
Abstract
Peripheral nerve blocks of the supraorbital, supratrochlear or occipital nerve have been utilized for the relief of headaches, although relief may be short-lasting. The purpose of this study was to evaluate the efficacy of supraorbital nerve stimulation for treatment of intractable supraorbital neuralgia. Patients presenting to the pain clinic with refractory frontal headaches who responded to a diagnostic supraorbital nerve block were selected for this case series. Patients underwent a trial of supraorbital nerve stimulation, and efficacy was assessed after 5-7 days (n = 16). From the trial, 10 patients consented to undergo permanent implantation of the stimulator. Opioid consumption and headache scores were monitored preoperatively and at timed intervals for 30 weeks. Headache scores decreased, and opioid consumption was reduced in half, and these beneficial accomplishments were maintained up to 30 weeks after implantation. In selected patients, supraorbital nerve stimulation for the treatment of chronic frontal headaches appears to be efficacious.
Introduction
Headache is a very common disease symptom with high lifetime prevalence. Most headaches such as migraine and tension-type headaches are benign (1). A plethora of pharmacological agents are used in the treatment of chronic headache. However, when most patients with chronic headache are referred to a pain specialist for treatment, most pharmacological therapy has failed and newer procedures such as peripheral nerve blocks may be initiated. The most widely used injection therapies for the treatment of chronic headache are local anaesthetic blocks of the greater and lesser occipital nerve and, less commonly, the supraorbital nerve (2).
Supraorbital neuralgia (SN) is a rarely diagnosed disease that has only recently been included in the International Headache Society classification (3). The majority of cases are post-traumatic in nature or related to entrapment neuropathy. SN is diagnosed as pain localized to the distribution of the supraorbital nerve with tenderness over its emergence or course, which is absolutely (but transiently) relieved by local anaesthetic blockade of the nerve (4). The prevalence of SN is 0.65% (5). SN can lead to chronic frontal headaches, and treatment options have not been described extensively.
Peripheral nerve stimulation (PNS) has been used to treat occipital neuralgia, although the long-term efficacy and outcome have not been demonstrated (6, 7). A retrospective report has suggested that PNS can be efficacious for the treatment of postherpetic zoster pain syndrome or post-traumatic facial pain in the distribution of the trigeminal nerve (8). We describe the use of a supraorbital PNS in a case series of patients with chronic frontal headache due to SN.
Methods
The Institutional Review Board approved the review of this case series. Patients referred to the pain centre with intractable chronic frontal and frontal-temporal headaches that were unresponsive to conventional pharmacological therapy were considered candidates for supraorbital nerve blocks after undergoing initial psychological evaluation. Comprehensive diagnostic investigations of these patients ruled out alternative headache causes, such as postherpetic neuralgia. All patients were initially evaluated and treated by neurologists and had negative magnetic resonance imaging scans of the brain. Diagnostic supraorbital and supratrochlear nerve blocks with 2 ml of 5 mg/ml bupivacaine were performed on all patients. Patients with a positive response to the diagnostic blocks had the nerve blocks repeated to confirm the response. Approximately 50 patients underwent these nerve blocks. These patients then underwent treatment with cryodenervation or pulsed radiofrequency procedure of the supraorbital and supratrochlear nerves. The duration of relief ranged from a few days to a few weeks. Current literature shows that a cryolesion provides only a temporary anaesthetic block, lasting weeks to months (9), and radiofrequency lesioning in proximity to bone often has unpredictable results (10). Patients who continued to have persistent headaches after these procedures were selected for the trial of supraorbital nerve stimulation.
Trial procedure
The trial was conducted on an out-patient basis with the patient supine and sedated. A 15-G Medtronic curved needle was used to gain access to the supraorbital groove via an entry point located at the anterior portion of the temple slightly above the orbital ridge. Caution was exercised, by maintaining a superficial position of the tunnelling tool, to avoid injury to the temporal artery, located posterior to the entry point. Fluoroscopy was used to facilitate advancement of the medial end point of the needle tip to a midline position, superior to the orbital ridge. The lead (Pisces Quad® or Octade®; Medtronic, Minneapolis, MN, USA) was threaded through the needle, which was then subsequently removed. The lead was manipulated in its medial-lateral orientation to overlap the headache pain distribution using an external screening cable and screener. Once the lead was determined to be in an optimal location, it was secured to the skin and subcutaneous tissues using a flanged anchor. Patients were evaluated for a period of 5–7 days to determine the efficacy of the stimulation. The trial electrode was removed at the time of the follow-up visit. Patients also kept a pain diary for the duration of the trial and those with at least a 50% improvement in headache score were selected for the permanent implant procedure. After the trial of the supraorbital nerve stimulator, patients were not scheduled for permanent implantation for at least 2 weeks.
Implant procedure
An Octade® lead was inserted in the supraorbital groove as in the trial procedure. Subsequently, a curved incision was made in the postauricular area and the lead secured with a flanged anchor. An infraclavicular pocket was created for the pulse generator. Using a tunnelling device, an extension was threaded from the infraclavicular pocket to the postauricular incision. The pulse generator was secured to the underlying tissues using anchoring sutures, and programmed to ensure adequacy of stimulation in the headache pain locations. Each patient was provided with a hand-held programmer to modulate stimulation.
The Octade® lead facilitates stimulation of both the supraorbital and suprathrochlear nerves. Negative amplitudes of 1–3 mA with a rate of 30–70/s and pulse width of 200–400 μs were commonly utilized. A complete description of the implantation and stimulation techniques is available from the authors.
The patient's preoperative and postoperative opioid requirements were documented. All opioid doses consumed pre- and postoperatively were converted to morphine equivalents. A discrete verbal numerical rating scale of 0–10 was used to assess the degree of headache, with 0/10 indicating no headache and 10/10 indicating the worst headache imaginable. The same headache scoring system was used for both the 5–7-day trial and the main study. Patients were followed up to 30 weeks postimplantation, and headache scores evaluated at regular intervals. Headache pain scores and opioid consumption were obtained from forms filled out by the patients at the time of their visit, before they have been seen by the nurses and physicians. Opioid consumption was analysed with paired t-test. Headache scores were analysed with repeated measures with preplanned comparison. All results are expressed as mean ±
Results
A total of 16 patients underwent a trial of supraorbital PNS, 10 (62.5%) of whom subsequently had permanent implantation of the supraorbital nerve stimulator. For these 10 patients, the visual analogue scale score before the trial was 7.28 ± 1.20 and after 5–7 days of stimulation was 1.61 ± 1.36. Among the six who did not continue, four patients reported no improvement in pain, one reported an increase in pain and one reported an improvement in pain but did not wish to pursue permanent implantation. Equal numbers of patients had received either cryodenervation or pulsed radiofrequency treatment of the supraorbital nerve prior to the trial of the supraorbital PNS. Previous antineuralgic treatment is summarized in Table 1.
Patient clinical profile

FPT, Failed pharmacological treatments; NB, nerve block; Cryo, cryolesion; RFTC, radiofrequency thermal coagulation.
The mean age of the patients who underwent permanent implantation of the supraorbital nerve stimulator was 43.0 ± 7.7 years; 60% were female. The duration of their headaches had been 10.6 ± 7.8 years (Table 1). The five patients who had failed the 5–7-day trial were 51.0 ± 11.6 years, all were female, and the mean duration of headaches was 12.3 ± 13.3 years. Headache scores were significantly reduced after implantation of the supraorbital nerve stimulator (Fig. 1), and the reduction was maintained up to 30 weeks after permanent implantation. The preimplant headache score was 7.5 ± 0.4 and at 30 weeks the pain was reduced to 3.5 ± 1.2 (P = 0.0047). The percentage of days with ≥ 50% improvement in pain scores for the overall study was 60%. The mean preoperative morphine equivalent consumed for the relief of headaches was 127.1 ± 170.1 mg/day. After implantation of the supraorbital nerve stimulator the morphine equivalent decreased to 65.7 ± 65.3 mg/day (P = 0.018) in the early postoperative period (8 weeks). At 30 weeks' follow-up the morphine equivalent required for the relief of headaches was 61.4 ± 57.6 mg/day (P = 0.019), which was significantly lower than the preoperative opioid requirements. Three patients required revision of the leads, including two due to superficial infections, both of which responded to oral antibiotics. The supraorbital electrode and the anchoring are shown in Fig. 2.
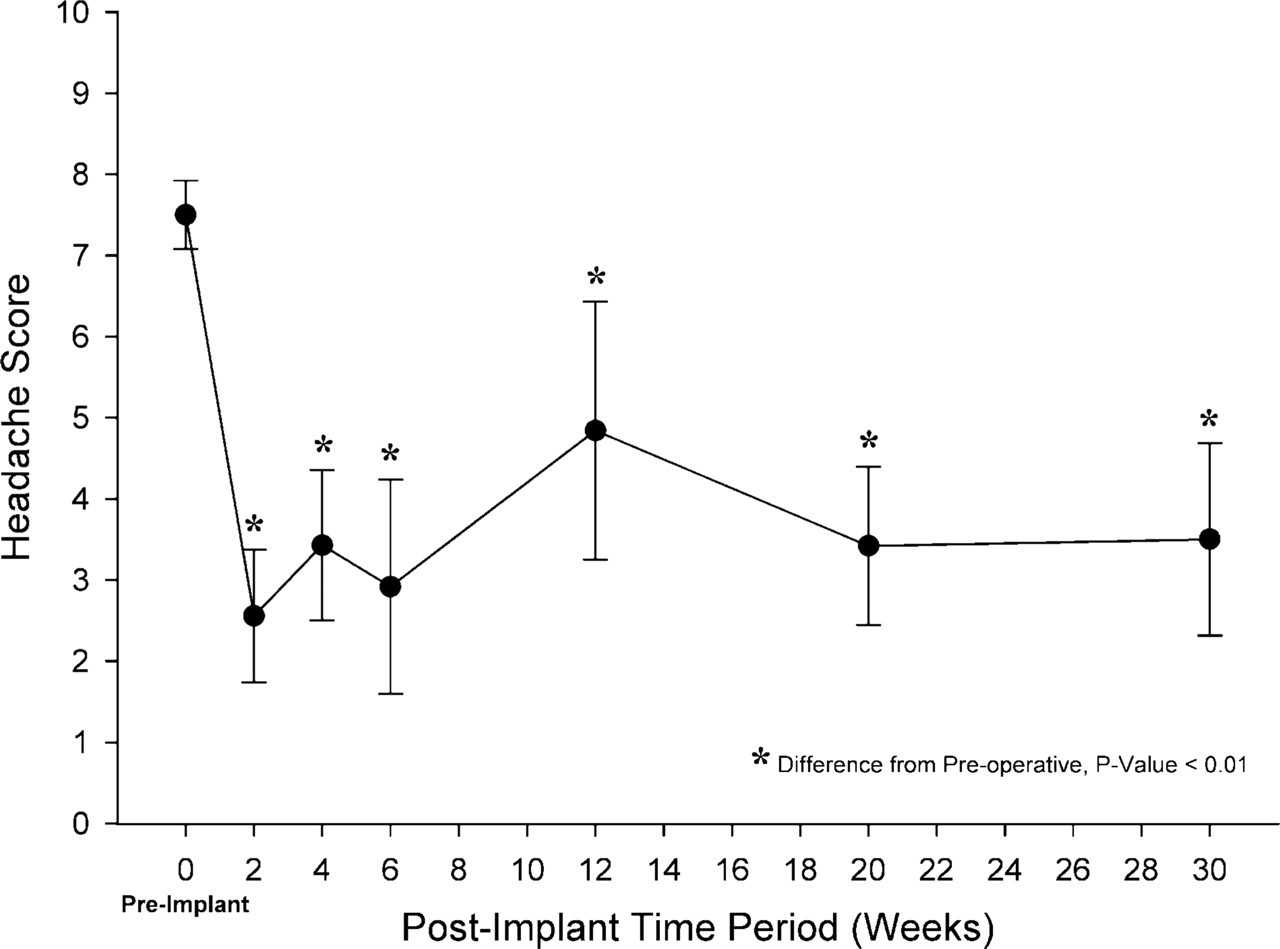
Headache score over postimplantation time of the permanent supraorbital nerve stimulator in 10 patients followed for 30 weeks. Data shown as mean ±
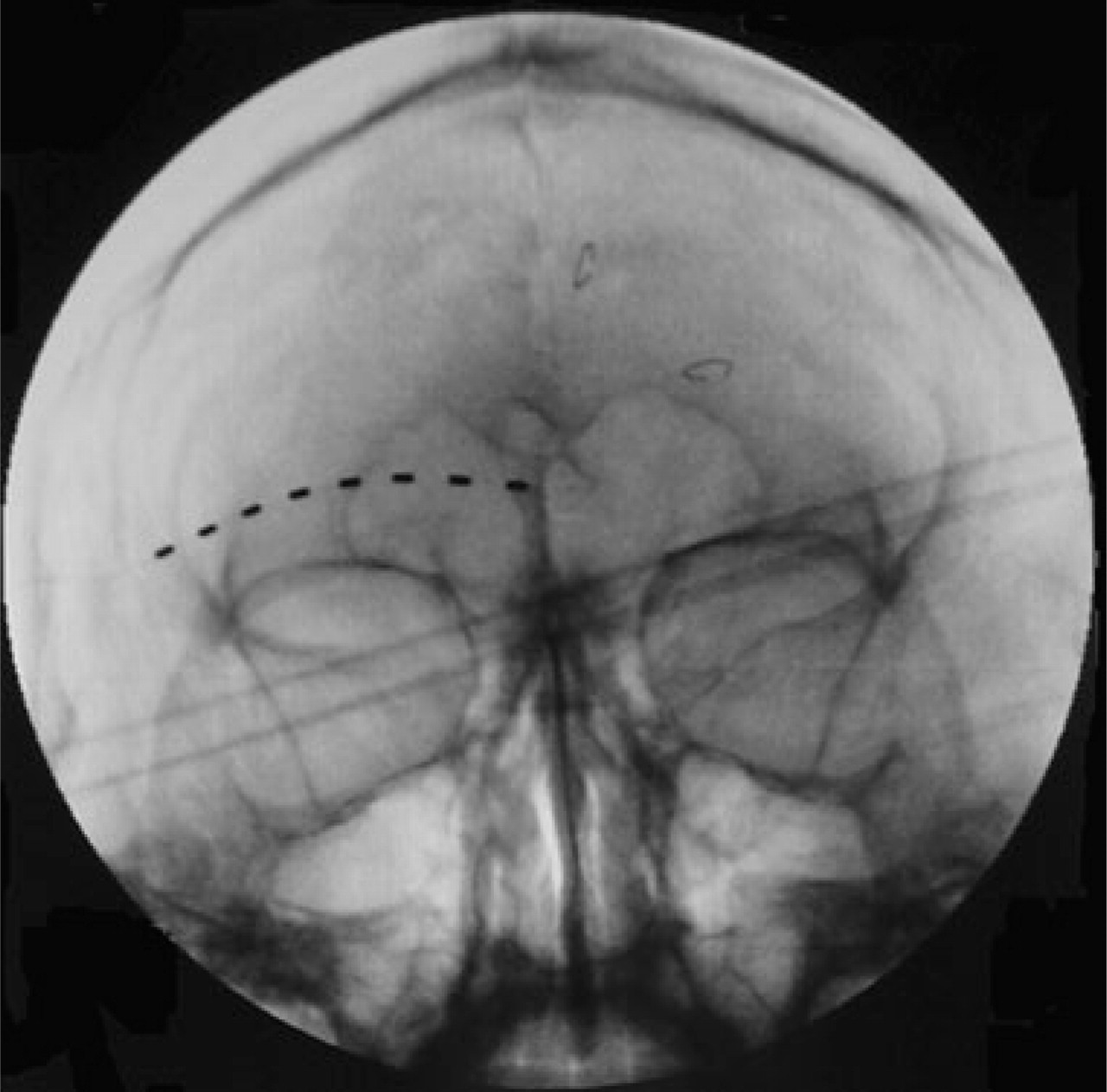
The Octade® lead placed in a patient for supraorbital neuralgia.
Discussion
This is the first case series describing supraorbital PNS for the treatment of refractory frontal headache. In selected patients, the placement of a permanent PNS in the supraorbital nerve distribution reduced headache score and opioid consumption, and the benefit was maintained up to 30 weeks postoperatively. However, there was no comparison group in this study, and so any changes in variables can only suggest a therapeutic effect.
Passage of the supraorbital nerve through the supraorbital notch and its location against the frontal bone renders the nerve sensitive to entrapment and the development of SN. In a series of 23 patients with migraine headaches, repeated (10 times) injections of local anaesthetic to the supraorbital and occipital nerves led to reduction in the migraine-type headaches (2). The effect of the repeated nerve blocks lasted for a prolonged period (> 3 months), extending well beyond the duration of the local anaesthetic effect. In another small series of patients with SN, release of the nerve surgically from soft tissue or bony excrescence has provided complete pain relief (5). Therefore, surgical exploration of the supraorbital notch is another option for patients with headaches in the supraorbital nerve distribution. However, surgical resection of the supraorbital nerve may lead to development of worsening neuropathic conditions of the face (11).
Supraorbital nerve stimulation is a relatively safe procedure in patients with SN. Due to the superficial nature of the lead and anchors, the most common complication was skin erosion and breakdown of the postauricular anchoring site. Lead migration, though a potential side-effect, was not commonly encountered. Damage to vascular structures in the head and neck were avoided by keeping the introducer needle and tunneller superficial to major vascular structures, such as the temporal artery. The infraclavicular pulse generator site needs retention sutures to prevent gravitational movement of the generator and potential tugging of the lead extension.
A complication seen in this series of patients was superficial infection, with an incidence of 20%. Although the 20% incidence is high compared with the incidence of 7% superficial and deep infection reported with vagus nerve stimulators (12), the infections in this case series were associated with the retroauricular connector and extension leads. The retroauricular connection position has been associated with higher infection rates in other surgical procedures (13). An incidence of a 30–40% complication rate has been reported for stimulators of the gasserian ganglion used for pain (14). The dermal and subcutaneous layers in the retroauricular position are generally thin and the bulky nature of the connectors used for extension wires from the electrodes probably contributes to skin breakdown.
Electrical nerve stimulation in the dorsal column of the spinal cord has been in use since 1967 (15) for the treatment of a variety of painful conditions such as complex regional pain syndrome (16), neuropathic pain, vascular diseases and lumbar radiculopathy (17). PNS is an extension of spinal cord stimulation, utilizing similar principles but addressing pain that is predominantly in the distribution of a peripheral nerve. Clinical experience with dorsal column stimulators has demonstrated that a decrease in efficacy can occur over time (18). This has not been observed with PNS, such as vagus nerve stimulators when used for the treatment of seizures (19). Similarly, when PNS was used for the treatment of trigeminal postherpetic neuralgia, efficacy was maintained up to 24 months (5). In the current series of patients, the reduction in headache pain scores and opiate use was maintained for at least 30 weeks after implantation of the PNS for refractory headaches. However, a longer-term study will be needed to determine whether these reductions are maintained beyond that time. Also, the efficacy of the procedure needs to be compared with the degree of improvement achieved with other treatments. For example, prospective, blinded, randomized clinical trials will be necessary to determine the efficacy of PNS vs. surgery as a modality of treatment for refractory SN headaches. It may also be interesting to consider PNS in properly selected patients without trial of radiofrequency lesioning or cryodenervation.
We conclude that supraorbital PNS can reduce opioid consumption and headache scores in selected patients with chronic frontal headaches related to SN.
Footnotes
Acknowledgements
Supported by University Anaesthesiologists, S.C., Rush University Medical Center, Chicago, IL, USA.