
Abstract
Although triptans represent the standard of care for migraine that is severe, disabling and/or suboptimally responsive to migraine non-specific analgesia, they are often underused in clinical practice. Simple analgesics and non-steroidal anti-inflammatory drugs (NSAIDs) may provide effective treatment in some patients, but it is an inadequate response to these drugs that drives the therapeutic progression to triptans at the end of the traditional ‘step-care’ approach. However, there are several disadvantages to this approach. It may cause patients to lose confidence in their physician during this hierarchical ‘trial-and-error’ search for optimal treatment when prescribed medications are ineffective, leading them to cease consulting before triptans are tried. It may also result in a protracted time interval of suboptimal treatment, with unnecessary suffering in patients who are triptan candidates. The alternative approach of ‘stratified care’, in which medication is prescribed according to the severity of symptoms, enables triptans to be used earlier in the treatment plan, especially when triptan candidates are given a choice between simple analgesic/NSAID and triptan medication from the start. This raises the question about the efficacy of triptans in triptan-naïve (TN) patients. A recent exploratory post-hoc analysis compared the effect of almotriptan 12.5 mg in TN patients (n = 342) with that in triptan-experienced patients (n = 237). Almotriptan was effective in both cohorts with a consistent trend in favour of the efficacy of almotriptan in TN patients, notably for sustained pain freedom (SPF) and SPF plus no adverse events. Moreover, both headache recurrence at 24 h and the use of rescue medication was lower in the TN patients, whereas tolerability was equally good in both cohorts. These findings indicate that TN patients can expect excellent symptom control when they progress from non-specific analgesia to treatment with almotriptan and support the earlier use of triptans in line with the stratified care paradigm.
Introduction
The widely held view of most headache societies and migraine specialists is that triptans are the therapy of choice for the symptomatic treatment of patients suffering from moderate–severe migraine. This is particularly so in patients who are suboptimally responsive to migraine non-specific treatments such as simple analgesics and non-steroidal anti-inflammatory drugs (NSAIDs). Nevertheless, triptans appear to remain underutilized in clinical practice. This overview will examine the extent of, reasons for and potential consequences of this underutilization. It will also consider clinical strategies that may be used to improve this situation for migraine patients, with the aim of reducing the level of suffering and disability that migraine can cause. In addition, this paper will examine the response to triptans in triptan-naïve (TN) migraineurs relative to the response in triptan-experienced (TE) migraine patients who have chosen to continue treatment with triptans. This provides an opportunity to consider if the transition from migraine non-specific treatment to triptans presents a clinical barrier to the subsequent use of triptans after first exposure that might, in part, explain the underuse of triptans in migraine patients.
Prescription patterns of migraine medications and related patient behaviour
Results from surveys of the patterns of prescription of migraine medication in different countries (France, Germany, Italy, UK, USA) (1, 2) indicate that the most frequently prescribed medications for migraine are simple analgesics/NSAIDs (ranging from 36% in France to 97% in Italy), whereas the prescription rate for triptans in Europe is much lower (ranging from 3% in Italy to 13% in France) (Fig. 1a).1 Moreover, the pattern of prescription of simple analgesics/NSAIDs appears to be inversely proportional to that of triptans (Fig. 1b), even though patient satisfaction with migraine non-specific medications is notably lower than that with triptans. Two independent studies, conducted in Spain and involving > 1000 migraineurs, each indicated that approximately two-thirds of patients expressed satisfaction with triptan treatment, in contrast to < 10% with simple analgesics and approximately one-quarter with NSAIDs (3, 4) (Fig. 1c). This is consistent with the findings from another study in the USA, in which patients who made the transition from migraine non-specific therapy to triptans reported significantly improved satisfaction with the latter over the former (5).
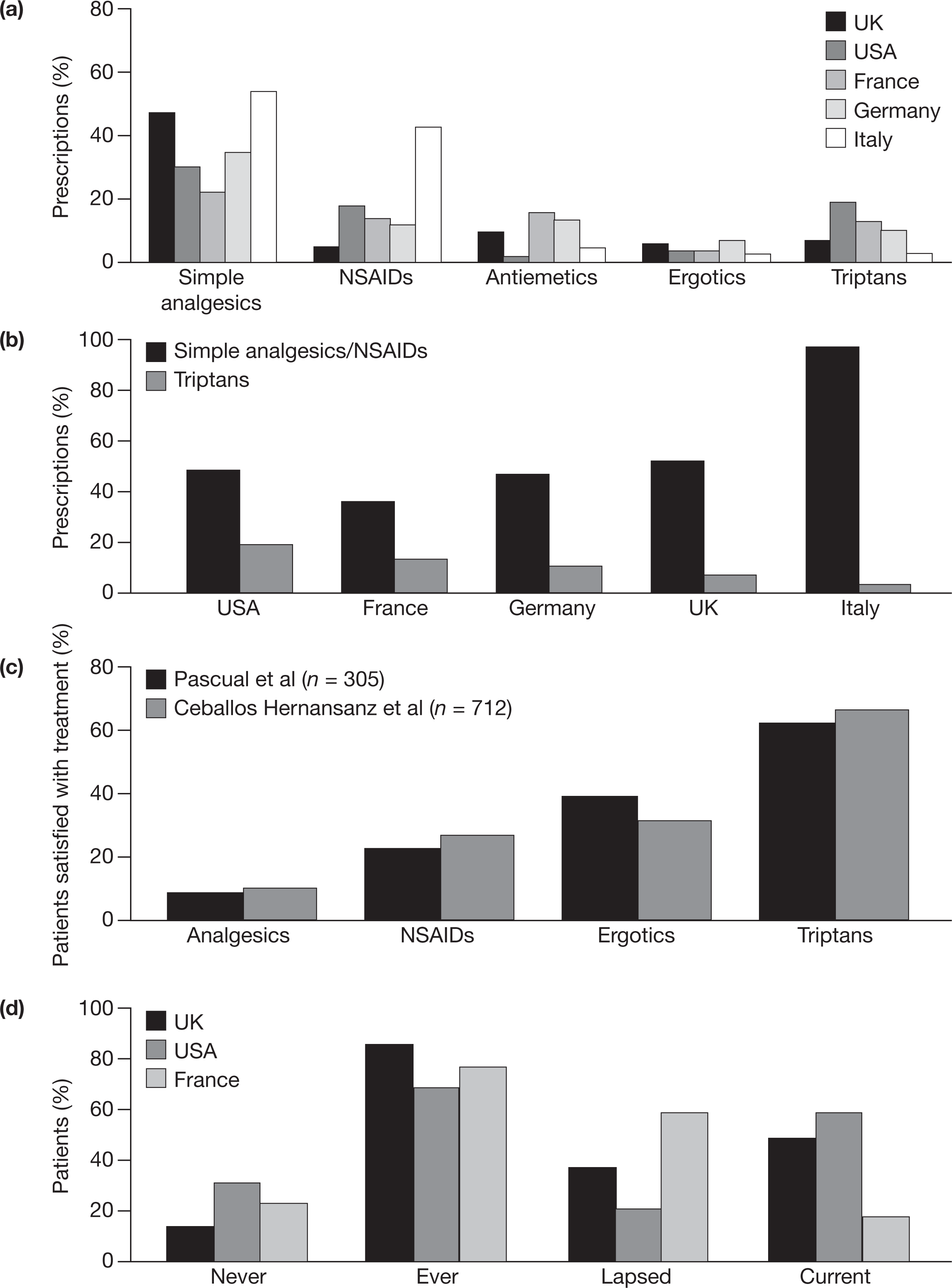
The apparent discrepancy between prescription patterns of, and patient satisfaction with, different migraine medications may be a reflection of a treatment approach that does not always meet patient expectations. An indication that this might be the case comes from observations that whereas most migraineurs consult their physician, at least initially, a substantial proportion of patients subsequently stop consulting. This pattern of consulting behaviour is evident across different countries (2, 6, 7) (Fig. 1d). There are two principal possibilities for this high level of lapsed consulting behaviour in migraine patients: patients are either satisfied with the treatment from their physician so they consider further consultations unnecessary, or they are in some way dissatisfied with their consultation and seek their own solution. The former reason is the ideal, although unlikely in most lapsed consulters. The latter gives rise to some concern that is shared by the European Headache Federation (EHF) (8), which has issued a declaration of consensus actions to be achieved by 2010. These target actions include an increase from 30% to 50% in the proportion of migraine patients under the care of a physician, an increase from 40% to 70% in the proportion of patients receiving ‘effective’ therapy, and at least 50% of patients who need migraine-prevention therapy to be receiving such treatment. Achieving these objectives will require careful appraisal of the treatment approach applied by physicians, notably in the primary care setting, to ensure that patients have expedient access to the most appropriate treatment that not only meets their expectations, but also encourages patient and physician engagement to reduce the risk of lapsed consultation for reasons of dissatisfaction.
Achieving optimally effective treatment paradigms in migraine
The traditional approach to managing migraine is the step-care paradigm, in which all patients receive medication in a hierarchical sequence in a quest to find an optimally effective solution. This paradigm essentially uses a trial-and-error approach starting with migraine non-specific medication, progressing through a series of alternatives and combinations, and culminating in the initiation of migraine-specific treatment (Fig. 2a). There are two potentially undesirable consequences that justify a challenge to the step-care approach. One is that patients who disengage with their physician early (and become lapsed consulters) do not have the opportunity to progress to triptan therapy. The second is the time interval between the first consultation and the first exposure to triptans in candidate migraineurs, which, in an ideal scenario, should be as short as possible. However, the period of time between the diagnosis of migraine and the first exposure to triptans can be protracted; for example, a review of data accrued during recent clinical trials in migraine indicates an average interval of 11 years before migraineurs were treated with a triptan (9). This finding prompts several fundamental questions signifying the limitations of the step-care approach: do all patients need to wait so long before progressing to triptan medication; how much unnecessary suffering have patients endured before they have the opportunity to progress to triptan therapy; and how can candidates for triptan treatment be identified more quickly? An alternative treatment paradigm that addresses the limitations arising from the step-care approach, while avoiding the inappropriate use of triptans, is the stratified-care approach.

Influence of treatment approaches on progression to appropriate triptan using (a) a step-care approach and (b) a stratified-care approach.
The stratified-care paradigm as a vehicle to identify triptan candidates earlier
The stratified-care paradigm differs from the step-care approach in that it endeavours to match migraine characteristics, elicited by consultation, with the profile of different medication options (Fig. 2b). In this way, the most appropriate treatment can be used according to the severity, frequency and level of disability associated with the migraine attack (10). Moreover, by allowing the patient to decide which medication provides the best outcomes, optimal treatment decisions are expedited while maintaining engagement between the patient and the physician, consistent with the EHF targets (8).
When used judiciously, the stratified-care approach is likely to expose more TN patients to this treatment option earlier in the course of the illness. Such patients are, however, not a wholly homogeneous population, and comprise two groups: patients who are aware of triptans and those who are not. This distinction is important, because their clinical management requires subtly different approaches. Patients who are not aware of triptans are TN patients who have neither sought nor been offered migraine-specific medication in the past. These patients need clear and straightforward counselling about this class of medication. TN patients who are aware of triptans may require a different approach to counselling that addresses their expectations, because they may have preconceived ideas, encompassing enthusiasm or reluctance, about their exposure to triptans. ‘Enthusiastic’ triptan-aware TN patients may have unrealistically high expectations with associated risks of dissatisfaction and/or medication overuse, while ‘reluctant’ patients may have concerns or fears that require reassurance. The evidence of the benefits of triptans in TN patients raises three further issues that need to be considered during their management: what can TN patients reasonably expect from their first exposure to triptans, which triptan to use, and are there any differences in the clinical response to triptans in TN and TE patients that manifest as therapeutic tolerance?
In terms of patients' expectations of their first exposure to triptans, there is evidence that, as well as improved patient satisfaction, migraineurs who have not previously taken triptan medication report more rapid relief of pain, more effective pain relief, and more rapid resumption of daily activities than when taking non-triptan medication (5). Moreover, selection of the most appropriate triptan needs to be based not only on careful consideration of the evidence (5, 11), but also on a target outcome measure that meets patients' expectations. Pain relief at 2 h post dose is a desirable but imprecise end-point to judge the effectiveness of treatment, because even though patients meet the pain relief criteria they may still have residual pain. Pain freedom at 2 h is a more robust end-point because it is more specific, although it does not take into account the risk of symptoms returning after 2 h. Sustained pain freedom (SPF), defined as pain freedom at 2 h plus no rescue medication and no headache recurrence within 24 h of dosing, is the current standard target outcome, although it does not take into account the potential burden of treatment-related adverse events. SPF plus no adverse events (SNAE) is the most robust yet challenging end-point measure that can discriminate between triptans to enable the selection of a triptan that offers the best chance for effective migraine management. In this regard, almotriptan 12.5 mg scores most highly of all available triptans (5, 12). Moreover, expectations that are achieved in TN patients should be enduring with repeated triptan treatment for subsequent migraine attacks. However, there is limited evidence to enable a comparison between outcomes in TN patients and TE patients. One post-hoc study has indicated that the response to eletriptan is indistinguishable between TN and TE patients (5, 13). This comparison has been explored further in migraineurs treated with almotriptan.
Almotriptan in triptan-naïve migraine patients
To compare the clinical response to almotriptan in migraine patients who had no prior exposure to triptans with that in patients who had previously received any triptan for their migraine, a post-hoc analysis was undertaken in patients who had moderate–severe migraine pain at baseline using data pooled from three clinical trials (5, 14–16). The history of prior triptan exposure was known in a total of 579 patients in these trials; 342 were TN and 237 were TE. In both patient cohorts, most were female (86.0 and 86.9%, respectively), although the mean age was slightly higher in the TE cohort [39.3 years (S.D. 10.5)] than in the TN cohort [36.7 years (S.D. 10.6)]. A greater proportion of patients in the TN cohort had severe pain at baseline (43.0% vs. 30.4% in the TE cohort) and, correspondingly, a greater proportion of TE patients had moderate baseline pain (68.4%) compared with the TN cohort (56.4%). All patients were instructed to take a single dose of almotriptan 12.5 mg when their migraine pain had reached at least moderate severity; a small proportion in each cohort actually took medication when their headache pain was mild (0.6 and 1.3% in the TN and TE cohorts, respectively). The efficacy end-points used for this comparative analysis were pain relief at 2 h after dosing with almotriptan, 2 h pain freedom, SPF and SNAE. Other outcome measures evaluated in this analysis were headache recurrence at 24 h, the use of rescue medication and the occurrence of any adverse event.
The results of a preliminary analysis are shown in Fig. 3a. Almotriptan 12.5 mg was effective across all end-point parameters in both TN and TE patients. For the more challenging end-points of SPF and SNAE, there was a trend favouring TN patients. Of the other end-points, fewer TN patients experienced headache recurrence at 24 h and they took less rescue medication. The low frequency of adverse events of any aetiology showed that almotriptan 12.5 mg was equally well tolerated by both TN and TE patients, and that there was no excess tolerability burden in TN patients. The trend to a greater overall apparent benefit of almotriptan in TN patients is intriguing and worthy of further exploration. First, the contention that TN patients suffer from less severe migraine pain than TE patients needs to be considered against the background that a greater proportion of TN patients in the present analysis reported severe migraine pain at baseline than TE patients. This shows that perceived pain intensity is no less challenging to treat in TN patients. Second, these findings need to be considered against the placebo response in TN and TE patients. Two studies have enabled exploration of this effect in patients with moderate to severe pain at baseline (13, 16). Both studies showed a similar trend for more favourable outcomes with placebo in TN than in TE patients (Fig. 3b), suggesting that TN patients may have greater expectations of treatment than TE patients. The clinical relevance of these observations lies in the importance of treating migraine to patients' expectations as a fundamental premise upon which to build tailor-made treatment paradigms for individual patients, particularly during the early consultation phase. It also underlines the greater relevance of the stratified-care than the step-care approach to expedite optimal treatment outcomes with triptans.

Summary and conclusions
It is clear that, for a variety of reasons, triptans are not being used to their full therapeutic potential in the treatment of migraine. Addressing these reasons is a key factor in improving outcomes in migraineurs. The transition from a step-care to a stratified-care treatment paradigm offers an important opportunity to identify patients who are triptan candidates earlier in the treatment pathway. Patients who make the switch from migraine non-specific treatment to triptans exhibit better outcomes and increased treatment satisfaction. Furthermore, preliminary analysis indicates that migraine patients can expect excellent symptom control when they progress to first triptan exposure with almotriptan 12.5 mg.
Footnotes
Competing interests
J.P. has acted as a paid consultant to Almirall.
Acknowledgements
The author would like to thank Stuart Donovan PhD, from Complete Medical Communications, who provided medical writing support funded by Almirall.
1The survey by MacGregor et al. (![]() ) focuses on prescribed medication and does not take into account physician recommendations to patients about the use of over-the-counter medications for migraine. The availability of such medications may vary across different countries, which may account for some of the disparity between countries.
) focuses on prescribed medication and does not take into account physician recommendations to patients about the use of over-the-counter medications for migraine. The availability of such medications may vary across different countries, which may account for some of the disparity between countries.