
Abstract
The aim of this study was to identify and diagnose headache in a temporomandibular joint and orofacial pain clinic population using the second edition of The International Classification of Headache Disorder criteria. In 502 temporomandibular disorder and orofacial pain patients, 246 patients (49%) were diagnosed with tension-type headache (TTH), followed by migraine without aura (14.5%), probable migraine (12.9%), migraine with aura (7%), probable TTH (4.8%) and cluster headache (0.2%). The prevalence of headaches was compared between male and female patients, and the prevalence of migraine was found to be higher in women than in men. In evaluating by age, the prevalence of migraine was highest in patients in their 20s and 30s and declined as age increased above 40. TTH showed the highest rate throughout all age groups, but it also decreased as age increased. In this study, the prevalence of migraine was lower than that reported in Dr Kim et al.'s study, and the prevalence of TTH much higher than that reported in the previous study. Of the headache patients, 81.1% presented with masseter muscle pain and 47.8% with temporal muscle pain. This finding suggests that pericranial muscle pain may be an inducing factor of primary headache.
Introduction
Headache, one of the most common complaints of patients that present in all practices of medicine, constitutes a large public health problem impacting both the individual sufferer and society (1). The results of ongoing epidemiological studies of headache vary according to age, sex and race (2). Recently the International Headache Society (IHS) developed and adopted the second edition of The International Classification of Headache Disorders (ICHD-II) criteria in order to clarify the diagnosis of head, face and neck pain. These criteria have become the diagnostic standard for headache studies (3,4). The system lists 14 categories of headache. The first four categories represent the primary headaches, while the remaining 10 contain secondary headaches such as neuropathic pain and disorders of teeth, jaws and cervical structures (4).
Temporomandibular disorders (TMD), which are common in the general population, are associated with pain and dysfunction in the temporomandibular joint (TMJ) and associated muscles. The pain is often exacerbated or triggered by jaw function such as chewing or talking, and may be associated with limited or asymmetric jaw movements as well as joint noise with movement or locking upon opening the mouth (5).
There has been controversy over the association between TMD and headache. There has been a report that the overall prevalence of headache in TMD and orofacial pain patients is 70.6% (6) and that TMD may also be associated with symptoms such as otalgia and cervical pain (7). Recently Ballegaard et al. reported that the prevalence of TMD in the headache population was 56.1% and a high proportion of headache patients had significant disability because of ongoing chronic TMD pain (8). In contrast, a study conducted on an adolescent population (13–16-year-old subjects) reported that TMD and headache had no significant association. The authors commented that the lack of association between headache and TMD signs could reflect the difficulty in applying IHS criteria (which are suitable for adults) to children's headache (9).
The aim of this study was to identify and diagnose headache in a TMJ and orofacial pain clinic population using ICHD-II criteria.
Patients and methods
Study population
The study population consisted of men and women who presented for the management of TMD and orofacial pain in the TMJ and Orofacial Pain Clinic (Department of Oral Medicine, College of Dentistry, Yonsei University, Seoul, Korea). For inclusion, subjects had to have had two or more headaches in the previous 3 months.
Clinical examination
A headache specialist examined the patients and made the clinical diagnosis of headache based on the ICHD-II. The clinical examination of TMD and orofacial pain patients consisted of personal identification (name, age, sex), evaluation of the chief complaints, a review of the history of the present complaints, systemic disease or trauma, and evaluation of any habits or drug abuse. In addition, the TMJ, masticatory and pericranial muscles were palpated for tenderness and range of mandibular movement.
Statistical analysis
Analysis of data was performed using
Results
Demographic characteristics
A total of 502 patients participated. There were 391 women (77.9%) and 111 men (22.1%). The mean age was 30.4 ± 12.1 years (28.9 ± 12.6 for men, 30.8 ± 11.9 for women).
Clinical diagnosis of TMD and orofacial pain patients with headache
The clinical diagnosis of temporomandibular disorder and orofacial pain patients with a history of headache (n = 502)

Distribution of headache types in total patients
Distribution of headache types in total patients (n = 502)

CDH, chronic daily headache.
Headache types and sex
When classified by sex, in male patients TTH accounted for 55% of patients,
followed by probable migraine (14.4%), MoA (8.1%) and MA (4.5%). In female
patients, TTH accounted for 47.3% of patients
(n = 185), followed by MoA
(16.4%), probable migraine (12.5%) and MA (7.7%). The rate of migraine was found
to be significantly higher in women than in men (Fig. 1). Distribution of headache types according to sex
(n = 502).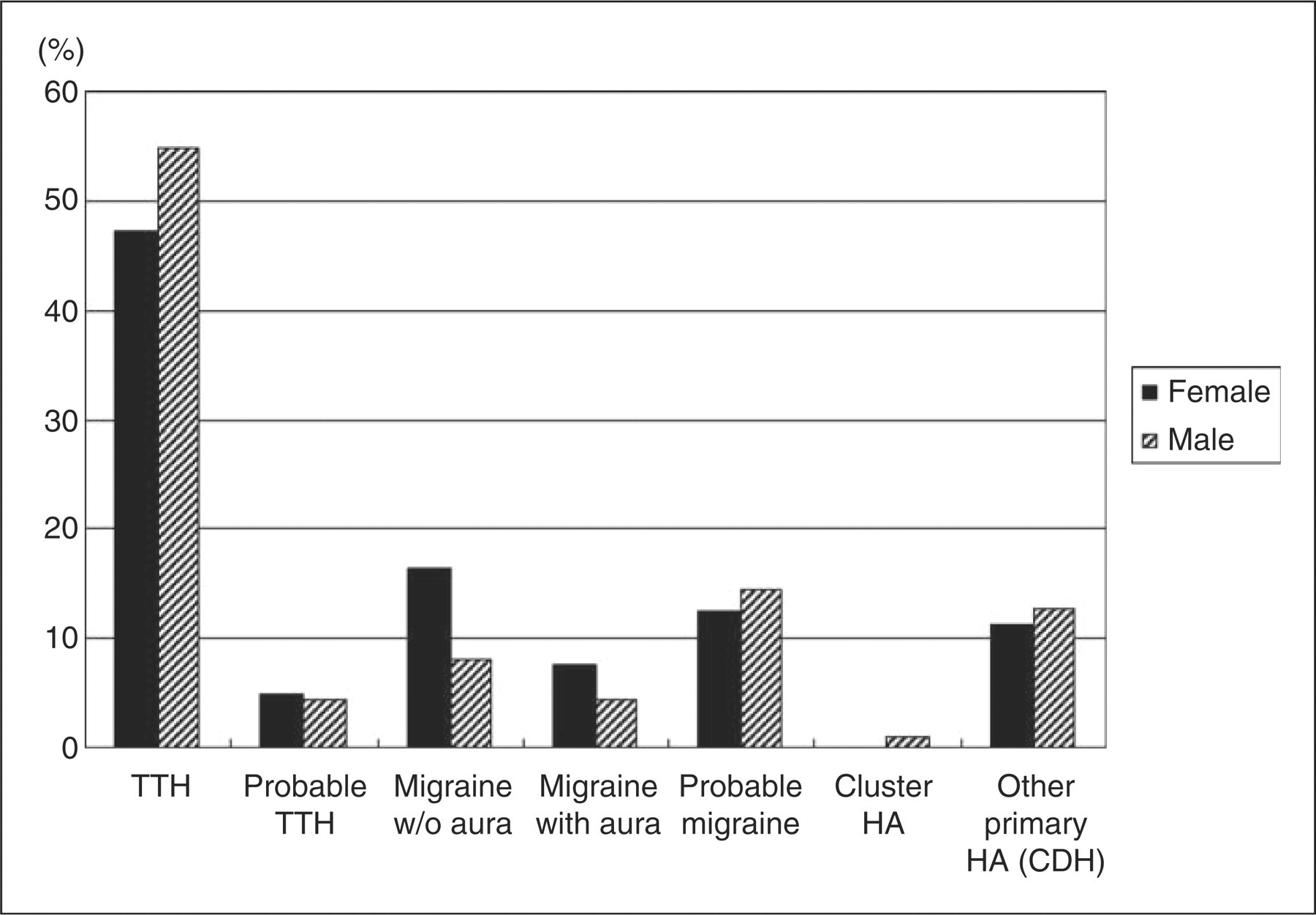
Headache types and age
When headaches were evaluated by age, the rate of each type of migraine (MoA, MA
and probable migraine) was highest in patients in their 20s and 30s and declined
as age increased above 40. In addition, TTH showed the highest rate throughout
all age groups, although it also decreased as age increased (Fig. 2). Distribution of headache types according to age
(n = 502).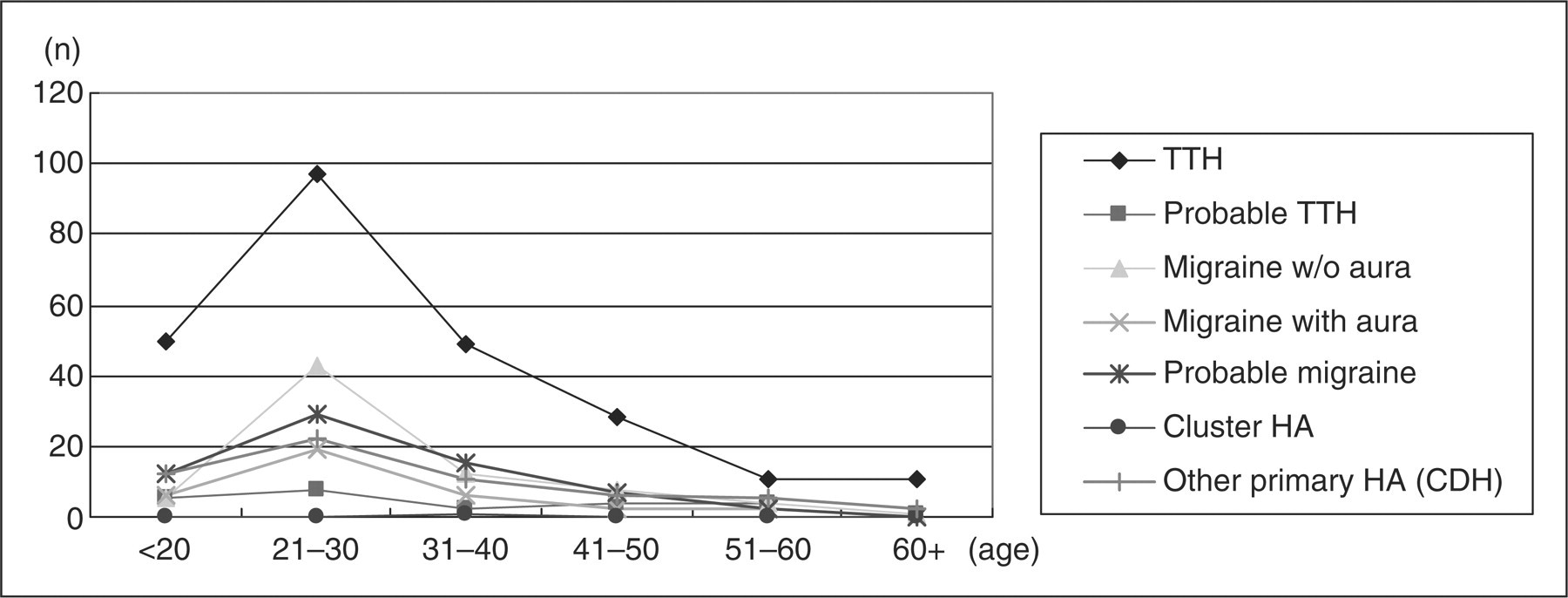
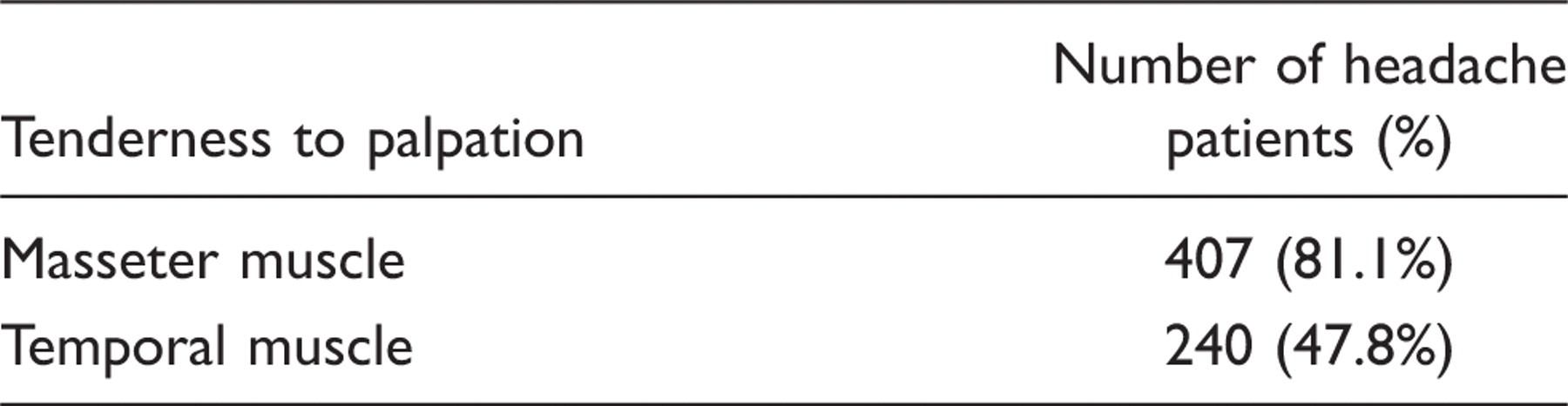
Headache and masticatory muscle pain
Headache and tenderness to palpation of masticatory muscles
Discussion
Headache is a common disease that impacts not only individual lives but also society (1,10,11). Similarly, TMD is widespread, with 70% of the population exhibiting one or more symptoms related to TMD (12). Furthermore, many previous studies have suggested that headache and TMD are related (13–15). Ciancaglini and Radaelli, for example, reported that headache occurred significantly more frequently in subjects with symptoms of TMD than in those without (27.4% vs. 15.2%). Furthermore, there is a scientific investigation that has described the pathways and mechanisms for pain referral from the head to the TMJ and vice versa (16). This overlap often occurs because of an anatomically close relationship and neural innervations.
In this study, TMJ disorder was the most prevalent problem experienced by our subjects (51.6%), followed by masticatory muscle disorders (35.2%), neurovascular pain (6.0%) and neuropathic pain (3.4%). These findings are consistent with those reported in a previous study (17).
In a previous study conducted by the Department of Neurology, Eulji Hospital, Seoul, Korea, the prevalence of migraine was reported to be 26.9%, whereas that of probable migraine, episodic TTH and probable episodic TTH was reported to be 5.1, 21.3 and 6.6%, respectively (18). In this study, we used ICHD-II criteria to assess the patterns of headache in patients who visited the TMJ and Orofacial Pain Clinic at our facility. Among the patients included in this study, TTH showed the highest prevalence, followed by migraine. In addition, one patient was diagnosed with cluster headache. Although the prevalence of migraine (21.5%) was lower than that reported in the previous study, that of TTH (49.0%) was much higher than in the previous study.
When the prevalence of headaches was compared between male and female patients, the prevalence of migraine was found to be higher in women than in men (female : male ratio 35.8:25.3), which is similar to the results of previous studies (2,19). On evaluation by age, the prevalence of migraine was highest in patients in their 20s and 30s and declined as age increased above 40. TTH showed the highest rate throughout all age groups, although it also decreased as age increased.
In addition, 81.1% of patients presented with masseter muscle pain and 47.8% with
temporal muscle pain in this study. Interestingly, of headache patients presenting
with temporal muscle pain, 30% reported that the headaches were triggered by
palpation of temporal muscles. This finding suggests that pericranial muscle pain
may be an inducing factor of primary headache (20,21). Improvement of headache after
treatment of muscle pain through medication, physical therapy, and trigger point
injection has been reported by Jensen and Olesen (22). In addition, botulinum toxin
therapy, which is known to inhibit muscle contraction temporarily, has also been
reported to be effective in treating headache (23,24). The difference in the
prevalence of TTH, which was highest in our study, may suggest that TMD is often
accompanied by muscle pain. Because patients presenting with TMD often suffer from
headaches as well, it is important that an appropriate examination and diagnosis be
made to ensure that the patient receives proper treatment. In addition, TMD may
induce or aggravate headache, therefore proper evaluation and management of TMD is
essential to treat headache in a TMJ and orofacial pain clinic (Fig. 3). Dr Olesen's postulates on the mechanisms of tension-type
headache (TTH).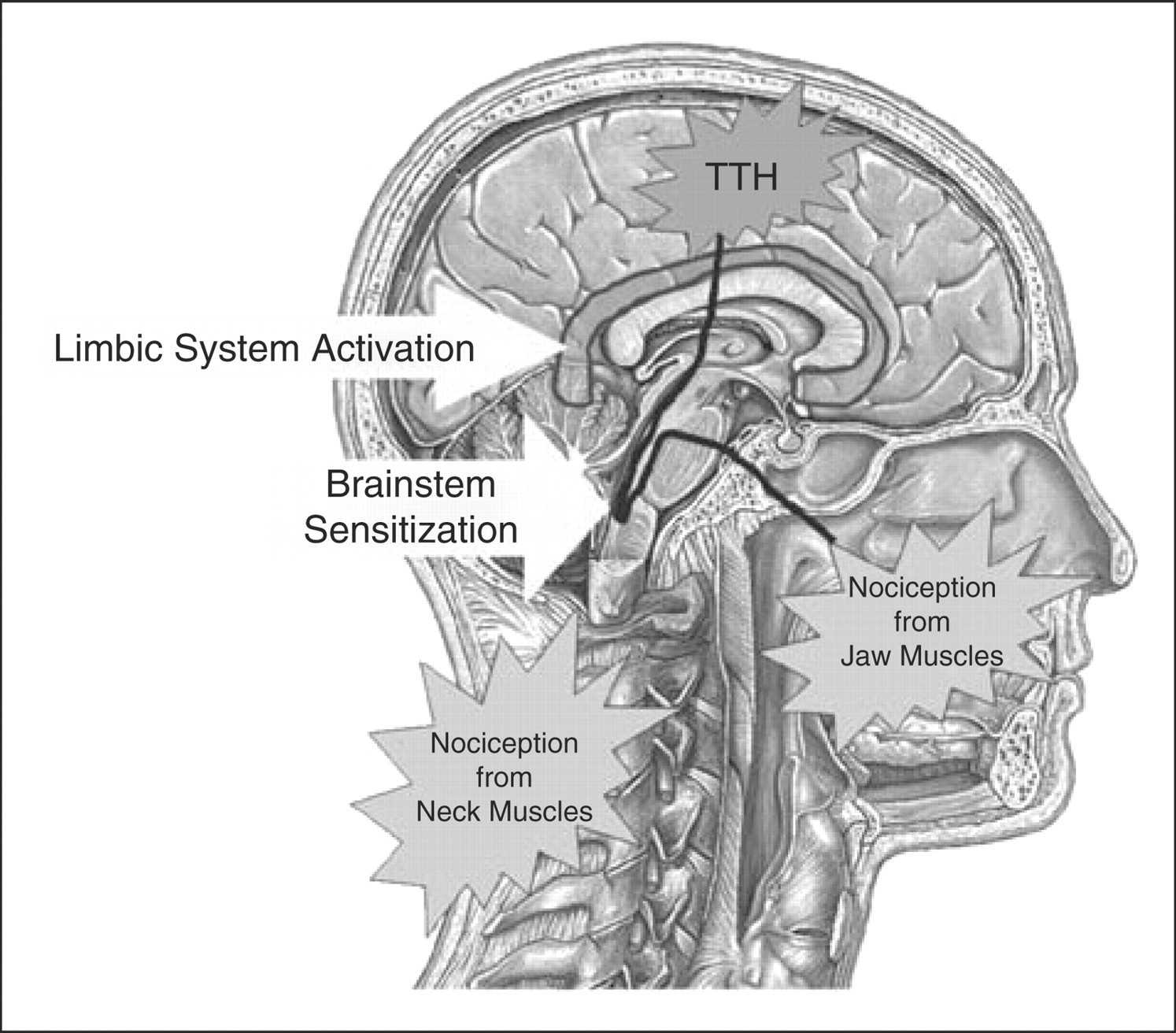
The limitation of this study is that the subjects were limited to patients of a TMJ and orofacial pain clinic. Because general dental clinic patients were not included as a control group, we could not compare the difference between the two groups (TMJ and orofacial pain clinic patients group and general dental clinic patients group). Future studies that include both populations will be helpful in exploring any systematic difference between the two groups, and further advancing our understanding of this topic.