
Abstract
Migraine is more likely to be misdiagnosed in patients with comorbid diseases. Not only primary care physicians, but also specialists might misdiagnose it due to the lack of diagnostic criteria awareness. The ID migraine test is a reliable screening instrument that may facilitate and accelerate migraine recognition. This study aimed to compare the prevalence and characteristics of migraine in a large sample of patients admitted to clinics of ophthalmology (OC), ear, nose and throat diseases (ENTC) and neurology (NC), as well as to validate the use of the ID migraine test in OC and ENTC settings. This was a multicentre (11 cites) study of out-patients admitting either to NC, ENTC or OC of the study sites during five consecutive working days within 1 week. From each of the clinics, 100 patients were planned to be recruited. All recruited patients were interviewed and those having a headache complaint received an ID migraine test and were examined for headache diagnosis by a neurologist, blinded to the ID migraine test result. A total of 2625 subjects were recruited. Only 1.3% of OC patients and 5.4% of ENTC patients have been admitted with a primary complaint of headache, whereas the percentage of NC patients suffering from headache was 37.6%. Whereas 138 patients (19.3%) in OC, 154 (17.3%) in ENTC and 347 (34%) in NC were found to be ID migraine test positive, 149 patients (20.8%) in OC, 142 (16%) in ENTC and 338 (33.1%) in NC were diagnosed with migraine. The sensitivity, specificity, and positive and negative predictive ratios of the ID migraine test were found to be similar in all clinics. An important fraction of the patients admitted to NC, as well as to OC and ENTC, for headache and/or other complaints were found out to have migraine by means of a simple screening test. This study validated the ID migraine test as a sensitive and specific tool in OC and ENTC, encouraging its use as a screening instrument.
Introduction
Despite the fact that migraine headache is diagnosed in less than half of all migraine patients, it remains one of the most common and disabling disorders encountered by physicians (1–9). Moreover, 77% of undiagnosed patients have reported substantial disability related to their headaches (10).
Migraine is more likely to be misdiagnosed in patients with comorbid diseases (11). Not only primary care physicians, but also specialists might misdiagnose it due to the lack of diagnostic criteria awareness. The International Headache Society (IHS) has proposed criteria for the diagnosis of migraine and other headache disorders (12), but it is widely held that these are being utilized poorly worldwide not only at primary care level but also by the potentially related specialists, since it is a rather complicated process. Therefore, simple screening tools are needed to aid the physician in the diagnosis of migraine. Lipton et al. have developed and validated a simple set of questions to screen for migraine in patients who have had frequent and severe headaches (13). The internal consistency of this three-item questionnaire was found to be high, and the operating characteristics of the model remained similar in clinically relevant subgroups (e.g. groups of different age and sex, as well as those with and without aura).
The low rates of correct diagnosis and treatment have several other causes, including low rates of referral to the specialists specifically for headache. On the other hand, physicians must not be blamed solely for this poor diagnosis profile in migraine, as some patients do not seek medical care for headaches or seek help from specialists who are not neurologists or headache specialists. It has been reported that patients with unrecognized migraine are more likely to consider themselves as suffering from ‘tension headache’ or ‘stress headache’ (14). Some patients have been admitted to headache specialty clinics after many years of belief that they had ‘sinusitis’ or ‘eye disorders’. Migraine's visual aura symptoms and/or ocular pain may lead some patients to the ophthalmologist for the first evaluation (15), and likewise its vertiginous symptoms (16) or the pain localized in the forehead or face evoking the suspicion of sinusitis or vertigo-like complaints causes admittance to the ear, nose and throat clinic (ENTC) (11, 17). Therefore, validated migraine screening tools, for not only primary care physicians but also for clinical specialists other than neurologists or headache specialists, are of potential value to prevent delay in appropriate migraine treatment, and may lead to referral for the patients who require specialty care.
The aim of the present study was to investigate the prevalence and characteristics of migraine among out-patients admitted either for headache or other causes to the ophthalmology clinic (OC) and ENTC in comparison with those admitted to the neurology clinic (NC), and to validate the use of the ID migraine test in OC and ENTC settings.
Methods
This was a multicentre (11 sites) observational study of out-patients presenting either to NC, ENTC or OC of the study sites during five consecutive working days within any week of June 2005. All patients who were > 17 years old, were able to communicate and gave signed informed consent to be included in the study. The patients were assured that declining to participate would in no way affect their care or treatment.
After Ethics Committee approval, patients were recruited according to a systematic sample selection method. The planned sample size was 100 patients from each of the clinics. The patient recruitment order was calculated for each individual centre, and in every study day a random number between 1 and 10 was chosen for determining the order of the first patient. r is a coefficient for calculating the recruitment order and is calculated by dividing the average number of patients admitted to that specific centre for the same day of the week at previous months by 20 to ensure the recruitment of around 20 patients regularly distributed within that day. z is a random number between 1 and 10, changing every study day and indicating the recruitment order of the first patient. The recruitment order is as follows: z, z + r, z + 2r, z + 3r, …, z + 19r. If any of these candidates did not meet the criteria for entering the study (not capable of communicating, unwillingness to enter the study; being < 18 years old, etc), the next patient was recruited without altering the following recruitment order.
The recruited eligible patients were interviewed about their sociodemographic characteristics and medical histories with a structured questionnaire designed for this study. Afterwards, the patients were asked two ID migraine pretest questions; the aim was to find out whether they had had two or more headaches during the past 3 months (13). If the answer to one of the two questions listed below was affirmative, the participants were enrolled for an ID migraine test and examination by a neurologist combined with a semistructured interview: (i) Do your headaches limit your ability to work, study, or enjoy life? (ii) Do you want to talk to your healthcare professional about your headaches?
The three ID migraine test screening questions were as follows: during the last 3 months, (i) Did you feel nauseated or sick to your stomach with your headaches? (ii) Did light bother you when you had a headache (drastically more than when you did not have headaches)? (iii) Did your headache limit your ability to work, study, or do what you needed to do for at least 1 day?
The cut-off point for a test diagnosis of migraine headache was two or more positive responses. This test had previously been linguistically validated for Turkish (data on file, Pfizer). Regardless of the test result, i.e. whether the test indicated migraine or not, neurologists or trained neurology residents interviewed the patients who had been subjected to the test using a symptom checklist based on a semistructured diagnostic headache evaluation prepared according to IHS criteria of The International Classification on Headache Disorders, 2nd edn (12) and assigned a clinical diagnosis of migraine, tension type or other headaches.
Detailed questions were asked about the headache in this interview. Specific questions included age at onset, headache frequency and duration (without acute medication), total life-time headache duration, pain intensity (mild, moderate or severe), headache features (i.e. location and quality of pain, effect on headaches of physical activity, and the occurrence of nausea, vomiting, photophobia, phonophobia, or any aura) and specific triggers. The following precipitating factors were assessed: stress, sleeping disorders (lack of sleep and/or oversleeping), skipping meals or fasting, menstruation in women, food items, bright lights, wind (south-west wind), specific smells, smoking, and alcohol.
Descriptive statistics were performed on demographic and clinical variables, and on responses to the migraine screener test. For the validity assessment of the three-item ID migraine test screener, the sensitivity and specificity of the screener against migraine diagnosis based on IHS criteria were evaluated. Positive and negative predictive values for the test were also calculated both for the group with two positive answers as well as for the group with all positive answers. The sensitivity was defined as the ratio of screener-positive subjects to subjects with migraine according to IHS criteria. The specificity was defined as the ratio of screener-negative subjects to the subjects without migraine according to IHS criteria. The positive predictive value is the ratio of subjects with migraine according to IHS criteria to all subjects with positive screener; the negative predictive value is the ratio of subjects without migraine according to IHS criteria to all subjects with negative screener.
χ2 tests were used for comparisons between patient subgroups admitted to the OC, ENTC and NC. The level of statistical significance was considered to be P < 0.05.
Results
Patient characteristics
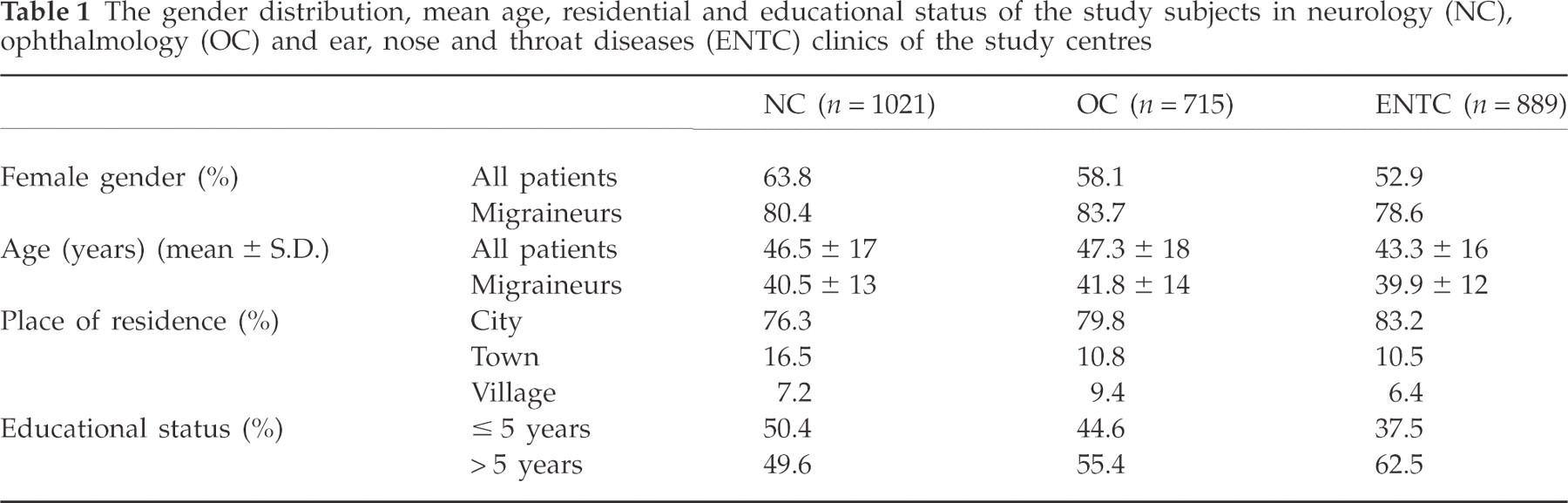
The study was performed in 11 centres in various cities of Turkey. A total of 2625 subjects at the NC (n = 1021), ENTC (n = 889) and OC (n = 715) were recruited for the study. Sociodemographic features (gender distribution, age, place of residence and education) did not differ significantly among the groups, whereas the number of female migraine patients was significantly higher than the males. Mean ages were similar in all groups (P < 0.05; Table 1).
The gender distribution, mean age, residential and educational status of the study subjects in neurology (NC), ophthalmology (OC) and ear, nose and throat diseases (ENTC) clinics of the study centres
Migraine prevalence and characteristics
Upon specific questioning for headache, a total of 1585 patients [429 patients (60%) in OC, 489 patients (55%) in ENTC and 667 patients (65.8%) in NC] reported having headaches. Of all 2625 subjects, 1021 (38.9%) who gave a positive answer to either or both of the pretest questions were screened with ID migraine test and examined by the neurologists or a trained resident. Only nine patients (1.3%) in OC and 48 (5.4%) in ENTC were admitted with a primary complaint of headache, whereas 384 (37.6%) patients were seeking medical advice for their headache in NC.
The neurologist's final diagnoses according to the criteria of IHS in the three groups are shown in Table 2, headache characteristics are shown in Table 3 and headache localization and severity are shown in Figs 1 and 2. Although it did not reach the level of statistical significance, migraine (especially migraine with aura), frequent episodic tension-type headache and chronic tension-type headache were more often diagnosed and migraine patients with continuous headache more often admitted to NC (Tables 2 and 3); nausea and worsening of the headache with movement were less common in patients admitted to OC, whereas the headache worsening with movement was more common in ENTC (Table 3).
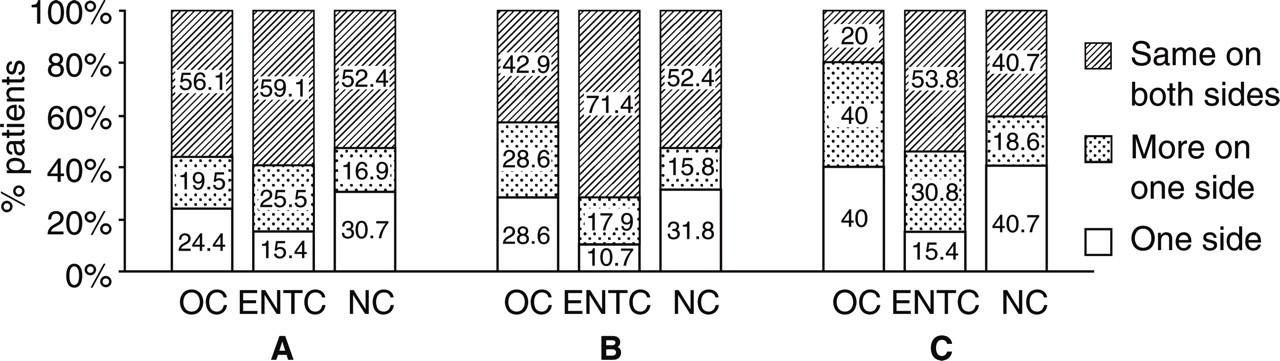
The localization of headache (A) in all screened patients (those subjected to the ID migraine test and answering at least one of the two prescreening questions positively), (B) in patients admitted with a complaint of headache, and (C) in patients diagnosed with migraine by the neurologists; in neurology (NC), ophthalmology (OC) and ear, nose and throat diseases (ENTC) clinics of the study centres.
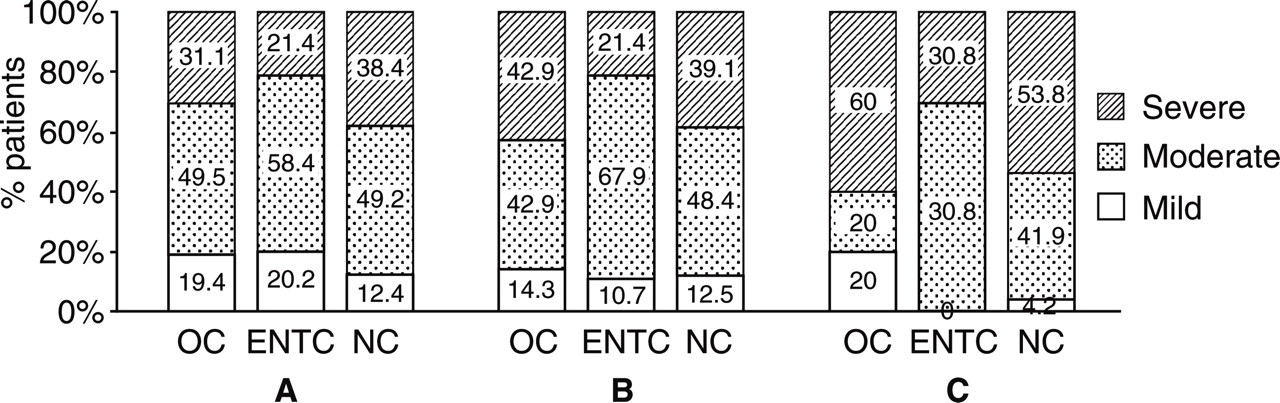
The severity of headache (A) in all screened patients (those subjected to the ID migraine test and answering positively at least one of the two prescreening questions), (B) in patients admitted with a complaint of headache, and (C) in patients diagnosed with migraine by the neurologists; in neurology (NC), ophthalmology (OC) and ear, nose and throat diseases (ENTC) clinics of the study centres.
The neurologist's diagnoses according to the criteria of the International Headache Society in neurology (NC), ophthalmology (OC) and ear, nose and throat diseases (ENTC) clinics of the study centres

*There were patients with headache of more than one type.
The headache characteristics of the migraine patients in neurology (NC), ophthalmology (OC) and ear, nose and throat diseases (ENTC) clinics of the study centres

Chronic daily headache patients were patients with migraine who had > 14 headache days per month for more than the last 3 months. They included patients with chronic migraine and patients with medication overuse headache associated with migraine. Of all migraine patients, 18.1% had chronic daily headache (21.3% in NC, 13.4% in OC and 15.5% in ENTC), whereas 81.9% had episodic migraine.
Sensitivity and specificity of ID migraine test
In all screened subjects, 62.6% were found to be ID migraine positive (two or more positive answers to three questions). Table 4 shows the detailed ID migraine test results obtained from each clinic. More than half of the ID-migraine-positive patients (54.6%) have answered all three questions positively, whereas the remaining subjects gave positive answers to any two questions. Although no significant differences were found between specialty clinics regarding ID migraine results, the number of patients with disability without nausea or photophobia encountered at NC was higher (6.4% of NC, 2.8% of OC and 4.3% of ENTC patients). Also, patients with only photophobia were more common in OC (2.2% in NC, 3.6% in OC and 1.8% of ENTC patients) (Table 4).
The ID migraine test results of patients admitted to neurology (NC), ophthalmology (OC) and ear, nose and throat diseases (ENTC) clinics of the study centres

ID+, ID migraine test positive; ID−, ID migraine test negative; ID+/−, ID migraine test positive or negative.
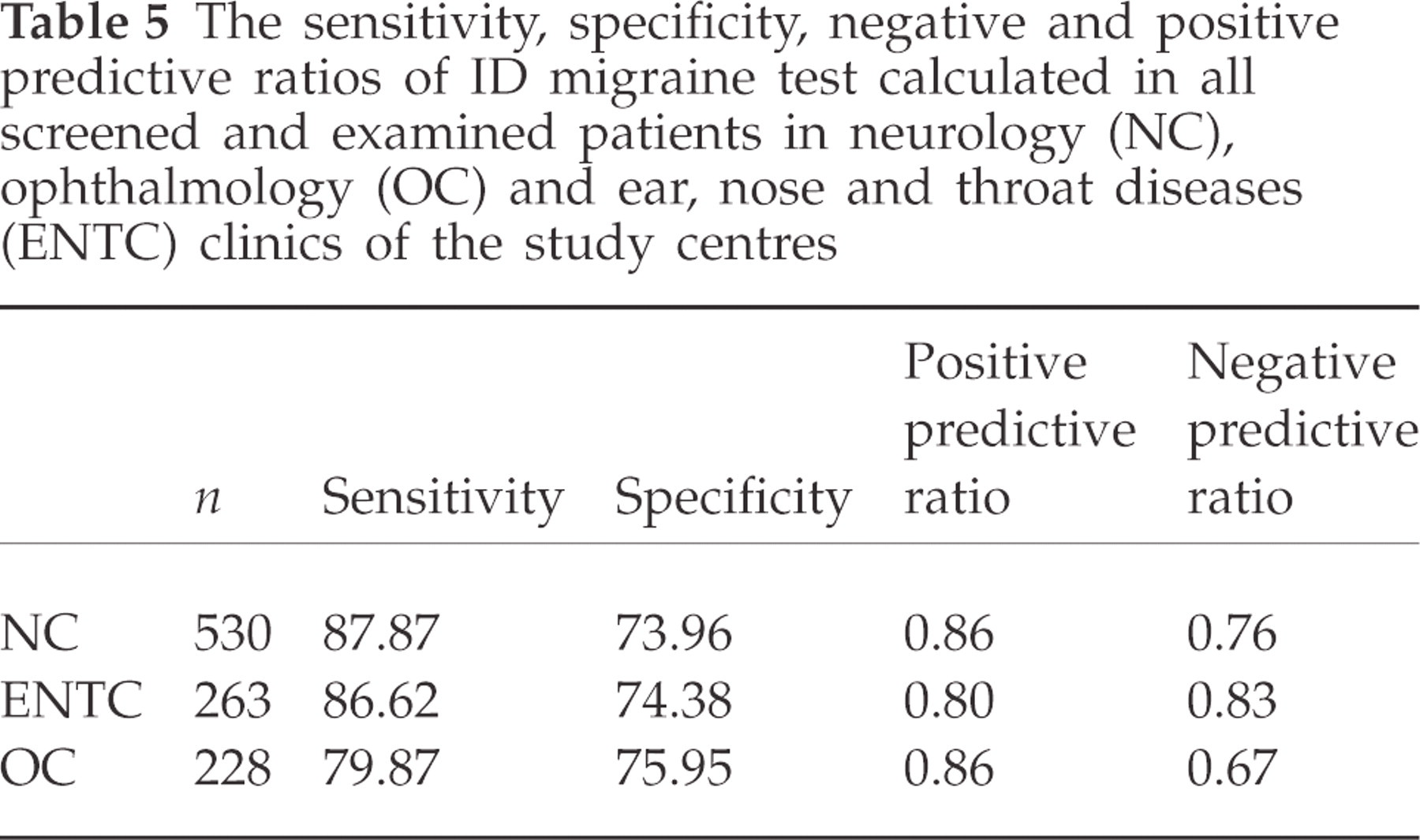
The sensitivity, specificity, negative and positive predictive ratios of ID migraine test in the three groups are shown in Table 5. ID migraine test was positive in 86.2% of episodic migraine patients and in 83.3% of chronic daily headache patients, with no significant difference.
The sensitivity, specificity, negative and positive predictive ratios of ID migraine test calculated in all screened and examined patients in neurology (NC), ophthalmology (OC) and ear, nose and throat diseases (ENTC) clinics of the study centres
Triggering factors
Stress, lack of sleep, skipping meals/fasting, wind, menstruation, smells, smoking, oversleeping, specific foods and alcohol were reported as triggering factors. The distribution of the triggering factors was similar between the groups, but some of the triggering factors, such as lack of sleep, skipping meals and smoking, were less commonly mentioned by patients admitted to OC (Table 6).
Reported triggering factors for headache attacks in migraine patients in neurology (NC), ophthalmology (OC) and ear, nose and throat diseases (ENTC) clinics of the study centres

History of medication for headache
Of all patients, 94% reported that they used medication for their headaches with similar rates in all specialty clinics. Analgesics and non-steroidal anti-inflammatory drugs were used as the major medication group in the majority of patients (86.7% in NC, 88.6% in OC and 86.6% in ENTC). Of migraine-specific drugs, triptans were used most frequently in all groups. Triptans were reported to be used by 14.8% of the patients, which was the highest among the three study groups (2% in OC and 7% in ENTC) and three times more frequent than ergots (5.3%) in NC, whereas ergot use was 6% in OC and 2.1% in ENTC.
Discussion
This study has presented a substantially higher prevalence of migraine among patients admitted to neurology out-patient clinics (33.1%), as expected; nevertheless, about 1/5 of the patients admitting to both ophthalmology (20.8%) and ENT (16.0%) clinics also had migraine, some of them being severe cases. Interestingly, the patient groups presented very similar profiles of headache localization and characteristics. Furthermore, the ID migraine screening test, which is a very simple and easy-to-apply tool, seemed to be valid in the assessment of those patients. Therefore, it could be used for the routine evaluation of all patients admitted to non-neurological specialty clinics for any kind of primary complaint, and could be of help in identifying potential migraine patients so that they can be referred to neurology clinics or headache specialty clinics.
Studies of abbreviated diagnostic criteria intended to simplify the diagnosis of migraine headache can be found in the medical literature (13, 18). The ID migraine screening test developed and validated within a primary care population by Lipton was used in our study (13). In the first ID migraine test study, 75% and 79% of patients had migraine headache based on clinical evaluation and IHS criteria, respectively, and the sensitivity analysis showed that the diagnostic properties of the three-item screening instrument did not differ substantially by sex, age, presence of other comorbid headaches, or previous diagnostic status. Our study has shown that the ID migraine test is a valid tool in ophthalmology and ENT clinics, also.
It is noteworthy that a remarkable number (57%; 198 of 347) of patients with a positive ID migraine test also responded positively to all three items questioned. This suggests that nausea, photophobia and disability caused by migraine headache have a tendency to appear together. Thus, any increase in pain or nausea or other associated symptoms may also trigger an increase in the others, thereby having a multiplier effect and resulting in a more intense and prolonged migraine attack, as suggested by others (19, 20).
We analysed the triggering factors of migraine headaches to outline any differences between the groups admitted to three different specialty clinics. The careful monitoring of the triggering factors of headache could be an important step in migraine treatment, since their avoidance may reduce the frequency and severity of attacks. A minority of the study population have reported alcohol to trigger migraine. This finding is extremely low compared with other studies, which report 29–35% alcohol triggering (21–23). The explanation for this difference, which is quite simple, is that since our sample consisted mostly of Muslims, most of them abstained from alcohol. According to Kelman's study, osmophobia occurs in about one-quarter of migraine patients during an acute migraine attack, whereas perfume or odour trigger migraine in almost 50% of patients (24). We expected that the migraine patients with osmophobia or with attacks triggered by smells would be admitted more frequently to ENTC than other clinics, but this was not the case. The triggering factors for migraine headache in different clinics were distributed more or less similarly in our study, but the patients admitted to OC reported lack of sleep, skipping meals and smoking less frequently than other patients. Wind-induced attacks were reported most in ENTC (46.7%). Photophobia is described by 66–88% of individuals with migraine and is included as one of the major criteria for migraine diagnosis in the IHS classification (25). The higher number of patients with photophobia in OC (3.6%) compared with ENTC (1.8%) and NC (2.2%) reflects the misinterpretation of migraine by patients as an eye problem.
Our study has shown that the disability rates and severity of migraine in NC are higher than in other clinics; likewise, patients having migraine with aura were admitted more frequently to NC (9.2%) than to OC (3.9%) or ENTC (1.9%). The fact that 90% of patients who had reported a worsening of the headache with movement were admitted to ENTC seems to demonstrate that such a symptom evokes suspicion of sinusitis. On the other hand, patients with osmophobia were not abundant in ENTC.
In conclusion, ID migraine test is a sensitive and specific tool in OC and ENTC besides the NC, and its use as a screening instrument must be encouraged. The sensitivity, specificity and positive/negative predictive values in different clinics are comparable. The possibility of migraine should be considered in all patients presenting at OC and ENTC, and neurologists or headache specialists should play a leading role in the diagnosis and treatment of this disabling and prevalent disorder.
Acknowledgements
This study was supported by an unrestricted research grant made by Pfizer-Turkey. The authors wish to thank the researchers the names of whom are listed below:
MIRA-3 study group