
Abstract
Our aim was to measure and compare the link between pain patients and the different kinds of analgesic medications they use by the Leeds Dependence Questionnaire (LDQ). This is a self-completion 10-item instrument to measure the severity of dependence upon a variety of substances. LDQ was administered to 200 episodic migraine patients (EM group), 77 chronic migraine patients (CM group) overusing acute medications, and 114 patients suffering from rheumatic disease (RD group), consecutively attending the Headache Centre or the Rheumatology Clinic of the University Hospital of Modena in the course of the first semester of 2007. The link with analgesics was greater in migraine patients than in patients with rheumatic disease, since the LDQ total score was significantly higher in the EM (6.65 ± 0.32, P < 0.005) and CM groups (9.61 ± 0.59, P < 0.0001) than in the RD group (5.17 ± 0.37) (Kruskal–Wallis and Mann–Whitney U-tests). Migraine patients were significantly more linked to triptans and to combined medications than to non-steroidal anti-inflammatory drugs. The strength of the link between migraine patients and the analgesic medications they take could represent a factor of vulnerability: overusing these medications could develop medication overuse headache.
Keywords
Introduction
Both people suffering from rheumatic diseases (1) and those suffering from headache (2) commonly take analgesic medications. The overuse of acute medications can transform self-limited headache into a chronic form (3), named medication overuse headache (MOH) (4), especially in migraine patients. This chronic headache is highly disabling and difficult to treat. Only the withdrawal of the offending medications and the beginning of adequate prophylactic treatment allow an improvement of the disorder within months, but relapse remains frequent (5). Any acute medication can cause MOH, if taken frequently and for a sufficient period of time (6). However, pharmacological properties of the different acute medications seem to be important in determining the frequency of MOH, the speed of inducing it, the outcome of treatment and the propensity to relapse (7, 8). Indeed, it has been reported that opioids, butalbital, caffeine and ergotamine have a high probability of inducing MOH (9). After withdrawal treatment, patients overusing opioids have the highest relapse frequency (10). If overused, triptans, which are specific antimigraine drugs, can induce MOH even more rapidly than other analgesics (11). Excluding triptans and ergotamine, migraine and rheumatic disease patients take the same types of analgesic medications (1). Nevertheless, patients with rheumatic diseases overusing acute medications do not develop MOH if they are not also primary headache sufferers (12–14).
Despite the growing interest in MOH, few tools have been developed to study specifically the relationship between migraine patients and the acute medications they take. The Leeds Dependence Questionnaire (LDQ) is a self-administered questionnaire which can measure dependence upon a wide variety of substances (15). The aim of our study was to analyse, by means of LDQ, whether the link with analgesic medications was different between migraine and rheumatic disease patients, and if the degree of the attachment varied according to the kind of preferred medication.
Patients and methods
Subjects
During the first semester 2007 we recruited (Table 1) three groups of subjects, all White: (i) the episodic migraine (EM) group: 200 patients suffering from migraine with and/or without aura according to the International Classification of Headache Disorders, 2nd edn (ICHD-II) criteria (4), consecutively attending the out-patients' wards of the Headache Centre of the University Hospital of Modena for a follow-up visit. This group's favourite symptomatic medications were: non-steroidal anti-inflammatory drug (NSAIDs) alone in 120 subjects (60%), triptans in 60 (30%), combinations with caffeine or with codeine in 20 (10%); (ii) chronic migraine (CM) group: 77 subjects suffering from chronic migraine according to ICHD-II criteria (4, 16) and overusing acute medications, consecutively admitted to the in-patients' ward of the Headache Centre to undergo withdrawal from their overused medications. Self-reported favourite symptomatic medications were: NSAIDs alone in 41 (53%) subjects, triptans in 22 (29%), combinations with caffeine or with codeine in 14 (18%); (iii) rheumatic disease (RD) group: 114 subjects suffering from rheumatic diseases (disorders of connective tissue 51%, spondyloarthropathies 21%, rheumatoid arthritis 16%, osteoarthritis 7%, psoriatic arthritis 3%, and gout 2%), consecutively attending the out-patients' wards of the Rheumatology Clinic of the University Hospital of Modena for a follow-up visit. This group's favourite symptomatic medications were: NSAIDs alone in 108 (95%) subjects, and combinations with caffeine or with codeine in six (5%) subjects. All symptomatic medications preferred by the patients were prescription drugs. The diagnoses of migraine patients and of patients suffering from rheumatic diseases were made, respectively, by a specialist of the Headache Centre and by a rheumatologist of the Rheumatology Clinic of the University Hospital of Modena.
Patients' characteristics

EM vs. CM: a
P < 0.05,
CM vs. RD: b
P < 0.05,
RD vs. EM: c
P < 0.05,
EM vs. CM: d P < 0.001, Student's t-test for unpaired data;
EM vs. CM: e P < 0.05, χ2 test followed by Fisher's exact test.
CM vs. RD: f P < 0.001,
CM vs. RD: g P < 0.05, χ2 test followed by Fisher's exact test.
RD vs. EM: h P < 0.001,
RD vs. EM: i P < 0.05, χ2 test followed by Fisher's exact test.
We excluded episodic and chronic cluster headache subjects, chronic and episodic tension-type headache patients, symptomatic headache subjects, patients with rheumatic diseases who declared themselves not to be taking symptomatic medications or to also suffer from headache, and patients who had either a prior history of drug and/or alcohol abuse or strong opioid analgesic use.
The LDQ is a self-completion, 10-item, 0–3 rating scale instrument, designed to measure the severity of dependence upon a variety of substances, according to the frequency (0 = never, 1 = sometimes, 2 = often, 3 = nearly always), independently of the type or quantity of substance used (15). The LDQ total score increases with the increasing degree of substance dependence, yielding a dependence score between 0 (absence of dependence) and 30 (extreme dependence). No cut-off score indicative of dependence has been established (15). In order to have an appropriate questionnaire for our patients, the term ‘drink or drug(s)’ was substituted with the term ‘analgesic(s)’.
Procedures
The LDQ questionnaire was administered to the subjects by two trained medical graduates. Written, informed consent was obtained from each subject, following an exhaustive description of the study procedures and objectives. Each subject was told that the questionnaire was being used only for research purposes. In answering the questions, subjects were instructed to think about the last week, to think about their favourite symptomatic analgesic (and to specify it), and to tick the response that was more appropriate for them. The study was approved by the Ethical Committee of Modena and was conducted in compliance with the Declaration of Helsinki, latest version.
The number of symptomatic medications used was determined by the patients' diaries kept during the months prior to the visit to the Headache Centre or the Rheumatology Clinic. All patients' diagnoses and other characteristics were recorded by clinical documentation.
Data analysis
All data were checked by trained physicians and inserted into a database. LDQ questionnaire scores were compared using the Kruskal–Wallis analysis of variance for non-parametric variables, followed by the Mann–Whitney U-test for independent samples. Statistical differences in patients' characteristics were analysed by χ2 test, followed by Fisher's exact test, to compare percentages, by Student's t-test for unpaired data, to compare mean values between two groups, and by one-way analysis of variance (
Results
Migraine patients (Table 2) were linked to analgesic medications more than patients with rheumatic diseases. Indeed, the LDQ total score of the RD group (5.17 ± 0.37) was significantly lower than that of both the EM (6.65 ± 0.32) and CM (9.61 ± 0.59) groups (Kruskal–Wallis and Mann–Whitney U-tests). Besides having the highest LDQ total score, the CM group had significantly higher scores than the EM and RD groups, respectively, in six and in seven out of 10 items of the questionnaire. The RD group never achieved significantly higher scores than those of the two groups of migraine patients in any items. All three groups of pain patients obtained the top score (EM, 1.69 ± 0.08; CM, 1.70 ± 0.14; RD, 1.38 ± 0.10) in item 8 (asking if getting the effect is more important than the kind of drug) and the lowest scores in the items more evocative of addiction, such as item 3 (exploring compulsion) in the EM group (0.29 ± 0.04), item 9 (investigating the need to maintain a constant effect) in the CM group (0.36 ± 0.08) and item 4 (asking how much the patient plans the day around taking analgesics) in the RD group (0.19 ± 0.05).
Leeds Dependence Questionnaire (LDQ) score (mean ± S.E.M.) for the three groups of patients

EM vs. CM: a P < 0.05;
EM vs. CM: b P < 0.0001.
RD vs. EM: c P < 0.05;
CM vs. RD: d P < 0.0001;
CM vs. RD: f P < 0.005, Kruskal–Wallis test followed by the Mann–Whitney U-test for independent samples.
RD vs. EM: g P < 0.005.
Analysing the total LDQ score by kind of preferred medication (Table 3), migraine patients of both the EM and CM group were linked to NSAIDs significantly less (EM, 5.60 ± 0.34; CM, 7.41 ± 0.64) than to triptans (EM, 8.40 ± 0.71; CM, 11.91 ± 1.19) or combined medications (EM, 7.80 ± 1.06; CM, 12.43 ± 1.32). The CM group was linked to any kind of medication significantly more than the EM or RD groups (Kruskal–Wallis and Mann–Whitney U-tests).
Total Leeds Dependence Questionnaire (LDQ) score (mean ±
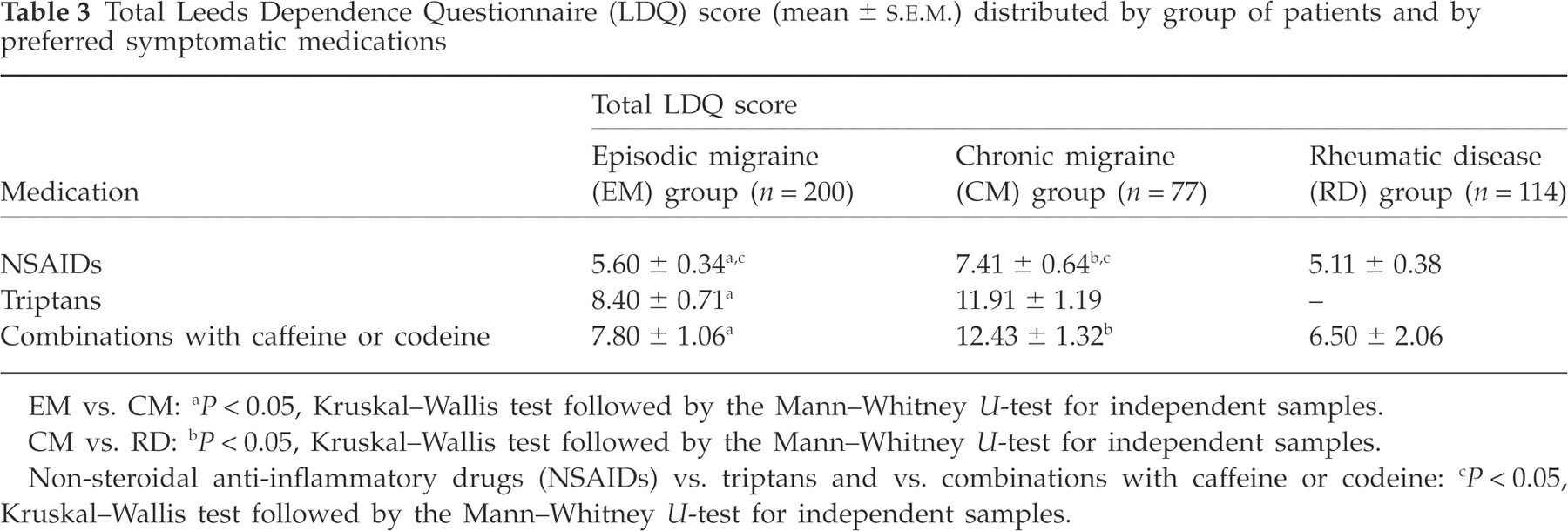
EM vs. CM: a P < 0.05, Kruskal–Wallis test followed by the Mann–Whitney U-test for independent samples.
CM vs. RD: b P < 0.05, Kruskal–Wallis test followed by the Mann–Whitney U-test for independent samples.
Non-steroidal anti-inflammatory drugs (NSAIDs) vs. triptans and vs. combinations with caffeine or codeine: c P < 0.05, Kruskal–Wallis test followed by the Mann–Whitney U-test for independent samples.
Discussion
Our findings show that the link between the pain patient and analgesic medication is greater in migraine patients than in those suffering from rheumatic diseases. The LDQ total score (Table 2) was actually significantly higher in the EM (6.65 ± 0.32, P < 0.05) and CM group (9.61 ± 0.59, P < 0.0001) than in the RD group (5.17 ± 0.37) (Kruskal–Wallis and Mann–Whitney U-tests). It has been recently reported that 66.8% of MOH patients exhibit dependence on acute treatments for headache according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edn (DSM-IV) criteria (18, 19). However, the application of DSM-IV criteria to abuse and dependence in patients with chronic pain has been criticized since it could result in a large number of false positives (20, 21). In our study, we used the LDQ questionnaire, which is particularly suitable for comparison studies; the higher the total score, the greater the link between the patient and the substance (15). Also with this instrument, chronic migraine patients overusing acute medications were those who had the highest degree of attachment to analgesics. By means of the LDQ questionnaire, we found in a previous study (22) that the intensity of analgesic need in chronic headache patients is comparable to addicts' need for substances of abuse. In 122 chronic daily headache sufferers overusing analgesics and in 115 drug addicts with a diagnosis of heroin, cocaine or alcohol dependence, according to the criteria of DSM-IV (18), mean LDQ total scores (±
The degree of attachment to the analgesic varied in both the EM and CM groups according to the kind of preferred medication. Indeed, the LDQ total score (Table 3) was significantly higher in migraine patients preferring either triptans or combined medications than in migraine patients who favoured NSAIDs. It is difficult to hypothesize that the greater migraine patients' attachment to triptans could depend on factors different from the demonstrated effectiveness of these drugs in quickly relieving the migraine attack (24). To our knowledge, non-therapeutic use of triptans has never been reported. Subjects with histories of substance abuse do not like sumatriptan (25). Even more liposoluble triptans do not produce pleasurable effects and patients dislike them (26). Moreover, even if the frequency of triptan-overuse headache has been increasing since the marketing of these drugs, the prevalence of MOH seems to remain stable as a whole over the years (27).
Migraine patients of both the EM and CM groups also had a link to combinations containing caffeine or codeine of intensity similar to the link to triptans. These substances are psychoactive; however, they have a low abuse potential and dependence is rare (28). The high degree of migraine patients' attachment to combined medications could be supported by either the synergistic effectiveness of caffeine and codeine with analgesics (29) or the capacity to counteract mood worsening, anxiety and fear that typically accompany migraine attacks (30). This explanation is supported by the fact that the LDQ total score in the RD group was similar in patients using either NSAIDs or combined medications.
Analgesics may reinforce the antecedent drug-taking behaviour being able to terminate pain, an aversive and unpleasant condition (31). Indeed, it has been hypothesized that abuse potential and analgesic effects are intrinsically related and are mediated by overlapping neural substrates (31). Recent experimental data have demonstrated that analgesic activity of paracetamol involves the cannabinoid system (32–34). These findings could explain the relaxation, slight drowsiness, euphoria, or feeling of tranquillity that have been repeatedly reported following paracetamol administration (35).
NSAIDS are also self-administered in pain conditions, even if they are considered to have almost no abuse liability and used as negative comparators of analgesics with abuse liability, such as hydrocodone (positive comparator) (20). Normal animals would not drink a solution of suprofen. However, when arthritis was induced by injecting Freund's adjuvant, rats drank a pharmacologically active amount of the drug (36). This behaviour was interpreted as evidence either that the rats were self-medicating for pain (36) or that they were treating the distress that accompanies the illness (28). In our study, even EM and RD patients only occasionally taking NSAIDs established some involvement with these favourite medications: the total LDQ score of these patients was much higher than that reported in subjects with no substance use disorder (1.72 ± 3.62), even if certainly lower than that measured in patients with both drug and alcohol disorders (9.10 ± 8.08) (37).
This study has some limitations. As with all surveys of this type, LDQ scores are based upon patients' direct responses. However, our pain patients had no reason to answer incorrectly; every medication that they used as a symptomatic analgesic was legal, non-narcotic and a prescribed drug. Patients suffering from rheumatic diseases used a low number of symptomatic medications. This datum could depend on the fact that all were also following pharmacological treatments (corticosteroid and/or disease-modifying anti-rheumatic medications) capable of reducing disease activity. However, it has been reported that in clinical samples, in contrast to population surveys, underuse of analgesic drugs is common (28) and that analgesic intake is higher among headache sufferers than in subjects with other chronic pain, such as neck or low back pain (38). Our findings apply therefore to migraine and rheumatology clinic patients who are the target of prescription medications; they cannot be generalized to other patients and contexts.
We believe that the link to analgesic medications is stronger in migraine than in rheumatic disease patients not because of a higher addiction susceptibility or for the psychotropic properties of the drugs, but because analgesics are more important in the management of migraine than in the treatment of rheumatic diseases. The great importance of analgesics for migraine patients could depend on two factors: first, the limited efficacy of available prophylactic treatments, which do not eliminate, but simply reduce the frequency of attacks; second, the lack of aetiological treatments capable of acting on the mechanisms which cause migraine and of preventing the progression of the disease. Nowadays there are available different specific anti-rheumatic medications capable of modifying the disease process (39, 40). Rheumatic patients can merely use analgesics in addition to these specific treatments. For migraine patients, analgesics are instead indispensable to treat the disease, as also appears from the classification of migraine treatments into acute (i.e. analgesics) and prophylactic (41). This hypothesis is supported by the results of our study: migraine patients (both episodic and chronic) reached significantly higher scores than rheumatic patients in item 10, investigating the difficulty of living without analgesics. According to this interpretation it is plausible that the better the analgesic medication answers the migraine sufferer's need, the more important it becomes for the patient. Every time that the patient experiences its efficacy, the link to the analgesic becomes stronger. Of course, if migraine attacks become more and more frequent, the patient will use his/her preferred analgesic more and more often and in increasingly large doses. With time, the recourse to that analgesic, which seemed initially a solution, will in fact only complicate the path towards cure, causing rebound headache and the development of MOH. Therefore, the strength of the relationship between the migraine patient and analgesic medication might represent a factor of vulnerability: overusing these medications could develop MOH.
In the clinical setting, LDQ testing could serve as an easy tool to alert physicians treating migraine patients when further intervention is needed to prevent analgesic overuse.