
Abstract
Medication overuse headache (MOH) is a growing problem worldwide and a challenge for clinicians and investigators. This study aims to contribute to the ongoing debate surrounding the classification of MOH. Applying the revised diagnostic criteria for MOH contained in the updated International Classification of Headache Disorders (ICHD-II), we enrolled 140 probable MOH (p-MOH) patients. They were submitted to an in-patient detoxification protocol and re-examined 2, 6 and 12 months later to confirm, or otherwise, the diagnosis of MOH and to observe the evolution of their headache. MOH diagnosis was confirmed 2 months after detoxification in 71% of patients, who reverted to an episodic headache pattern and stopped their drug overuse The overall clinical situation at 2 months closely reflected the 1-year trend. The 2-month period after drug withdrawal should be retained as a diagnostic criterion in the ICHD-II because it is useful not only as a diagnostic parameter, but also as predictor of a good outcome of 1-year drug withdrawal. In addition, the present findings point to the need for a more objective criterion to quantify headache frequency after drug withdrawal.
Introduction
Medication overuse headache (MOH) presents headache specialists with a number of challenges from various points of view, nosographic, pathophysiological and therapeutic. The estimated prevalence of MOH is about 1–2% in the general population (1), being higher in women (2.6%, rising to 5% in women in their fifth decade of life) and lower in men (0.19%) (2). The prevalence can be as high as 70% in the population of headache sufferers referred to specialist centres (3), and the type of abused medication is changing as new drugs become available (4).
The first International Headache Society (IHS) Classification of Headache Disorders (ICHD-I) included the category ‘Headache induced by chronic substance use or exposure’ (5), defining it as a chronic headache—at least 15 headache days per month during the previous 3 months—that develops following daily use of ergotamine or a specified monthly amount of analgesics, alone or in combination with barbiturates or other non-narcotic compounds, and disappears within 1 month of the withdrawal of the substance. The second IHS classification, The International Classification of Headache Disorders, 2nd edition (ICHD-II) (6), used the term MOH, introducing the new category of triptan-overuse headache defined as headache associated with the intake of this class of drugs on a minimum of 10 days/month for a period of ≥ 3 months. For analgesics, the criterion was intake on 15 days/month, for ≥ 3 months. ICHD-II further differentiated between ergotamine, analgesics, opioids and other drugs. For all the different types of MOH, reversion to the episodic form within 2 months of discontinuation of the overused medication was a diagnostic requirement (criterion D). The lively debate sparked by this new classification has, in the few years since its publication, already led to important revisions of the classification of MOH, with the elimination of the headache characteristics, the introduction of a new subtype (MOH attributed to a combination of acute medications) (7) and the subsequent proposal of appendix criteria for MOH, which no longer require the improvement of headache after withdrawal (8). In particular, the suggestion to eliminate criterion D (‘headache resolves or reverts to its previous pattern within two months after discontinuation …’ of the overused medication) (6) as a diagnostic parameter for MOH has been linked to the fact that patients cannot be diagnosed before drug withdrawal and headache improvement, in other words by the paradox that patients with MOH cannot be diagnosed while they have the headache, but can be diagnosed when they no longer have it.
A meta-analysis of studies on MOH patients has shown that the headache diagnosis at onset is migraine in 65% of patients, tension-type headache (TTH) in 27%, and mixed or other headaches in 8% (9). According to different studies, migraine as the only diagnosis has been related to a better prognosis than a diagnosis of TTH or a mixed diagnosis of migraine and TTH (1).
The pathophysiology of MOH is not known, and several hypotheses are being tested (from a likely role of 5-hydroxytriptamine to a condition analogous to central sensitization) (1).
While treatment strategies are debated (in-patient vs. out-patient, the starting of preventive therapy during or after withdrawal, the usefulness of adopting a replacement therapy), it is generally agreed that abrupt drug withdrawal should be the first therapeutic step. Different approaches to treatment have been proposed, ranging from simple advice to withdrawal of overused drugs (10, 11) to different pharmacological in-patient or out-patient treatments, i.e. oral prednisone (10, 12), naratriptan (10), repetitive intravenous (i.v.) dihydroergotamine injections (13, 14), lidocaine infusion (15), i.v. benzodiazepines and ademetionine (16), mixed pharmacological and behavioural interventions (17), and the so-called headache school (18). To date, standardized guidelines for the treatment of these difficult patients are lacking.
Another aspect to take into consideration in the therapeutic approach to MOH is the problem of relapses. The rate of relapses, which occur mainly during the first year, has been suggested to range from 30 to 45% (17, 19, 20). This aspect needs to be studied further, in order to shed light on the risk factors for relapsing, and on how it might be prevented.
At our headache centre in recent years, we have adopted the CARE protocol (21), a course of in-patient therapy and after-care that, based on the building of a strong doctor–patient alliance, takes into consideration both the medical and the psychological needs of patients.
The aim of our study was to analyse the outcome of a group of 140 patients enrolled in the CARE protocol, comparing the results of the application of different sets of diagnostic criteria. The data obtained provide an evidence-based contribution to the ongoing debate on the classification of MOH.
Methods
The Headache Centre based at the ‘C. Mondino Institute of Neurology’ Foundation (Pavia, Italy) is a tertiary referral headache centre. We evaluated, in a prospective, non-randomized way, consecutive patients seen for the first time at the centre between May 2004 and January 2006 and who fulfilled revised ICHD-II criteria (7) for probable MOH (p-MOH). After giving their verbal informed consent to participate, patients were enrolled in the CARE I protocol (21). This consisted of a 2-month observational period during which the patients, awaiting hospitalization, monitored characteristics of headache and drug intake by means of an ad hoc diary (22). We considered this phase as a picture of p-MOH in each patient and utilized the diary data to determine headache frequency and to calculate the amount of drug intake before in-patient withdrawal. Subsequently, the patients underwent detoxification as in-patients and then, over the next year, attended three follow-up visits (at 2, 6 and 12 months) (Fig. 1).
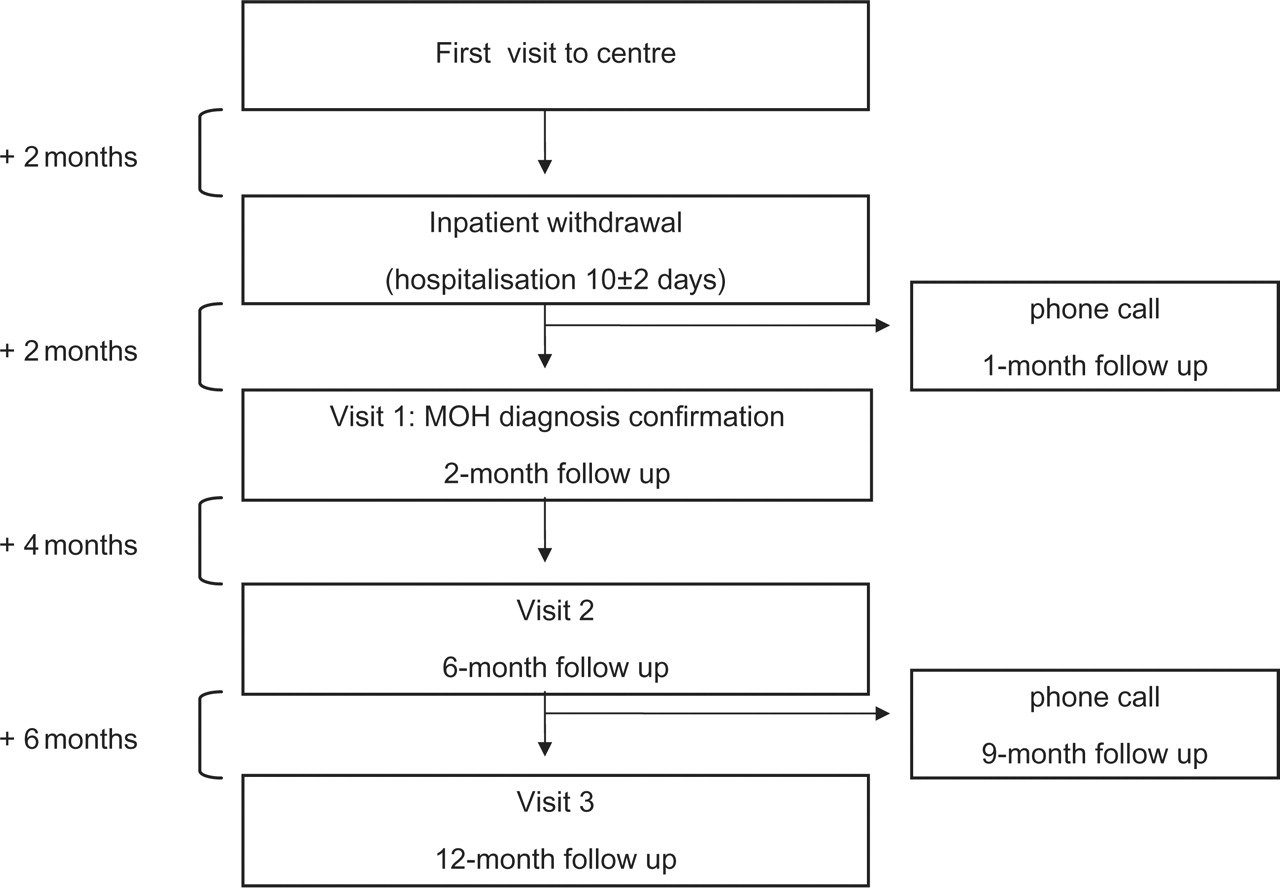
Study design of CARE I protocol.
Patients were instructed to keep up filling in the ad hoc diary adopted during the observational period also during hospitalization and the entire follow-up time. One hundred and forty patients (27 male, 113 female) with a mean age of 44.5 ± 11.4 years (range 21–73 years) and a diagnosis of p-MOH according to revised ICHD-II criteria for this condition (7) were included in the study.
On day 4 or 5, a preventive treatment was started, personalized according to the presence of comorbidities and the previous prophylactic therapy used by the patient. During hospitalization, each subject was allowed to use a rescue medication (100 mg of intramuscular ketoprophen) only in case of severe rebound headache. Upon discharge, we prescribed a symptomatic drug of a different category from that overused, instructing the patient to utilize it only for severe attacks and for no more than 5 days a month. Generally, we chose simple analgesics and triptans.
All the participants were assessed by the same neurologist (a headache specialist), using an ad hoc data sheet, which also made provision for the collection of a comprehensive personal and family history, with particular attention paid to headache history and the profile of drugs used. The same neurologist personally cared for each patient throughout the follow-up year after the in-patient treatment, monitoring the clinical situation through three scheduled visits (2, 6 and 12 months’ follow-up) and two phone calls (1 and 9 months’ follow-up). The psychological evaluation of the patients consisted of a general standard interview and a Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders-IV Axis I Disorders (Structured Clinical Interview for DSM -I) (23). During their hospital stay, all patients received educational and rehabilitative counselling, including instructions for the post-discharge period. On discharge, patients were asked to continue to fill in their headache diaries, scheduling follow-up visits. The patients were told that they could contact the neurologist as often as they felt necessary.
At the 2-, 6- and 12-month follow-up visits, the pattern of the headache was evaluated, recording, on the basis of the information contained in the patient's diary, the number of days with headache and the use of symptomatic drugs. Prophylactic therapy was generally maintained unchanged for the first 6 months, after which we tried to reduce the dose of the prophylactic drug or, in the case of multiple drugs, to simplify the treatment regimen.
For statistical reasons, we identified a subcategory of ‘polyabusers’, defined as patients with overuse of more than one class of symptomatic drug and meeting more than one of the ICHD-II criteria from 8.2.1 to 8.2.5 (relating to different subtypes of MOH).
In accordance with the aim of our study—to analyse the applicability of revised ICHD-II diagnostic criteria (7) as well as the appendix criteria proposed more recently (8)—we collected data in order to compare the groups with or without headache improvement following withdrawal. On the basis of the revised ICHD-II criteria for MOH, at the 2-month follow-up, patients who had reverted to an episodic pattern of headache and who no longer overused symptomatic drugs were labelled ‘true’ MOH, whereas the label p-MOH was applied to those who, after withdrawal, still suffered from chronic headache but had not reverted to symptomatic overuse (‘medication overuse has ceased within the last two months but headache has not so far resolved or reverted to its previous pattern’—8.2.8, criterion C, point 2), and also to those with chronic headache still overusing symptomatic medications (‘overuse medication has not yet been withdrawn’—8.2.8, criterion C, point 1) (7).
In addition to the qualitative criterion specified in ICHD-II (‘headache resolves or reverts to its previous pattern within two months after discontinuation’), the patients were also analysed according to a quantitative criterion, namely a ≥ 50% reduction of monthly headache frequency after 2 months.
At the 6-month and 12-month follow-up, patients presenting with a reversion to a chronic pattern of a headache that had previously (i.e. at the 2-month follow-up) become episodic, associated with overuse of drugs for ≥ 3 months, were defined as relapsers, as were those presenting with persistent chronic headache after withdrawal (p-MOH), again associated with a relapse into overuse.
The Statistical Package for the Social Sciences (
Results
Patient population
According to the revised ICHD-II criteria for MOH (7), all the 140 patients were classifiable as p-MOH, whereas all could be diagnosed as MOH according to the appendix criteria (8).
The mean duration of chronic headache was 5.8 years (range 3 months to 33 years) and the mean duration of symptomatic drug overuse was 4.8 years (range 3 months to 28 years). On the basis of the data contained in the headache diaries filled in 2 months before hospitalization (observational period), we recorded means of 23 headache days (range 15–30), 22 days of symptomatic drug intake (range 10–30) and 43 doses taken monthly (range 10–220). Four patients (3%) overused ergotamine (8.2.1), 37 (26%) overused triptans (8.2.2), 35 (25%) overused analgesics (8.2.3), five (4%) overused opioids (8.2.4), 38 (27%) overused combination medications (8.2.5) and 21 (15%) overused more than one of the above categories (and were thus considered ‘polyabusers’).
As regards the prescription of preventive therapy, three patients (2%) were discharged without, whereas 137 (98%) used one or two prophylactic drugs (52 in monotherapy and 85 in polytherapy). The prophylactic regimen was prescribed taking into account the patient's history and comorbidities, using common preventive agents (calcium antagonists, β-blockers, tricyclic antidepressants with or without neuroleptics, other antidepressants, antiepilectic drugs).
Follow-up data
Complete datasets were available for 130 patients (93%) 2 months after withdrawal, for 126 patients (90%) 6 months after withdrawal and for 114 patients (81%) 12 months after withdrawal (Fig. 2).
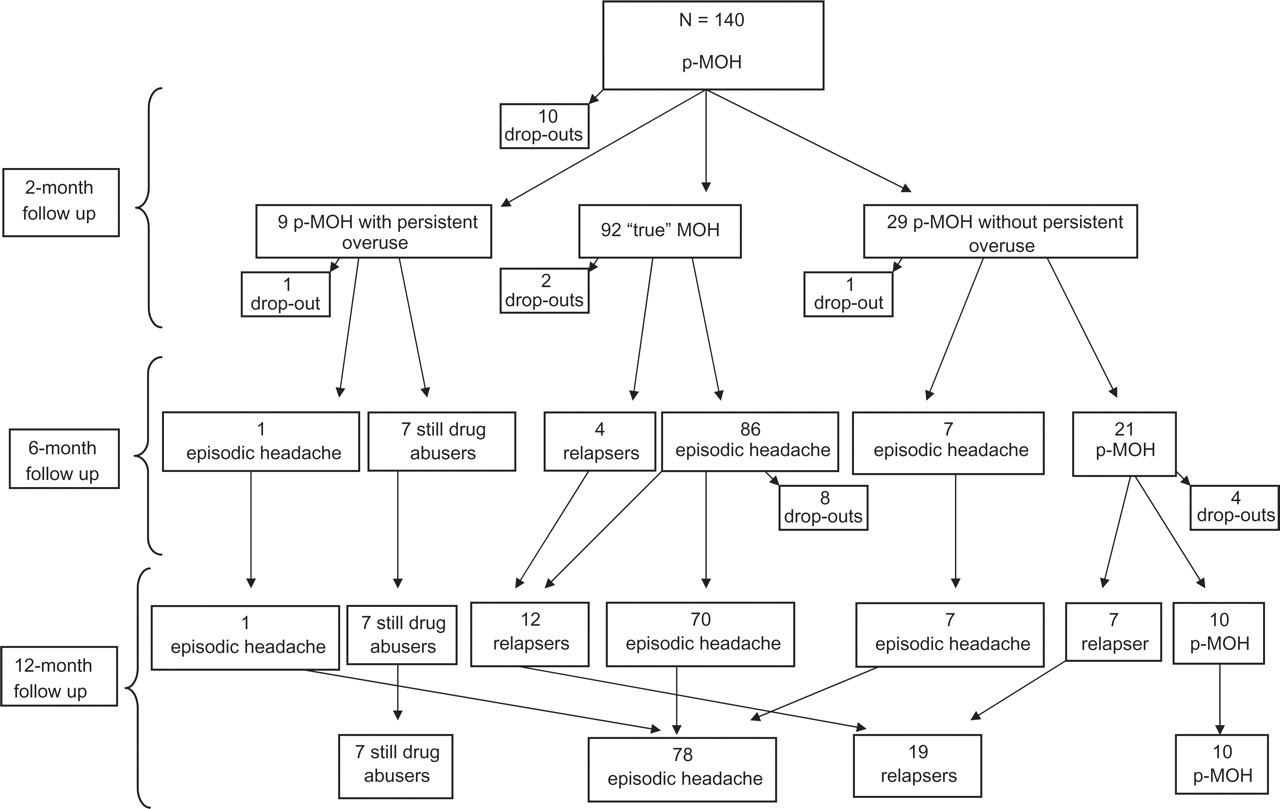
Pattern of probable medication overuse headache at 2-, 6-, 12-month follow-up.
No significant differences in demographic and clinical history were found between the patients included in the analysis and those lost to follow-up.
Description of the sample at 2-month follow-up
One hundred and thirty patients (93%) (26 male, 104 female; mean age 44.8 ± 11.6 years, range 21–73 years) returned to the centre for the follow-up evaluation at 2 months (Fig. 2). MOH diagnosis was confirmed in 92 patients (71%), who had reverted to an episodic headache pattern and stopped their drug overuse (group 1: ‘true’ MOH). Headache was still present in a chronic form in 38 patients (29%): in 29 of these (22%) the headache persisted despite their discontinuation of the overused drug (group 2: p-MOH without persistent overuse), whereas the remaining nine subjects (7%) had never stopped their overuse of symptomatic drugs (group 3: p-MOH with persistent overuse). We re-evaluated the headache history of each of the patients in groups 2 and 3 in accordance with the criteria set out in ICHD-II, but did not find any other possible causative factor for their headache.
When we applied the proposed quantitative criterion (≥ 50% reduction of headache frequency), true MOH was diagnosed in 57% (vs. 71% with qualitative criterion, χ2 = 5.40; d.f. = 1; P = 0.020) (Table 1).
Medication overuse headache (MOH) diagnosis at 2-month follow-up according to the International Classification of Headache Disorders (ICHD)-II qualitative criterion (‘headache resolves or reverts to its previous pattern’) and to the alternative quantitative criterion (reduction of headache frequency ≥ 50%) in 130 patients
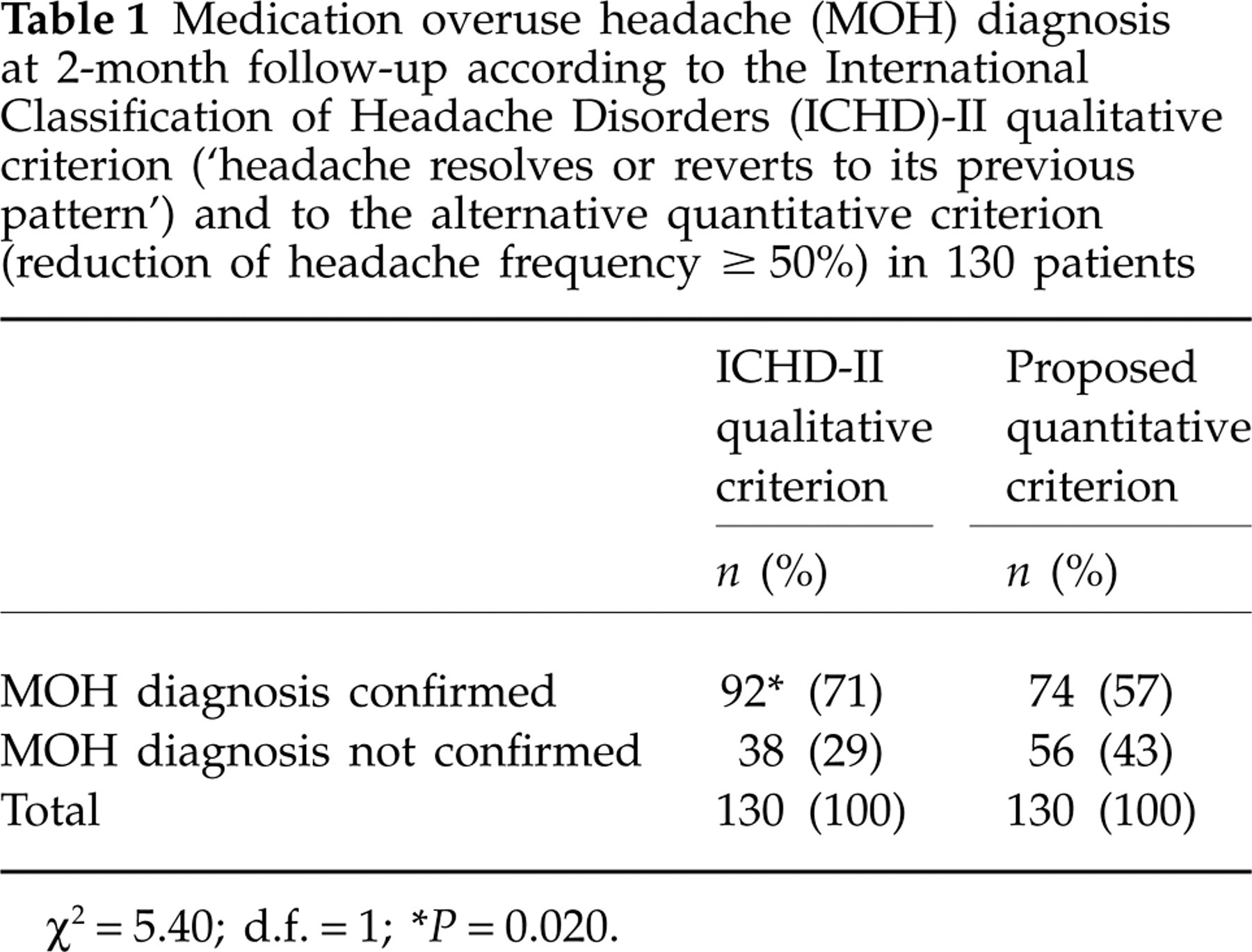
χ2 = 5.40; d.f. = 1;
∗ P = 0.020.
According to the appendix criteria, MOH could be diagnosed at this time point only in the nine subjects (7%) who were still overusing symptomatic drugs, whereas of the remaining 29 subjects still suffering from chronic headache but no longer overusing drugs, 11 were diagnosed with chronic migraine and 18 with mixed migraine and chronic/episodic TTH. In the 92 subjects who had reverted to an episodic pattern the diagnosis was migraine in 74 cases, and mixed migraine and TTH in the other 18.
When comparing the groups identified adopting the different (qualitative/quantitative) criteria, we found that migraine as the initial headache was statistically more frequent in subjects with a confirmed MOH diagnosis (χ2 = 16.32, d.f. = 1, P < 0.0001 for the qualitative criterion; χ2 = 12.64, d.f. = 1, P < 0.001 for the quantitative criterion) (Table 2). Instead, the association migraine + TTH was nearly equally distributed among the treatment non-responders.
Primary headache diagnoses and 2-month outcome

Comparison between ICDH-II qualitative criterion (χ2 = 16.32; d.f. = 1;
∗ P < 0.0001
) and the proposed quantitative criterion (χ2 = 12.64; d.f. = 1;
∗∗ P < 0.001).
M, migraine; TTH, tension-type headache.
Table 3 shows the entity of reduction of headache frequency (≥ or < 50%) in the three groups of patients identified using the qualitative criterion: 72% of the ‘true MOH’ patients (group 1) had a reduction of headache frequency ≥ 50% vs. 24% of the p-MOH patients without persistent overuse (group 2) and 11% of p-MOH patients with persistent overuse (group 3).
Reduction of headache frequency (headache days/months), days of intake/months and symptomatic drug doses taken by < or ≥ 50% in the three groups of patients identified applying the qualitative criterion

Analysing the reduction of drug intake (days of intake/month and doses/month) in the same groups (Table 3), we found that the persistent overusers (group 3) showed a considerable reduction of their drug intake, particularly in terms of the number of doses taken: in 56% of these patients this reduction was ≥ 50%.
When the median reduction of drug intake was analysed in terms of days of intake/month and doses/month, statistically significant differences emerged between the three groups: the ‘true’ MOH patients (group 1) showed a significantly greater median reduction of drug intake compared with groups 2 and 3 (Kruskal–Wallis test; P < 0.001 for reduction of days of drug intake and P < 0.01 for reduction in number of doses taken) (Fig. 3).

Reduction of days with drug intake and reduction in number of doses taken in the three diagnostic groups according International Classification of Headache Disorders-II qualitative diagnostic criteria: group 1—true MOH (▪); group 2—p-MOH without persistent overuse (▒); group 3—p-MOH with persistent overuse (□). Data are expressed as percentage change from observational period (data from headache diaries filled in 2 months before hospitalization). Median values are shown. (Kruskal–Wallis test; ∗P < 0.001 for reduction of days of drug intake; ∗∗P < 0.01 for reduction in number of doses taken.)
No statistically significant differences emerged between the groups at the 2-month follow-up when considering the different drugs abused (Table 4), although 100% of ergotamine abusers and 78% of triptan and analgesic overusers were found to revert to an episodic pattern of headache after 2 months, whereas the percentage tended to be lower among the polyabusers (59%).
Profile of drug overuse at 2-month follow-up (P = NS)

Group 1, true MOH; group 2, probable-MOH without persistent overuse; group 3, 8.2.1: ergotamine-overuse headache; 8.2.2: triptan-overuse headache; 8.2.3: analgesic-overuse headache; 8.2.4: opioid-overuse headache; 8.2.5: combination medication-overuse headache. ‘Polyabusers’, patients overusing more than one of the above classes of drug, i.e. fulfilling the ICHD-II criteria (from 8.2.1 to 8.2.5) for more than MOH subtype.
Description of the sample at 6 months and 1 year
Six months after the detoxification therapy, no significant changes were found compared with the situation at 2 months (see Fig. 1). Only 4.4% of patients diagnosed with true MOH at 2 months relapsed (4/90), whereas 25% of those presenting p-MOH without persistent overuse (group 2) reverted to an episodic headache pattern (7/28). Of the persistent abusers (group 3), only 1/8 showed an improvement. Of the whole initial sample (n = 140), 26 (18.6%) patients dropped out, whereas 114 completed the 1-year post-detoxification follow-up afterwards. Of these, 36 (31.6%) continued to have chronic headache: seven (19.4%) were non-responders (subjects who had persisted in their drug overuse from the initial evaluation), 10 (8.7%) could still be defined as p-MOH and 19 (16.7%) were relapsers. This means that 68.4% (n = 78) of the initial sample had reverted to episodic headache after 1 year (Fig. 2).
We found a higher prevalence of episodic headache at the 6-month follow-up (96/126; 74.6%) compared with the assessments at 2 months (92/130; 70.8%; χ2 = 0.98; P = 0.84; d.f. = 1) and at 1 year (78/114; 68.4%; χ2 = 0.39; P = 0.65; d.f. = 1), even if not statistically significant.
Among the patients with a confirmed diagnosis of MOH (group 1), we found a drop-out rate of 11% at 1-year follow-up, whereas 82 (82/92, 89%) patients were available for evaluation. Only 12 patients (14.6%) had relapsed, whereas the remaining 70 (85.4%) continued to show an episodic pattern.
Analysing the 29 patients with p-MOH without persistent overuse (group 2) at 1 year, we found a drop-out rate of 17.2%, whereas seven (24.1%) had relapsed into overuse, seven (24.1%) had an episodic pattern of headache, and 10 subjects (34.5%) still had a diagnosis of p-MOH without enduring overuse.
Among the nine patients with p-MOH with persistent overuse (group 3), we found a drop-out rate of 11.1% at 1 year, whereas the diagnosis was unchanged in the other 88.9%.
It is noteworthy that the patients who could be classed as persistent abusers or relapsers at 1 year were more likely to belong to the groups not responding to detoxification at 2 months than to the group of responders ('true’ MOH patients) (χ2 = 29.51; d.f. = 1; P < 0.0001) at that time point, strongly confirming the diagnostic importance of the ICHD-II 2-month criterion.
We classified patients’ headaches at 1 year in accordance with the ICHD-II criteria: 61 (53.5%) had migraine, 18 (15.8%) a mixed picture of migraine and episodic TTH, four (3.5%) migraine and chronic TTH, five (4.4%) chronic migraine and 26 (22.8%) still had a diagnosis of p-MOH.
Prophylactic therapy was, in all cases, prescribed on the basis of the patient's personal history and comorbidities, without significant differences emerging between the groups in this regard. The duration of the medication overuse did not appear to influence the trend of the headache over time.
Description of patients lost to follow-up
Of the whole initial sample, 26 (18.6%) patients (five men, 21 women; mean age 40.8 ± 8.3 years) dropped out of the study: 10 at 2 months, four at 6 months and 12 at 1 year. We were able to contact 22 of them (84.6%): 14 did not relapse into abuse, eight did. Six of them said that they themselves had decided not to return to the centre, while 16 failed to comply with the protocol.
Discussion
Many factors are related to MOH and may influence the progression from drug use to drug abuse, from headache to rebound headache. The diagnosis of MOH is clinically important because patients ‘rarely respond to preventative medication whilst overusing acute medications’ (6) and, in the context of the ongoing debate, new appendix criteria (8) have been suggested in order to test proposed revisions to the current diagnostic criteria for MOH (6, 7). The paradoxical situations whereby MOH patients cannot be diagnosed until their overuse has been discontinued, and some patients who did not improve after drug withdrawal then became responsive to prophylaxis (24), have led to the suggestion that criterion D (‘Headache resolves or reverts to its previous pattern after two months of discontinuation of …’ the offending drug) (6) should be removed from the main body of the classification on the grounds that it is too restrictive. Instead, our data—the majority of our patients (70.8%) fulfilled criterion D 2 months after withdrawal—seem to dispute this. Our data suggest that the main issue, rather, is that of the non-responding patients: what is their diagnosis? Why did they fail to respond to withdrawal within a 2-month period? It also noteworthy that a small percentage of patients not responding after 2 months were found to be responders 4 months later (6%); however, only one (0.71%) of the patients who did not respond at 2 months did so at 1 year.
Some studies (10, 25, 26) have used an objective, quantitative criterion (≥ 50% reduction of frequency of the headache attacks) to diagnose MOH 2 months after symptomatic drug withdrawal. The ICHD-II (6, 7) provides the subjective, qualitative criterion ‘Headache resolves or reverts to its previous pattern’. However, many patients can find it very difficult to recall the ‘previous pattern’ of their headache, especially if their MOH is a problem they have lived with for many years. Equally, any recollection of the ‘previous pattern’ is not guaranteed to be accurate. For these reasons, we suggest changing ‘previous’ into ‘episodic’ pattern (corresponding to < 15 days/month). This is justified by the fact that, in our study, the diagnostic criterion ‘≥ 50% reduction of frequency’ excluded a sizeable group of patients who showed the said reduction of frequency, yet remained within the chronic headache range (headache on > 15 days/month). However, it is also worth stressing that the remaining 30% of our sample, while not officially classifiable as MOH, nevertheless showed a reduction of headache frequency and, in particular, a reduction of doses/month. The quantitative and qualitative criteria both present weaknesses: the quantitative criterion risks incorrectly classifying as ‘true’ MOH patients still affected by chronic headache (24% in our sample); the qualitative one, on the other hand, is subject to distortions of memory, and too prone to subjective interpretation. Studies have implicitly recognized and addressed this limitation of the official classification by using more objective criteria, but standardization of this important aspect is critical in order to ensure comparability of studies, which is currently lacking.
Other issues worth debating are the definition of patients with p-MOH as a first diagnosis (‘overused medication has not yet been withdrawn’) as opposed to a second diagnosis (‘medication overuse has ceased within the last two months but headache has not so far resolved or reverted to its previous pattern’), and the situation of patients failing to respond to withdrawal of medication and, even more so, of those who are not able to withdraw the offending medication and continue to be chronic headache sufferers. In other words, a distinction needs to be drawn among the non-responders: in our study, a small group of patients (n = 9; 6.4%) did not respond at all (neither withdrawing the offending drug(s) nor showing any improvement of their headache), thereby maintaining a diagnosis of p-MOH (in accordance with criterion B, point 1 of ICHD-II code 8.2.7 Probable medication-overuse headache) (6); another group (n = 29; 22.3%) withdrew the offending medication, but without showing any improvement in headache frequency, thereby maintaining the diagnosis of probable MOH (in accordance with criterion B, point 1 of ICHD-II code 8.2.7) (6). In short, the ICHD-II allows diagnosis of p-MOH in two very different clinical situations, which have different aetiological mechanisms and probably require different therapeutic strategies. From a clinical point of view, both groups present a therapeutic challenge, the former representing the really difficult nut to crack (these patients are not able to discontinue the abused medication), and the latter promoting debate on the reasons why the headache pattern may fail to change after drug withdrawal and in-patient detoxification.
It is noteworthy that most of the patients who were relapsers or whose situation was unchanged at the 1-year follow-up came from the group who were non-responders after 2 months. This means that the 2-month outcome is important not only for classification purposes, but also as a prognostic factor. From another point of view, new research data on MOH might be drawn from the study of these difficult patients. In the study by Zeeberg et al. (24), 35.9% of the initial sample (121/337) was excluded because the patients failed to stay medication-free; of the study group, 48% were unchanged and 7% worsened, whereas 45% improved with mere discontinuation of the offending drug (25). In the study by Bigal et al. (27), 30.3% of patients were relapsers after 1 year. In our sample, 31.6% of patients had chronic headache 1 year drug-free, albeit presenting different clinical pictures (chronic abuse and chronic headache, relapse into abuse and chronic headache, or complete withdrawal of abused medication and chronic headache). It is to be stressed that we do not know why > 30% of the patients had failed to improve or had relapsed at 1 year, but these patients demand the attention of clinicians and researchers. They might represent a specific diagnostic entity, with specific medical and/or psychological needs, which should be a new focus for research.
It is worth noting that almost 70% of patients showed benefits of detoxification and preventive medication over a period of 12 months, a figure very similar to the 73% reported by Bigal et al. (27), and higher than that reported in a study in which mere discontinuation of the offending drug was adopted (45% in a 2-month period) (25). It indirectly supports the efficacy of detoxification in the treatment of MOH, as suggested by Bigal et al. (28). Other studies (10, 11) have outlined the good efficacy of advice to withdraw the overused drug as the only intervention, at least in a subgroup of patients with migraine (or chronic migraine), low medical needs and no psychiatric comorbidity (11). The existence of two different MOH sub-types has been suggested (29). As regards the headache subtypes, we did not record any cases of ‘pure’ chronic TTH as the initial headache, whereas chronic migraine was very rare and diagnosed only in the year after detoxification. The debate on chronic migraine has been ongoing for a long time (30) and there is urgent need for revision of the relevant diagnostic criteria (8).
In our study, the 1-year relapse rate was 16.7%, lower than the 41% reported by Katsarava et al. (19), who pointed out that the first year after withdrawal is associated with the highest risk of relapse (94% of their patients relapsed within the first year of withdrawal). Other studies have reported relapse rates of 22–44% during the first year of follow-up (31–35). However, different studies are not always comparable because of their use of different headache classification systems, different therapeutic choices (in withdrawal, detoxification and prophylaxis) and different criteria for evaluating improvement. Therefore, the question remains, what is the best way to manage these difficult patients? The very low relapse rate we found after 1 year strongly supports our strategy of care. However, it has to be stressed that the study design was not built to give evidence of the treatment efficacy of the ‘CARE’ protocol, even if studies are ongoing to support our plan of therapy for MOH patients. To date, we do not know whether much of therapy efficacy is related to drugs or to the strong doctor–patient alliance or placebo effect.
In summary, the 2-month period after drug withdrawal should be retained as a diagnostic criterion in the ICHD-II because it is useful not only as a diagnostic parameter, but also as predictor of a good outcome of 1-year drug withdrawal. Second, we highlight the presence of a significant proportion of ‘refractory’ (or intractable) patients who should be better studied, because they may have different MOH characteristics, or not even have MOH at all. The current classification is not able to distinguish and adequately ‘label’ this group of patients. A third point to underline is the need for a more objective criterion to detect headache frequency after drug withdrawal, as this would ensure comparability of different studies and differentiate patients according to their pre-withdrawal situations.
Finally, in-patient detoxification is useful, but in the context of a global approach that takes into account both the medical and the psychological needs of MOH patients, and in which educational strategies and long-term counselling help to strengthen the doctor–patient relationship, thereby reducing the occurrence of relapses.
Footnotes
Acknowledgements
This study was supported by a grant from the Italian Ministry of Health (RC2004-2006) and by the Eurohead project (LSHM-CT-2004-504837). The authors gratefully thank Dr Cristiana Rezzani, Department of Applied Health Science, University of Pavia, for her support in the statistical analysis of the data.