb pain (i.e. without headache).
RLP is a common disease entity in childhood. Analgesics are frequently used for abortive treatment. However, there is no guideline for preventive measures (especially pharmacological). Our case 1 (a 12-year-old girl) showed marked effects on the frequency of limb pain, headache and abdominal migraine with propranolol.
Mechanisms of migrainous limb pain
It is difficult to speculate on the mechanisms of migrainous limb pain, as current knowledge of the pathophysiology of even classical features of migraine is limited. No anatomical or physiological evidence of convergence of trigeminal and cervical afferents are reported below C4 (in the spinal cord) in the literature. Therefore, the limb pain cannot be explained just by activation of the trigeminovascular system (3, 13). The clinical heterogeneity of patients with migrainous limb pain (our own and in the literature) suggests that various mechanisms are involved. These may be vasospasm, central sensitization, complex regional pain syndromes (CRPSs), ion channel disorders, etc.
Vasospasm of muscular arteries may be the principal mechanism for migrainous limb pain. Vasospasm is associated with classical migraine visual aura (although a causal relation is debatable) (14). Retinal vasospasm is considered to be a primary cause of retinal migraine (15). Vestibular and auditory symptoms of migraine are explained by spasm of cochlear and/or vestibular branches of the internal auditory artery (16). Case–control studies suggest that migraine is associated with arterial wall abnormalities, such as variant angina, cervical artery dissection and Raynaud's phenomenon (17). Endothelin-1, a potent vasoconstrictor, is increased during and between migraine headaches (17). There is a suggestion that migraine might be a more generalized vascular disorder and its clinical features may present outside the headache and the headache phase (18). Tietjen has suggested that migraine is a systemic disorder because of the evidence of systemic endothelial dysfunction and altered reactivity of the systemic vasculature in migraine patients (19). De Marinis et al. described four patients with recurrent neck pain as a variant of migraine (two patients had never had headache). All four had dilation of extracranial arteries and an increase in temperature in the neck and adjoining areas (20). The temperature was higher in the affected limb even in the study by Saito et al. (6). These two observations may suggest a vascular theory for limb pain in a migraineur. Saito et al. have suggested a release of abnormal neurotransmitters at the vascular walls of the extremities as the pathophysiology of limb pain, similar to the trigeminovascular theory of migraine headache (6). Vanmolkot et al. have recently demonstrated decreased diameter and compliance of muscular arteries in migraine patients, and suggested a generalized increase in vascular smooth muscle tone. The arteries of ULs showed more abnormality than those of LLs. The authors further demonstrated the reduced flow-mediated vasodilation of the brachial artery (17). These observations may explain the predominantly UL involvement in patients with migrainous limb pain. The commonest triggering or exacerbating factor of migrainous limb pain is limb use or movement (3). Massage or pressing of the limb is used to provide relief in the some patients. These two observations further support the view of vasospasm or ischaemic pain (21). Heightened haemostasis (procoagulant state) in persons with migraine (because of the elevated von Willebrand factor) may further complicate or initiate the limb pain. Johnson et al. suggest ‘Extremity ischemia secondary to hypercoagulability does not always manifest as critical limb ischemia but may present more subtly as claudication or rest pain’ (22).
Allodynia is one of the common accompanying symptoms of migraine headache. It may be present all over the body. Allodynia is the result of the development of central sensitization (increase in responsiveness) of second-order neurons in the trigeminal nucleus and third-order neurons in the thalamus. Second-order neurons receive information from the face and scalp, third-order neurons from the whole body (23). The involvement of only one limb is the most common presentation in patients with migrainous limb pain. However, more than one limb may be involved simultaneously (usually in a marching pattern). The spreading tendency of pain suggests central origin (probably central sensitization) (24). The central sensitization usually develops during an attack of migrainous headache (because of the activation of the trigeminovascular system). However, central sensitization may be activated directly (without headache phase) by peripheral stimulation (25). Spontaneous body or limb pain has been attributed to central sensitization by a few authors (7, 8). Cutaneous allodynia was present in only one patient in our case series. The two largest case series did not mention the presence of cutaneous allodynia in their patients. The literature is silent regarding the presence of allodynia in RLP of childhood, including a familial case series of limb pain (> 10 patients) that was considered a precursor of migraine. It suggests that central sensitization may not be the sole mechanism of limb pain in migraine patients. The presence of allodynia reduces the responsiveness to triptans. The different responses to acute therapy in patients with limb pain and migraine (in the literature and our case series) further reinforce the idea that central sensitization cannot be the only mechanism for limb pain in patients with migraine (as advocated by a few authors).
Autosomal dominant inheritance, periodic symptoms and episodes triggered by stress or exercise suggest a disease of ion channel disorders (16). Therefore, the possibility of channelopathy cannot be ruled out completely.
Recently, de Mos et al. reported an association of migraine with CRPS (or reflex sympathetic dystrophy) (26). The continuing pain (not recurrent) and the features of involvement of the somato-sensory-sympathetic system (oedema, changes in skin blood flow, etc.) are essential for the diagnosis of CRPS (24, 26). Therefore, CRPS is less likely to be the cause of migrainous limb pain.
In conclusion, RLP in patients with migraine may be a migraine variant or a migraine manifestation. Further investigation (especially on the epidemiology and pathogenesis) in patients with RLP (isolated or with headache) are warranted to establish the interrelations of migraine and RLP.
Footnotes
Competing interests
None to declare.