
Abstract
Background
Although specific role players are currently unknown, contribution of inflammatory mediators has been suggested in the pathophysiology of idiopathic intracranial hypertension (IIH), which is a disease more prevalent in obese female individuals of childbearing age. We aimed to investigate the levels of adipokines and cytokines to demonstrate possible markers for inflammation that participate in IIH pathophysiology and their association with clinical features of IIH.
Methods
IIH patients, diagnosed according to the revised criteria, and age-, gender- and body mass index (BMI)-matched healthy controls were enrolled in this study. Serum samples were evaluated for insulin-like growth factor 1, insulin, nesfatin, adiponectin, interleukin (IL)-1β, IL-6, IL-8, leptin, plasminogen activator inhibitor type-1, resistin, tumour necrosis factor-alpha (TNF-α) and monocyte chemotactic protein 1 via enzyme-linked immunosorbent assay or multiplex immunoassays.
Results
IL-1β level was significantly higher (p = 0.012), and IL-8 and TNF-α levels were significantly lower in the IIH group (p < 0.001 and p = 0.008, respectively) compared to the control group. There were no correlations between the cytokine/adipokine levels and age, BMI, disease duration, and cerebrospinal fluid oligoclonal bands. There were also no significant differences in cytokine and adipokine levels between IIH patients regarding visual impairment. However, statistically significant differences were found between IIH patients with relapse versus healthy controls regarding IL-1β (p = 0.007), IL-8 (p = 0.001) and TNF-α (p = 0.017) levels. Other investigated cytokines and adipokines showed no significant alterations in IIH patients investigated in the remission period.
Conclusion
Altered serum levels of IL-1β, IL-8 and TNF-α seem to be associated with IIH pathogenesis, and these cytokines may be used as prognostic markers in IIH to predict relapse.
Introduction
Idiopathic intracranial hypertension (IIH), also known as pseudotumor cerebri, is a syndrome of unknown mechanism that is characterised by increased intracranial pressure without a structural brain lesion and abnormal findings in the cerebrospinal fluid (CSF) (1). The strongest and most consistent risk factors are obesity and female gender of childbearing age, and the primary presenting symptoms are headache and visual disturbances (2–5).
Many factors, such as increased CSF production, decreased CSF absorption, obstruction of dural venous sinuses and increased cerebral blood flow, have been proposed in the aetiology of IIH, but the pathophysiology of existing abnormal CSF dynamics is still unclear (4–8). Even though pressure dynamics of CSF seem to have a central role in the aetiology, the unexplained association with obesity is considered to be a pro-inflammatory state and levels of leptin, an adipokine, and certain cytokines have been demonstrated to increase in some preliminary studies of IIH patients (9–12).
Nesfatin is an interesting adipokine with recent increased awareness of its wide spectrum of central actions in stimulating the pituitary-adrenal axis and sympathetic nervous system. Also, activation of nucleobindin2 (NUCB2)/nesfatin-1 neurons in the brain by various stressors suggests that nesfatin might play a role in the adaptive response under stressful conditions (13). The involvement of nesfatin in IIH pathogenesis has never been investigated.
We aimed to investigate the levels of adipokines and cytokines to demonstrate possible markers of inflammation participating in IIH pathophysiology and to evaluate whether obesity-associated increase of adipose tissue might be modulating the clinical features and symptoms in IIH through altered adipokine and cytokine production.
Methods
Study participant selection
Thirty-nine patients diagnosed as having IIH according to revised diagnostic criteria (2) constituted the patient group. The control group was chosen from hospital staff and relatives of patients and included 40 age-, gender- and body mass index (BMI)-matched, healthy and headache-free controls without a history of central nervous system disease or admission to a physician for other medical disorders. The controls were questioned before being included in the study about current use of any medications such as steroids and immunomodulatory drugs that could potentially affect intracranial pressure and our cytokine results. Moreover, all controls underwent a thorough physical, neurological and neuro-ophthalmological examination to confirm the lack of any active disease and absence of papilledema.
IIH patients underwent analyses of complete blood count, routine biochemistry, antinuclear antibodies, homocysteine, Factor V Leiden, lupus anticoagulant, antiphospholipid antibodies, antithrombin III protein C, protein S, thyroid function tests and brain magnetic resonance imaging (MRI) and magnetic resonance venography (MRV) scans to exclude secondary causes. Detailed anamnesis including used drugs such as tetracycline and hormonal treatments were also noted and patients with secondary causes were excluded. The study was approved by the local ethics committee and written informed consent was obtained from all participants.
Clinical evaluation
A detailed medical history was recorded and neurological examination was performed in all participants by a neurologist. Patients were evaluated for age, gender, age at onset, the follow-up period, BMI, presence of papilledema, visual loss and visual field defects, CSF opening pressure, presence of oligoclonal bands (OCBs) in CSF, response to standard treatment primarily with diazomide and relapse, when present. Relapse was defined as recurrent papilledema and/or re-occurrence of symptoms due to increased intracranial pressure. Patients were treated medically and/or surgically according to their clinical needs. Regular neurological and ophthalmologic examinations were performed during follow-up of all patients.
Serum samples and handling
As daily physiological fluctuations of adipokine levels are well known, blood samples were collected from antecubital veins of all participants at 8:00 a.m. after eight hours of fasting in order to achieve standardisation. Samples were centrifuged and prepared sera were stored at −80℃ for later use. Repeated freeze/thaw cycles were avoided.
Assay procedures
Serum levels of adiponectin, interleukin (IL)-1β, IL-6, IL-8, leptin, monocyte chemotactic protein 1 (MCP-1), plasminogen activator inhibitor type-1 (PAI-1), resistin and tumour necrosis factor-alpha (TNF-α) were measured by using multiplex immunoassays (Millipore, Milliplex Map Kit). Insulin-like growth factor 1 (IGF-1), insulin, and nesfatin levels were detected using enzyme-linked immunosorbent assay (ELISA) in accordance with the manufacturer’s protocol (YH Biosearch, Shanghai, China). The levels of the cytokines and adipokines were quantified by reference to standard curves.
Statistics
The data analysis was performed using SPSS version 22 (SPSS Inc, IL, USA). Numerical data were summarised using means and standard deviation (SD). Mann–Whitney U test was used for comparison of cytokine/adipokine levels between the IIH and control groups. Associations among cytokine/adipokine levels and between cytokine/adipokine levels and demographic/clinical parameters (age, BMI, disease duration, number of relapses) were analysed by Spearman correlation test. Comparisons between clinical subgroups of IIH patients were performed using Mann–Whitney U or Kruskal–Wallis test. A p < 0.05 was considered statistically significant.
Results
Clinical features of IIH patients
The clinical features of 36 IIH patients were evaluated and three patients with new-onset IIH and papilledema were excluded for a homogenous sample in terms of disease activity.
Demographic and clinical findings of IIH and control groups.

IIH: idiopathic intracranial hypertension; BMI: body mass index; CSF: cerebrospinal fluid.
Comorbid and remarkable medical conditions in the IIH patients were as follows: hypertension (n = 4), hypothyroidism (n = 3), diabetes mellitus (n = 2), psoriasis (n = 1), ectopic pregnancy (n = 1), juvenile myoclonic epilepsy (n = 1) and bariatric surgery (n = 1). The medical histories of the other patients were unremarkable.
All patients were treated medically and two patients with visual loss and visual field defect underwent endoscopic endonasal optic canal decompression. Relapse of IIH was seen in 12 patients during their follow-up period, and seven of these patients also had visual loss or visual field defects. BMI was significantly higher in patients with visual field defects (p = 0.04).
Laboratory findings
Serum samples were collected from a total of 76 individuals.
Laboratory findings of IIH and control groups.

IIH: idiopathic intracranial hypertension; IGF-1: insulin-like growth factor 1; IL: interleukin; PAI-1: plasminogen activator inhibitor type-1; SD: standard deviation; TNF-α: tumour necrosis factor-α; MCP-1: monocyte chemotactic protein-1.
p< 0.05 was considered statistically significant.
Correlations between clinical findings and cytokine/adipokine levels
There were no statistically significant differences in cytokine and adipokine levels between IIH patients regarding visual loss and relapse status (Table 3). However, significantly higher IL-1β (p = 0.007) and significantly lower IL-8 (p = 0.001) and TNF-α (p = 0.017) levels were found in IIH patients with relapse compared to healthy controls (Figure 1).
Serum cytokine levels of idiopathic intracranial hypertension patients with relapse, without relapse and healthy controls (HC). Horizontal lines indicate median values. *p < 0.05, **p < 0.01, ***p < 0.001 by Kruskal–Wallis H test and Tukey’s post-hoc test. (Due to the broad distribution of values, logarithmic scale was used on the x-axis to allow the data to be shown in greater detail on a wide range.) IL: interleukin; TNF-α: tumour necrosis factor alpha. Laboratory findings of IIH patients regarding relapse and visual loss status. IIH: idiopathic intracranial hypertension; IGF-1: insulin-like growth factor 1; IL: interleukin; PAI-1: plasminogen activator inhibitor type-1; SD: standard deviation; TNF-α: tumour necrosis factor-α; MCP-1: monocyte chemotactic protein-1. p < 0.05 was considered statistically significant.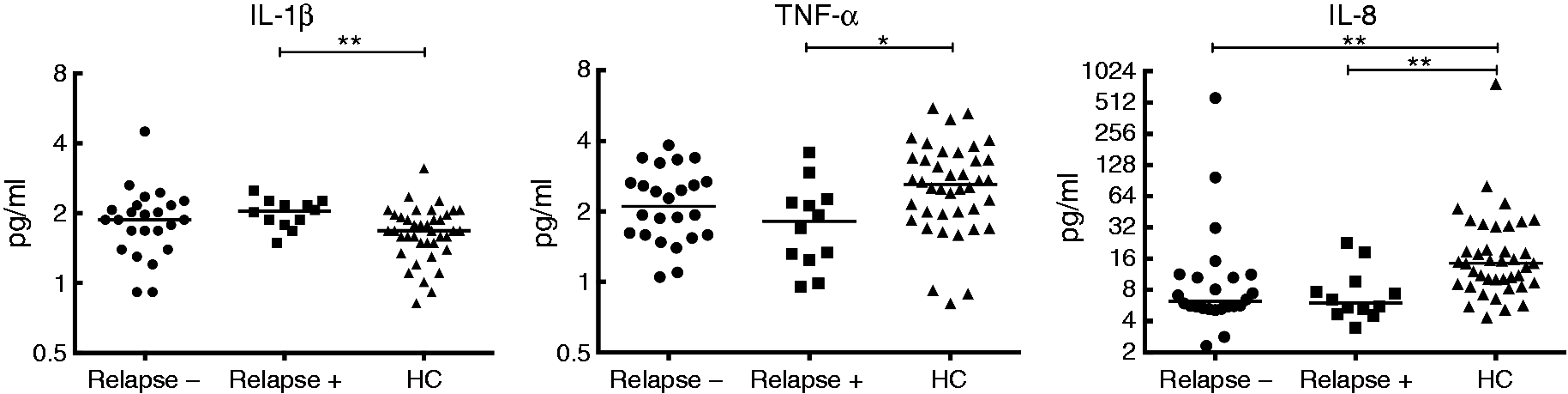

There were no correlations between cytokine/adipokine levels and age, BMI, disease duration. Likewise, there were no significant differences between cytokine/adipokine levels of IIH patients with and without CSF OCBs (in seven out of 21 investigated patients) and papilledema.
There were significant positive correlations between leptin-MCP levels (rs = 0.395, p = 0.017) and nesfatin-IGF-1 levels (rs = 0.916, p < 0.0001) in IIH patients.
Discussion
Our results showed an increase in serum levels of IL-1β in IIH patients, which indicates involvement of innate immunity in IIH pathophysiology (14). In addition, we found significantly lower levels of IL-8 and TNF-α in IIH patients with relapse. However, we failed to show significant alterations of adipokine levels of IIH patients compared to matched controls, and there were no correlations between adipokine levels and clinical features of IIH subgroups, all suggesting that inflammatory findings observed in IIH patients are not simply mediated by adipose tissue.
Various cytokines have previously been investigated in IIH patients (11,15,16). In a study by Edwards et al. (10) performed in a smaller cohort of IIH patients, serum and CSF levels of 14 different cytokines were investigated and an increase was shown in the levels of IL-2, IL-4, IL-10, IL-17 and interferon gamma (IFN-γ) compared to control groups consisting of other neurological diseases. Furthermore, we previously identified (17) anti-neuronal antibodies to uncharacterised antigens in the sera of IIH patients in rates comparable to those of encephalitis patients suggesting that inflammatory mechanisms are involved at least in some of the IIH patients. In the current study, the finding of significantly higher levels of IL-1β in the IIH group compared to the control group supports the fact that inflammatory factors may have a role in the pathogenesis of IIH. Although all cytokines investigated in our study are known to be of adipose tissue origin, the lack of correlation between BMI and levels of cytokines suggests that their levels do not depend on only adipose tissue.
TNF-α is a key component of the innate immune system such as IL-1β and IL-8 (18), and serum levels of TNF-α along with other proinflammatory cytokines are known to be elevated in obese individuals (19). Nevertheless, serum TNF-α and IL-8 levels of IIH patients were found to be paradoxically decreased as compared to overweight healthy individuals. This contradiction might be explained with differential obesity-related pathway regulation in IIH patients. In obese individuals, serum IGF-1 levels are reduced (20), whereas leptin levels are increased (21). By contrast, different from age-, gender- and BMI-matched healthy obese controls, IIH patients showed relatively reduced leptin and relatively increased IGF-1 levels, suggesting that obesity-related pathways are differentially regulated in IIH. Leptin and IGF-1 are known to enhance and suppress TNF-α and IL-8 production, respectively (22–26). Relative alteration of these factors and other TNF-α- and IL-8-related putative factors that have not been investigated in this study might have caused a cumulative impact on the levels of these two cytokines, thus causing a paradoxical reduction in their levels.
While serum leptin and CSF MCP-1 levels were found to be significantly higher in IIH patients (15), CSF leptin level was also found to be higher in IIH and no correlation was found between leptin and BMI in another study (11). Likewise serum leptin, ghrelin and insulin levels were comparable between IIH patients and obese controls (27). In a study (9) in which serum leptin levels were evaluated in obese IIH patients and obese and non-obese controls, significantly raised circulating leptin levels were found in obese women with IIH compared to both control groups. These results suggest that there may be other reasons (e.g. hypothalamic dysfunction leading to leptin resistance) affecting leptin levels besides BMI. The reason for the lack of alteration in our IIH patients, in terms of leptin and other adipokine levels might be that all of our patients were in remission and under dietary adjustments. Nevertheless, we found a positive correlation between serum leptin and MCP-1 levels. Although the correlation between leptin and MCP-1 has not been previously demonstrated, this is not an unexpected finding as both molecules have been shown to be elevated in plasma and adipose tissue of obese individuals (28).
Nesfatin-1 is a recently discovered 82-amino-acid peptide derived from NEFA/nucleobindin2 (NUCB2), localised in many tissues such as hypothalamus, brainstem and forebrain as well as peripheral adipose tissue, gastric mucosa, pancreatic endocrine beta cells, and testis (29). In several studies, exogenous nesfatin-1 was reported to inhibit nuclear factor (NF) kappa-light-chain-enhancer of activated B cells (NF-κB)-dependent inflammatory responses, lessen caspase-3-mediated neuronal cell apoptosis and maintain a balance in oxidant-antioxidant status through the augmentation of endogenous antioxidants and the inhibition of proinflammatory mediators (30,31). Furthermore, IGF-1 plays an important role in brain growth and development and is involved in repair responses both for the central and peripheral nervous system (32,33). In our study, a significant positive correlation was found between nesfatin and IGF-1 levels in IIH patients.
Regarding proinflammatory cytokine levels in IIH patients with or without relapse, the detection of higher levels of pro-inflammatory IL-8 and TNF-α in patients without relapse and IL-1β in patients with relapse suggest that chronic low-level inflammation might have a protective role in IIH. In our previous study (34), visual loss was more prevalent in IIH patients with pathological OCBs in the CSF, suggesting that optic nerve disturbance was related to inflammatory factors in addition to increased intracranial pressure. The mechanisms by which inflammation reduces neuronal damage induced by increased intracranial pressure in IIH need to be further studied. Pro-inflammatory cytokines are well known to activate multiple survival pathways and enhance proliferation capacity of endothelial and smooth muscle cells (35–38). Plausibly, mildly elevated pro-inflammatory cytokine levels might be attenuating vascular damage inflicted by increased intracranial pressure, improving nourishment of neuroaxonal structures and thus ameliorating visual disturbance. In any case, our findings indicate that proinflammatory cytokines can be used as prognostic markers in IIH.
Conclusion
This study is the first to analyse a large array of adipokines including nesfatin in IIH patients and showed significant changes in IL-1β, IL-8 and TNF-α levels in IIH patients. Although our results do not indicate a major role for the investigated adipokines in IIH, we have noted several proinflammatory markers like IL-1β, IL-8 and TNF-α are associated with relapse and thus might be used as prognostic markers. The most important limitations of our study are that all of our patients were in remission of IIH, and CSF examination could not be performed in healthy participants for ethical reasons. We believe that future studies should include CSF samples obtained during attack periods in order to illuminate the immune mechanisms involved in this puzzling disease.
Clinical implications
The altered levels of interleukin (IL)-1β, IL-8 and tumour necrosis factor-alpha (TNF-α) may support the role of inflammatory mechanisms in idiopathic intracranial hypertension (IIH). Serum levels of IL-1β, IL-8 and TNF-α may be used as prognostic markers in IIH. Adipokines such as nesfatin, adiponectin, leptin did not seem to play a major role in IIH pathophysiology.
Footnotes
Acknowledgments
The authors thank the participants for taking part in the present study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Istanbul University Scientific Research Fund (grant number BAP-53771).