
Abstract
The purpose of the present trial was to evaluate semi-standardized acupuncture efficacy in migraine prophylaxis. Twenty-eight subjects with migraine were randomized to the real or sham acupuncture groups. Semi-standardized and standardized minimal acupuncture were used, respectively, in the two groups of patients. They were all treated with 16 acupuncture sessions in 12 weeks. Both groups exhibited similar reductions in: percentage of patients with reduction of migraine ≥40% and ≥50% regarding frequency of migraine attacks, days with migraine, frequency of migraine attacks, average duration of a migraine attack, rate of rescue medication used, average headache severity rate and other parameters compared with the baseline period. Associated symptoms, such as nausea and vomiting, also showed equal estimates in both groups. These findings showed that semi-standardized acupuncture shows no difference from sham acupuncture in preventing migraine attacks.
Introduction
Acupuncture has been largely used for migraine sufferers in western countries, although the role it may play in migraine treatment remains unknown (1–3). Some trials have pointed out some effects of acupuncture in migraine, but no conclusive results have been reached, probably because there have been only a few high-quality trials in this area (4, 5).
Migraine does not exist as an entity in the theory of traditional Chinese medicine (TCM) (6). The basis of acupuncture follows the TCM grounding. However, there are serious methods of diagnosis, treatment and practice as far as acupuncture is concerned. In western countries practice sometimes follows the paths of neurophysiology, neuromuscular and other modern concepts and principles (7). According to TCM's principles, treatment should be individualized (8). Each acupuncturist should treat accordingly to their own experience and feelings. In fact, acupuncture can be applied in different ways. Traditional Chinese acupuncture basis has been disregarded in most trials. Usually, a standard treatment has been adopted regardless of the previous TCM diagnosis (9, 10). Furthermore, several acupuncture techniques have also been applied, although they cannot be matched to the original technique (7, 11). Therefore, comparisons of acupuncture trials are very difficult (7). Is there a midway betwwen traditional concepts and the scientific approach? The authors thought that the semi-standardized acupuncture treatment could be the best way, because TCM would be partially respected and the treatment would be easily reproduced in other trials in the future as well as in clinical practice.
The present trial was developed to evaluate the efficacy of semi-standardized acupuncture in migraine prophylaxis.
Methods
Study design
The present study was developed in the Headache Clinic of the Department of Neurology, in the Clinical Hospital, State University of Campinas (UNICAMP), Brazil. The protocol and supporting documents (information sheet, consent form, protocol) were approved by the institutional Ethics Committee in June 2000.
The recruitment of patients was done from August 2002 to March 2003, and the trial was completed in February 2004 (including all follow-up periods). Patients were recruited via a media campaign. They were scheduled by the research assistants and evaluated by an experienced neurologist.
Twenty-eight patients suffering from migraine, with or without aura, in accordance with the diagnostic criteria of the International Headache Society (IHS) (12), present for at least 1 year, male and female, aged 18–50 years, were enrolled. Other inclusion criteria were: patients with only migraine, patients who had not used drugs with migraine prophylactic effects or acupuncture in the previous 3 months, patients who could come to the clinical hospital 17 times only in the following 12 weeks (acupuncture treatment period) and patients who had accepted inclusion in the study after oral and written explanations about the clinical trial. The exclusion criteria were patients with any other chronic pain syndrome, who were unable to understand and maintain headache diaries, who were misusing drugs or alcohol and who occasionally used a minor tranquilizer or sedative.
Prior to enrolment there was a 4-week preliminary phase (baseline period) when patients kept a diary recording the frequency and intensity of headache, menstruation, drug intake and associated symptoms in each migraine attack. By that time, the selected patients had received a written text with information about all aspects of the trial, including possible adverse events and their right to withdraw from the trial at any time without giving reasons. During that period at least three, but not more than six migraine attacks, had to occur. A new attack was considered as such when the patient had been headache free for at least 48 h (13). Patients with non-migraine types of headaches were excluded as well as patients who had used drugs for the treatment of migraine attacks for more than 10 days in 4 weeks. After the baseline period, during the second neurologist visit, the selected patients signed the written informed consent. Before acupuncture treatment, the patients were evaluated by a general physician, who is also an acupuncture specialist (J.A-A.). At this time, the clinical history and physical evaluation based on the principles of Chinese medicine were recorded, including examination of the pulse and tongue. The evaluation was done and the probable treatment following TCM principles was planned for all patients in order not to break the ‘blinding’.
After the acupuncture doctor's evaluation, patients were randomly assigned to two acupuncture groups, group C and group D, by a research assistant. The research assistant prepared opaque, numbered and sealed envelopes containing one of the two above letters. They were divided into six blocks. A block had six letters, three letter Cs and three letter Ds. The random digits (14) were used to define the sequence of the letters in each block. Therefore, the order of the letters was different for each block. That sequence was unknown by the medical acupuncturist. The identification of each letter was unknown by the first and second research assistants, the statistician, the neurologist (evaluator) and the patients. Only the medical acupuncturist knew the meaning of each letter, but she had not revealed any code before completing all the data analysis. The second research assistant was responsible for sending the randomization list to the statistician at the end of the trial. Group C received the real acupuncture and group D the sham acupuncture. The acupuncturist doctor did not give any information to the patients, neurologist or research assistants about the acupuncture treatment.
Real and sham acupuncture are defined in World Health Organization (WHO) Guidelines for Clinical Research on Acupuncture (15) as being ‘acupuncture given as a real clinical treatment’ and ‘inappropriate acupuncture for the condition being treated taking into account the acupuncture microsystem’.
The patients were submitted to the acupuncture treatment for 12 consecutive weeks. That included 16 sessions, twice a week during the first 4 weeks and weekly during the following 8 weeks. Patients had to keep a headache diary from the baseline period (diary 1) up to follow-up period (diaries 5–10), which was for 24 weeks after the last acupuncture session (approximately 6 months). The follow-up period was designed to test the longer-lasting effects of acupuncture on migraine. During the acupuncture treatment, the patients completed three diaries (diaries 2–4). Neurologist visits were scheduled at weeks 0, 5, 18, 25, 33 and 42. Treatment of migraine attacks, if they happened, was done in the customary manner by each patient. The neurologist withheld any suggestions as to changes in the ongoing rescue medication and any comments on the acupuncture treatment with the patients.
Treatments
Sham acupuncture treatment
Twelve needles (six on each side) were inserted in each session (see Table 1).
Minimal acupuncture was used and consisted of very shallow needle insertion in the acupuncture points.
No manipulation was done.
The points in the sham acupuncture group were selected after an extensive consultation of the classical acupuncture literature to confirm that they had minimal or no influence on headaches (16–21).
Standardized and fixed acupuncture treatments were applied to the 16 sessions.
Protocol treatment in the sham acupuncture group (points)

Lian YL, Chen CY, Hammes M, Kolster BC. The Seirin pictorial atlas of acupuncture. An illustrated manual of acupuncture points. Cologne: Könemann Verlagsgesellschaft mbH Press 2000.
Real acupuncture treatment
The treatment was semi-standardized (see Table 2). The chosen points were related to the pain topography of the most frequent migraine attacks in each patient and based on some principles of traditional Chinese medicine.
From 6 to 10 points were used in each session (12–20 needles were inserted).
Each patient had a fixed treatment in their 16 sessions.
The needles were manipulated by rotation methods to produce a characteristic sensation known as De Qi. The ‘Qi sensation’ was explained to the patients of this group in the first session as an awareness of numbness, strange aching or tingling radiating from the point of needling.
Protocol treatment in the real acupuncture group (points)

Lian YL, Chen CY, Hammes M, Kolster BC. The Seirin pictorial atlas of acupuncture. An illustrated manual of acupuncture points. Cologne: Könemann Verlagsgesellschaft mbH Press 2000.
Treatment design in both groups
The skin was disinfected with 70% alcohol.
Sterile disposable and steel needles (0.25 × 40 mm) were used.
Moxa or electrical stimulation was not used.
The patients were kept lying down for 30 min with the needles in place.
Body acupuncture was done bilaterally.
Efficacy evaluation
Efficacy was measured by comparing the first diary, which was made in the baseline period, with the diaries of the treatment period (diaries 2–4) and of the follow-up period (diaries 5–10). Each diary covered 4 weeks.
Primary efficacy parameters
The percentage of patients with a reduction of ≥40% in migraine attack frequency from the second to the fourth diaries compared with the first diary (baseline period).
The percentage of patients with a reduction of ≥50% in migraine attack frequency from the second to the fourth diaries compared with the first diary (baseline period).
Total migraine days from the second to the fourth diaries compared with the first diary (baseline period).
Secondary efficacy parameters
Frequency of migraine attacks.
Average duration of a migraine attack.
Average headache severity.
Total duration of migraine pain in hours per diary.
Rate of rescue medication used.
Nausea frequency.
Vomiting frequency.
The severity of headache was evaluated on a 4-point scale (0, no headache; 1, mild headache = migraine not interfering with daily activities; 2, moderate headache = migraine interfering with daily activities; and 3, severe headache = migraine making normal daily activities impossible) following IHS recommendations (13).
Safety measures
The patients were instructed to report all adverse events to the medical acupuncturist in each session as well as in a paper that they had received before the first session. Adverse events were listed descriptively and comparison between groups was done, ascribing some statistical significant difference to some effects.
Subjects’ evaluation
Patients were fully informed that two kinds of acupuncture would be done. One would be real and the other would be false, placebo. No additional information was given.
At the end of the study, patients were invited to fill in a questionnaire evaluating the acupuncture treatment and to give their impression about which treatment group (real or sham acupuncture) they thought they had been included in.
Statistical analysis
The sample size was determined considering the results shown in an unpublished pilot trial that had been done before this present trial. The endpoint considered to calculate this sample was the percentage of patients with reduction of ≥40% in their migraine attacks in the second month of treatment with sham or real acupuncture. The equivalence range was 11.8–57.9% for patients with a reduction of the attack rate of 40% and with α= 0.05 and β= 0.20. The number of patients required was 26 divided into two groups. As a drop-out rate of 15% was expected, 30 patients had to be enrolled into the study.
Statistical comparisons were done using univariate analysis with the χ2 test and Fisher's exact test. Analysis of variance (Anova) for repeated measures was used to compare both groups. Comparisons within groups for the migraine parameters in each one of the periods were done using the Tukey's post-hoc test. Differences within each group were estimated using the profile test by contrasts. The significant level used for the statistical analysis was 5%, therefore P < 0.05 indicates significance.
Results
Patients
The selection of patients for the trial took place from August 2002 to March 2003. The follow-up period was from July 2003 to February 2004. Thirty-one migraine sufferers were enrolled in the study. They were randomly assigned to the real (16 patients) and sham acupuncture (15 patients) groups. However, only 28 patients completed the treatment and they were included in the statistical analysis. The flow of participants through each stage of the trial is presented in Fig. 1. There was no significant difference between study completers and drop-outs in diary scores, group of treatment, age or headache characteristics.

The flow of participants
The groups’ demographic data are presented in Table 3. There was only one statistically significant difference between groups, the age mean. The patients in the sham acupuncture group were older than in the real acupuncture group (P = 0.024).
Patient demographic characteristics

Efficacy and long-term follow-up (24 weeks)
No statistically significant difference between groups was observed in any pain parameter evaluated in this trial. Nevertheless, comparisons within each group found that all migraine pain parameters had improved with statistically significant differences in both groups. There was one exception: headache severity when the patients were experiencing pain.
Associated symptoms
The Tukey test showed that the real acupuncture group had significantly reduced nausea during the follow-up period when compared with the sham acupuncture group (F(9,198) = 2.09; P = 0.0372). The variance analysis showed that the variability in the graph lines is not attributable to chance.
There was no statistically significant difference between groups regarding the number and frequency of vomiting during attacks.
Rescue medication
No statistically significant difference appeared between groups or within each group.
Adverse effects
No serious adverse effect (AE) was notified. Most AEs observed were related to the local insertion of the needles, such as: local pain after session, ecchymosis, small haematomas, nodule and local paraesthesia during session. General effects were sleepiness and relaxing sensation; however, a statistically significant difference was observed in sleepiness in the real acupuncture group (P = 0.008), as well as in local nodules (P = 0.008) and local pain after sessions (P = 0.002).
Treatment impressions
All patients announced their intention to be treated with acupuncture in future. When they were asked how they would classify the treatment, patients who received real acupuncture classified it as good (28.6%), very good (42.8%) and excellent (28.6%). Patients who were in the sham acupuncture group rated it as regular (14.3%), good (35.7%) and very good (50%). In the sham acupuncture group nobody classified the treatment as excellent. Likewise, in the real acupuncture group, every patient qualified the treatment as good although there was no statistically significant difference between groups.
When they were asked about the kind of treatment that they received, patients in the real acupuncture group answered: ‘real treatment’ (28.7%), ‘placebo acupuncture’ (7%) and ‘I don’t know’ (64.3%). In the sham acupuncture group, they answered: ‘real treatment’ (28.6%) and ‘I don’t know’ (71.4%). There was no significant statistical difference between the replies from the two groups, indicating that the blinding (keeping the patients unaware of their treatment) was successful.
Discussion
Only one statistically significant difference appeared between groups in demographics characteristics (see Table 3). The age of the patients selected to the real acupuncture group varied from 22 to 50 (mean 32.50) and in the sham acupuncture group from 23 to 49 (mean 39.14). Despite sparse longitudinal prospective epidemiological data and information about the prognosis and natural history of migraine (22, 23), authors considered that this difference did not influence the results. Also, in the present trial the age span for patient selection was not large (18–50 years old). Therefore, no statistical correction for age was applied.
Efficacy
There were no statistically significant differences between the real and the sham acupuncture groups in any pain parameters evaluated in this trial during the treatment or follow-up periods, such as: percentage of patients with reduction ≥40% and ≥50% in migraine attack frequency, total migraine days, frequency of migraine attacks, mean duration of a migraine attack, mean headache severity and total duration of migraine pain in hours per diary (see Figs 2, 3 and 4). No differences were observed between groups in the rate of rescue medication used or frequency of nausea and vomiting. These results are in accordance with three sham-controlled trials testing the efficacy of acupuncture in treating migraine (24–26).

Percentage of responders (reduction ≥40% in migraine attack frequency) in each diary (4 weeks) compared with the baseline period (diary 1) in the real (▪) and sham (□) acupuncture groups. Diaries 2, 3 and 4 correspond to the treatment period (12 weeks). Diaries 5–10 correspond to the follow-up period (24 weeks)

Total duration of pain in each diary (4 weeks) in the real (▪) and sham (•) acupuncture groups. Diaries 2, 3 and 4 correspond to the treatment period (12 weeks). Diaries 5–10 correspond to the follow-up period (24 weeks)
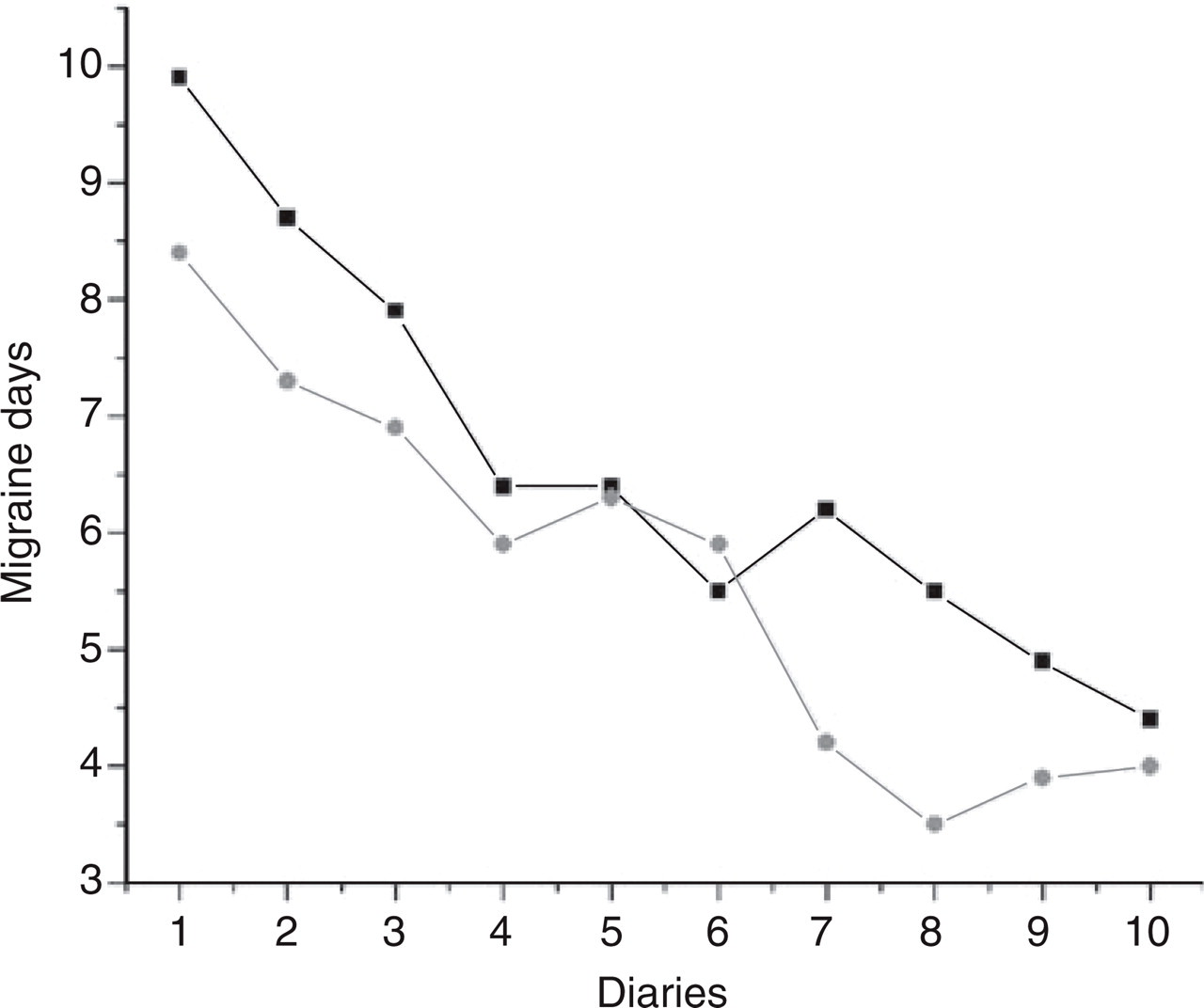
Total of migraine days in each diary (4 weeks) in the real (▪) and sham (•) acupuncture groups. Diary 1 = baseline period (4 weeks), diaries 2, 3 and 4 correspond to the treatment period (12 weeks) and diaries 5–10 correspond to the follow-up period (24 weeks)
Improvement within each group could be observed during the treatment up to 20 weeks after the last acupuncture session (most of the follow-up period) in almost all pain parameters evaluated, with the exception of pain intensity during the migraine attack. Although several trials testing acupuncture or drugs showed improvement of the frequency of migraine attacks, the same was not verified for headache severity (10, 11, 27–31).
It is widely known that:
The placebo effects are higher in pain sufferers than in patients suffering from other complaints (32).
Invasive technical proceedings have higher analgesic effects than oral drugs (2, 33, 34).
The majority of acupuncture trials that tested the efficacy of acupuncture in pain conditions had identified that sham acupuncture could result in a positive response, reducing the possibility of identifying statistically significant differences between real and sham acupuncture (2, 4, 5, 7, 15, 35).
Therefore, the improvement achieved for both groups (real and sham) could be a result of the combination of the three factors referred to above more than the specific effects of the needling. The non-specific effects depend on the patients’ beliefs, such as: the magic effects of the eastern techniques in the western patient's mind, the patients’ beliefs that they are being treated, the acupuncture consultation, the practioners’ expectations of acupuncture effects and the general results of needle insertion (15, 25, 36).
Another point should be highlighted: the improvement rate reached for both acupuncture groups in the present trial was below that of two previous high-quality trials (9, 25). It could be determined by several factors: chance, bias, the sort of semi-standardized acupuncture chosen by medical acupuncturists, the small size of the sample, or large variability of the results observed in both groups. It is important to recall that the patients were aware that the placebo acupuncture treatment was being applied. It is known that in pain studies the response to an active drug is lower in placebo-controlled trials than in open trials or in trials when patients were informed that they would receive only active treatments (32).
Persistence of the improvement lasted up to 24 weeks after the period of treatment (approximately 6 months) in both groups, in accordance with the long-lasting acupuncture effects related previously in three well-designed clinical trials (8, 25, 37). Guidelines and an article containing methodological suggestions for trials in acupuncture also suggested it (4, 15).
The number of days with nausea decreased slightly in the real acupuncture group from the first month of treatment up to the fifth month of the follow-up period, contrasting with the increase of the same variable in the sham acupuncture group. There was a statistically significant difference between them from the third to the fifth month of the follow-up period and the variance analysis did not attribute this result to chance. Nevertheless, the rate of rescue medication used and vomiting in both groups did not change in any phase of the trial.
Adverse events
Effects such as: local nodule (P = 0.008) and local pain after session (P = 0.002) appeared with a statistically significant difference in the real acupuncture group, which is understandable because the depth of needle insertion was very superficial in the sham group. In the real group, damage of superficial vessels and nerves is more likely. Sleepiness was significantly more frequent in the real acupuncture group (P = 0.008) and this is also attributable to the depth of needle insertion.
Limitations
Selection of patients was difficult because of the very strict inclusion and exclusion criteria adopted in this trial, which followed all suggestions presented in two guides: Guidelines for controlled trials of drugs in migraine (13), edited by the IHS, and Guidelines for Clinical Research on Acupuncture (15), edited by the WHO. Most of the volunteers for the trial were eliminated because they had other kinds of headache, mainly chronic daily headache.
The treatment adopted in the real acupuncture group (the semi-standardized treatment) was based on the experience of three medical doctors who have worked with acupuncture from 14 to 20 years. The treatment protocol was based on the topography of the headache related to the theory of traditional Chinese medicine. Therefore, our therapeutic scheme would not be the widespread treatment applied for acupuncturists. In fact, acupuncture practice is very different between acupuncturists throughout the world. The advantage of the semi-standardized treatment is that it could easily be reproduced in future trials, had the results been positive. In fact, acupuncturists know that there is a gap between their practice and what has been done in research. It is a common criticism when acupuncturists and some researchers comment on the scientific approach to the evaluation of acupuncture effectiveness (2, 4, 9).
Conclusion
The aim of the present trial was to verify the efficacy of the semi-standardized acupuncture treatment in migraine prophylaxis. All pain parameters evaluated showed that this approach is not better than sham acupuncture to prevent attacks in migraine sufferers. Results of a previous trial (pilot study) not yet published, where authors used the individualized treatment in the real acupuncture group, seem to offer the best approach. It takes into account all clinical signs and symptoms presented by each patient. However, it is a complex therapeutic scheme and difficult to reproduce.
Footnotes
Acknowledgements
We would like to thank Drs Lo Sz Hsien and Ling Tung Yang for their suggestions about the treatment through Traditional Chinese Medicine. We would also like to thank Leda Fernandes and Heloisa de Lima Gomes for their help in organizing the study and the data. The authors also thank the staff from UNICAMP Press Assessory, the Clinic Hospital Public Relations, Mr Antonio Alberto Ravagnani and the journalist Ani Seixas for their great help with the media. The study protocol was written by the principal investigator (JAA). This work was supported by the State of São Paulo Research Foundation (FAPESP, grant no. 00/09985-0).