
Abstract
The aim of this study was to estimate the 1-year prevalence of migraine and the degree of the association of migraine with some sociodemographic characteristics of a representative sample of the adult population of Brazil. This was a cross-sectional, population-based study. Telephone interviews were conducted on 3848 people, aged 18–79 years, randomly selected from the 27 States of Brazil. The estimated 1-year gender- and age-adjusted prevalence of migraine was 15.2%. Migraine was 2.2 times more prevalent in women, 1.5 times more in subjects with > 11 years of education, 1.59 times more in subjects with income of < 5 Brazilian Minimum Wages per month, and 1.43 times more in those who do not do any physical exercise. The overall prevalence of migraine in Brazil is 15.2%. Migraine is significantly more prevalent in women, subjects with higher education, with lower income, and those who do not exercise regularly, independently of their body mass index.
Introduction
Headache is one of the most common complaints by patients. Among its numerous subtypes, migraine is the one that causes a substantial burden on patients' lives and society.
The prevalence of migraine has been estimated in many population-based studies around the world. A recent paper reviewed 107 publications on the epidemiology of headache, including 71 on migraine, from many countries in the five continents (1). In this review, the mean prevalence of migraine in adults was 11% (1), ranging from 1% in Hong Kong (2) to 27.5% in Germany (3). Despite the large number of studies, most were done in specific areas or cities; just a few covered the whole population of a country. They were conducted in Austria (4), Canada (5, 6), England (7), France (8–10), Germany (3), Korea (11), Japan (12), Puerto Rico (13), Sweden (14) and the USA (15–17). Some of these nationwide studies were conducted by personal interview (4, 8, 9), others by mailed questionnaire (3, 10, 15–17), but the majority by telephone interview (5–7, 11–14). In Brazil, which is a very large country with differing cultures and socioeconomic status in its five geographical regions, the prevalence of migraine has been reported only in some cities of the South and Southeast regions (18–22). There has been no previous nationwide study of migraine in our country.
The association of migraine with some sociodemographic factors, such as degree of education, marital status, household income and job status, has been described in some studies, with conflicting results (3, 7, 15–18, 23–30). Migraine prevalence seems not to be associated with obesity (31, 32), although its frequency and severity may increase with body mass index (BMI) (31). The association of migraine with the level of physical activity has been suggested by some authors (33, 34), but to our knowledge the only population-based study to address this issue was Rasmussen's (35), who found no association between low physical activity and migraine.
The objectives of this study were to estimate the 1-year prevalence of migraine and to estimate the degree of association of migraine with some sociodemographic characteristics, including BMI and the frequency of physical activity, in a representative sample of the adult population of Brazil.
Methods
This was an observational, cross-sectional, population-based study. From September 2006 to January 2007 we conducted telephone interviews on 3848 subjects (2307 female and 1541 male), aged 18–79 years, from the 27 States of Brazil, in its five geographical regions, in proportion to the population of each State/region. According to the 2000 Brazilian Census (36), Brazil had 169 799 170 inhabitants (107 042 030 from 18 to 79 years of age).
The sample size was calculated with Epi Info 6.04b software, for an expected migraine prevalence of 20 ± 2%, and a 95% confidence interval (95% CI). We have chosen the 20% expected rate because this is close to the estimated 1-year prevalence in previous Brazilian studies (18, 19, 21). The calculated number of required respondents was 1537. We have added a design effect of 2.5 in order to have sufficient participants, even in less populated States/regions, giving 3843 subjects to be interviewed.
Six trained lay interviewers, at the Execução Contact Centre (Florianopolis, Brazil), a national data-gathering firm, administered the structured questionnaire. From a database of all households with fixed telephones, in each State, telephone calls were made by random digit dial software until the number of responders was reached. Three attempts were made to call any selected telephone number, at different times of the day, before abandoning that number. In Brazil, according to the 2006 National Survey of Households Sample (37), 97.9% of households with an income of ≥ 5 Brazilian Minimum Wages (BMW) have a fixed telephone. In households with an income of < 5 BMW, 76.9% have a fixed telephone in the South, Southeast and Central-West regions, but only 50.2% in the North and Northeast regions. The interview was conducted with whoever answered the telephone, if eligible. An eligible respondent was 18–79 years old, a permanent resident of the household, and mentally capable of answering the questions. Fifty per cent of those contacted agreed to participate. We could not gather any sociodemographic information from those who refused to collaborate. As it was anticipated that more women would answer the phone calls, whenever 60% of the total number of interviews, in each State, were conducted with women, thereafter we would interview only men.
All interviews, including the verbal informed consent, which was read to subjects who agreed to participate, were recorded. Some were reviewed at random by the senior author (L.P.Q.), to ensure that the interviews were of good quality. The questionnaire was not validated, but was based on one previously used in a local study (18) and had been tested satisfactorily in 50 telephone calls with headache subjects. It included questions about the sociodemographic characteristics of the population, as well as questions about headache, based on the second edition of the International Classification of Headache Disorders (ICHD-II) (38). In order to minimize recall bias, the complete interview was done only with subjects who reported headaches within the last year. Migraine was diagnosed when all ICHD-II criteria were fulfilled. We did not differentiate between migraine with aura and migraine without aura, because the interview did not assess aura. The diagnosis of probable migraine was made when all criteria was fulfilled but one. Subjects were told to answer the questions based on their most frequent type of headache, if they had more than one type. Therefore, we gave only one diagnosis for each participant.
Age was divided into six categories: 18–29, 30–39, 40–49, 50–59, 60–69 and 70–79 years. Education level was categorized by years of school: < 8 (elementary), 8–11 (high school) and > 11 (college). Marital status was grouped as single, married, divorced and widowed, and household income by BMW: < 5, 5–9.9 and ≥ 10. Five job conditions were defined: working, retired, unemployed, housewife and student. BMI was calculated based on the subject's self-reported weight and height at the time of the interview and was stratified into three groups: < 25 (normal/underweight), 25–29.9 (overweight) and ≥ 30 (obese). Physical activity was grouped according to the frequency of regular physical exercise, in days per week: none, 1–2 and 3–7.
One-year prevalence rates were calculated, with 95% CI. The overall prevalence was adjusted by gender and age, according to the distribution of the Brazilian population (36). Crude prevalences were weighted, by gender, in the different age groups, according to the percentage of men and women of the Brazilian population in those groups. The overall prevalence was then calculated, weighting prevalences in all ages, according to the distribution of the Brazilian population in each age group. The degree of the association was calculated through prevalence ratios, adjusted with Poisson regression by gender, age, education level, marital status, household income, job status, BMI and physical activity. Statistical Analysis System (SAS, Cary, NC, USA) software was used to analyse the data.
This study was approved by the Ethics Committee on Research of the Hospital Israelita Albert Einstein, São Paulo, Brazil.
Results
A total of 8168 households were contacted, but only in 4075 did the individual who picked up the telephone agree to participate. The response rate was 49.9% (51.9% for women, 46.5% for men). In 227 the survey was not completed; some were excluded because respondents were not eligible, others because they did not complete the interview. Therefore, the questionnaire was filled out in 3848 households.
Table 1 shows the distribution of the survey participants, by gender and age, as well as the geographical regions where they live, and compares it with the Brazilian national population census (36). We interviewed more women (60%) and more subjects aged 18–39 years than the estimated Brazilian population. The mean age was 42.2 ± 14.8 years. Some other sociodemographic characteristics of the respondents are shown in Table 2.
Comparison of demographic characteristics, gender and age, and Brazilian geographic regions among the 3848 respondents with those of the Brazilian census population

∗Source: Instituto Brasileiro de Geografia e Estatística. 2000 Brazilian Census.
Distribution of the respondents, by some sociodemographic characteristics (n = 3848)
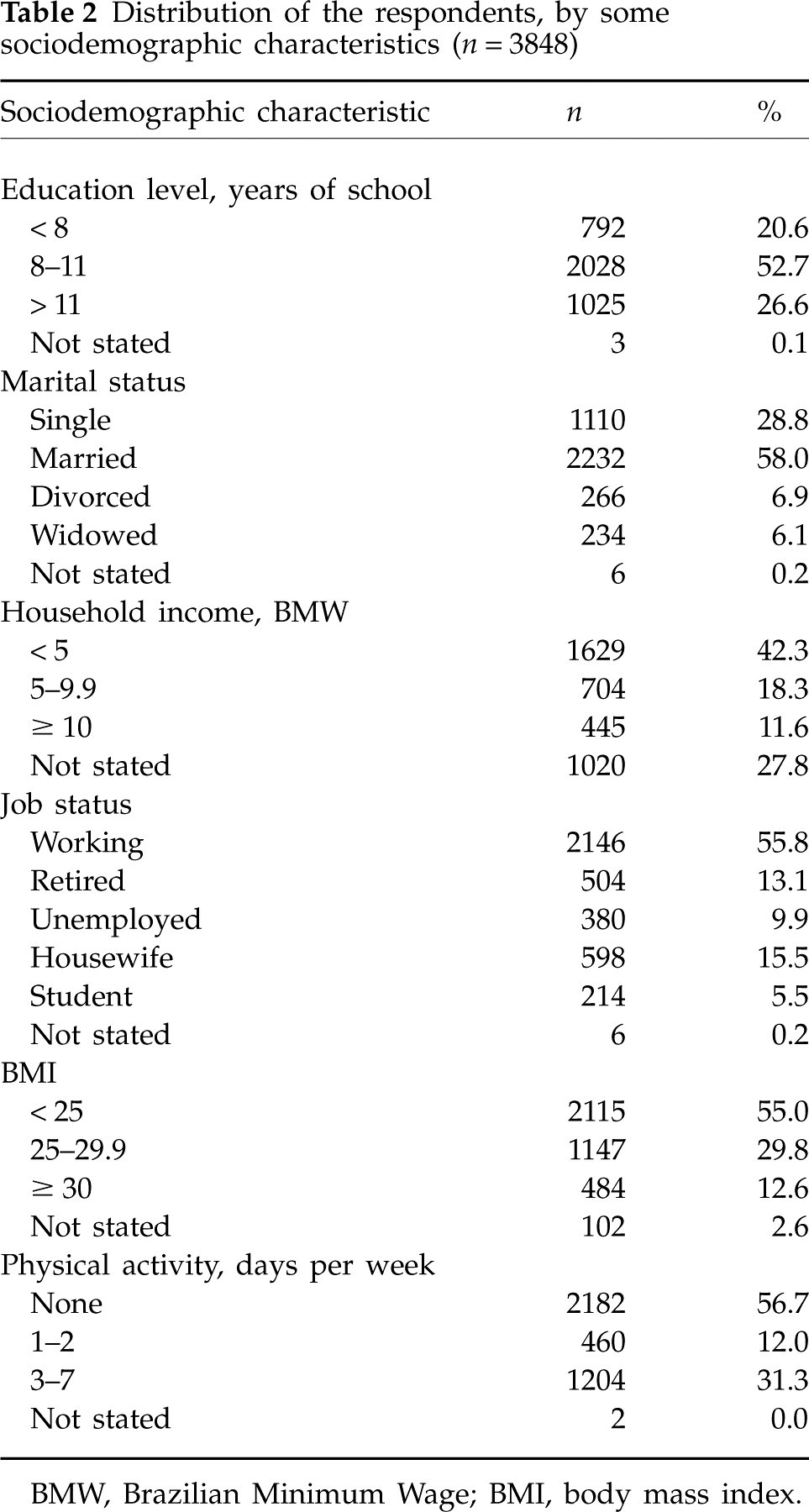
BMW, Brazilian Minimum Wage; BMI, body mass index.
Headache within the last year was reported by 2790 subjects. The estimated 1-year crude and gender- and age-adjusted prevalence of migraine and other types of headache is presented in Table 3. The prevalence of migraine was 20.9% in women and 9.3% in men, with a 2.2 : 1 female/male ratio. Prevalence peaked at the ages 30–39 years, overall (18.1%, gender adjusted) and in women (27.1%), but not in men. It was lowest in those aged 70–79 years, both in women (3.4%) and in men (2.7%) (Fig. 1). Prevalence rates of migraine in the five geographical regions of Brazil were 20.5% (95% CI 18.6, 22.5) in the Southeast, 16.4% (95% CI 13.3, 19.4) in the South, 13.6% (95% CI 11.6, 15.6) in the Northeast, 9.5% (95% CI 6.0, 13.1) in the Central-West and 8.5% (95% CI 5.3, 11.7) in the North.
Estimated 1-year crude and gender- and age-adjusted prevalence of migraine and other types of headache, with 95% CI

∗Adjusted for gender and age.
CI, Confidence interval.

Estimated 1-year prevalence of migraine, by age. Overall (gender-adjusted), women and men.
Table 4 shows the association of migraine with some sociodemographic characteristics of the population, crude and adjusted. Subjects with > 11 years of education reported 1.5 times more migraine than those with < 8 years. Migraine was 1.6 times more prevalent in subjects with a family income of < 5 BMW than in those with a family income of ≥ 10 BMW. Subjects who reported regular physical activity had significantly less migraine than those without any activity, regardless of the number of days per week of regular exertion. There was no significant relationship between migraine prevalence and marital or job status, or with BMI.
Distribution of overall 1-year crude prevalence of migraine, and crude and adjusted prevalence ratios, with 95% CI, by education level, marital status, household income, job status, BMI and physical activity (n = 627)

∗Adjusted for gender, age, education level, marital status, household income, job status, BMI and physical activity.
CI, confidence interval; PR, prevalence ratio; BMW, Brazilian Minimum Wage; BMI, body mass index.
Discussion
This is the first nationwide epidemiological study of migraine in Brazil. We interviewed subjects from its five geographical regions, in all 27 States. As we contacted more women than men, and the proportion of respondents in each age group was different from the Brazilian population, we adjusted the overall prevalence of headache types by gender and age. Although the participation rate was low (50%), Brazilian contact centre experts consider this a very good response rate, because the usual telephone interview participation is 35–40% in our country (personal communication). As the response rate was similar for both men and women, gender headache prevalences were probably not influenced by this. Since headache sufferers may be more likely to respond to a headache survey, this might overestimate headache prevalences. To minimize recall bias, we completed the whole questionnaire only with subjects who reported at least one headache within the last year. Although some patients may have had more than one type of headache, in this study we made just one diagnosis. As we asked subjects to answer the questionnaire based on their most frequent type of headache, rather than their most severe headaches, this might bias towards less severe headaches (tension-type headache). However, because people tend to remember their more severe headaches, this might overestimate the prevalence of migraine.
Because this was a telephone interview survey, many (1070) subjects refused to state their income. However, most (2778) did. We believe the non-respondents may be distributed equally among the three household income categories, because there is no reason why they would be in one specific group. We have shown in a previous article (18) that the answer to this question is reliable, because we have compared the declared income with electricity consumption, and the results were comparable. In Brazil, not all households with an income of < 5 BMW have a fixed telephone. This is particularly true in the North and Northeast regions, where only 50% of households have one. In order to increase the number of participants in this group, we added to the sample number a design effect of 2.5. We chose to make a telephone interview study because it would be too expensive to make a door-to-door survey in such a large country. We believe that we would have had a low response rate in a mailed questionnaire survey, because this is not commonly done in Brazil, and many subjects might not have completed the questionnaire due to illiteracy.
In our study, the estimated 1-year prevalence of migraine was 15.2%. This is lower than the rates previously reported in some Brazilian cities (16.3% in Porto Alegre (22), 22.1% in Florianopolis (18) and 21.4% in Ribeirao Preto (19)), but higher than the 10.7% noted in Pelotas (20) and 12.6% described in Marilia and Sao Paulo (21). The mean migraine prevalence of these four Brazilian studies is 16.6%, which is close to our finding. The different prevalence rates among Brazilian regions may reflect their dissimilar socioeconomic and cultural status. There was a direct relationship between the prevalence of migraine and the degree of development of the region. The 1-year migraine prevalence in other nationwide studies was 10.2% in Austria (4), 14.6% in Canada (5), 14.3% in England (7), 22.3% in Korea (11), 8.4% in Japan (12), 13.5% in Puerto Rico (13), 13.2% in Sweden (14) and 11.7–12.6% in the USA (15–17).
We found a higher prevalence in the age group 30–39 years, especially in women (27.1%). Prevalence rates were much lower after the age of 60 years, in both genders. This type of age-related curve is commonly reported (4–17, 21). Migraine is one of the few medical disorders in which the older patients get, the better their disease becomes. In our sample, migraine was 2.2 times more prevalent in women than in men. This type of female/male ratio is widely supported in the literature (1). We have noted that migraine was 1.5 times more prevalent in subjects with > 11 years than in those with < 8 years of education. A similar finding has also been reported in the USA (24) and in Turkey (26). This relationship was not found by some other authors (3, 7, 18, 23, 25, 27, 30). We have confirmed our previous observation, in Florianopolis, Brazil (18), that migraine was more prevalent in persons with a lower household income. It is 1.59 (1/0.63) times more frequent in subjects with an income of < 5 BMW than in those with ≥ 10 BMW. This inverse relationship has also been demonstrated in the USA (15–17, 24), but not in Europe (7, 23, 29) or in Chile (28). We have no explanation why the association of migraine with household income and education level are in opposite directions. We did not note any significant association of migraine with marital or job status, or with BMI. We have previously reported a higher proportion of migraineurs in divorced or widowed persons (18). Köseoglu et al. (26) described more migraines in married people. Similarly to our finding, job status was not associated with migraine in some publications (23, 26).
Obesity and migraine prevalence were not significantly associated in two studies (31, 32). Bigal et al. (31), however, have described how attack frequency and severity of migraine increased with BMI. We have not looked at these variables. We noted that migraine was significantly less prevalent in subjects who report regular physical activity compared with those who do not exercise regularly: both with 1–2 days of exercise per week (34% less migraine) and with 3–7 days of exercise per week (26% less). If we group these two categories together, migraine was 1.43 (1/0.7) times more frequent in participants without physical activity than in those who exercise at least 1 day per week, independently of the other sociodemographic factors, including BMI. Rasmussen (35) did not find a significant association of migraine with the level of physical activity. Narin et al. (34) have shown that regular long-term aerobic exercise reduced migraine pain severity, frequency and duration, possibly due to increased nitric oxide production. Köseoglu et al. (33) also emphasized the beneficial effect of an aerobic exercise programme on migrainous headache, especially in those with lower basal β-endorphin levels. As we did not study the timing between the start of migraine and the start of physical activity, any inference of causality is precluded. We also do not know if migraineurs do not exercise regularly because of their headaches, or if they have more migraines because they do not exercise.
In conclusion, the overall prevalence of migraine in Brazil is 15.2%. Migraine is significantly more prevalent in women, subjects with higher education, with lower income, and those who do not exercise regularly, independently of their BMI.
Competing interests
None to declare.
Footnotes
Acknowledgements
This study was partly funded by Instituto Israelita de Ensino e Pesquisa do Hospital Israelila Albert Einstein, São Paulo, Brazil, and by Brazilian Headache Society. The authors thank Dr Marcelo Bigal, Dr Nelson Blank and Dr Emil Kupek for their assistance, and Dr Alan Rapoport for reviewing the manuscript.