
Abstract
A 44-year-old female with gabapentin-responsive supraorbital neuralgia is presented. She had pre- and post-treatment nociceptive-specific blink reflexes carried out which tracked the good clinical outcome from treatment. The results of the electrophysiological testing imply some central component to the pathophysiology of supra-orbital neuralgia.
Introduction
Supraorbital neuralgia (SON) is a rare facial pain syndrome, characterized by attacks of unilateral pain in or above the eye, with tenderness on palpation of the supraorbital notch. Although pharmacological treatments are widely used (1–3), the International Headache Society (IHS) definition requires decompressive surgery to release bands crossing the supraorbital nerve at its point of exit through the supraorbital notch or local anaesthetic blockade (4). Recently, more cases of SON have been described (1, 2, 5) and new diagnostic criteria have been proposed (5).
We present the case of a 44-year-old woman with SON, who also had migraine which was worse perimenstrually. She declined the operative procedure and was treated with gabapentin 1800 mg daily, which was the most she could tolerate before side-effects became unbearable. This suppressed the attacks most of the time, except during her perimenstrual phase.
In order to clarify the function of the supraorbital nerve and trigeminal nerve in this condition, we performed blink reflex studies before and during gabapentin treatment.
Case
A 44-year-old female presented to our clinic with a 3-year history of right-sided periorbital pain. She began to have stabs of pain in the right supraorbital region, of sudden onset, lasting 30–60 s and having sudden offset. She would have one stab every 3 months. There was no nausea, photophobia, phonophobia, aggravation with movement or cranial autonomic symptoms. She could not trigger the attacks.
After 2 years, one evening she had five bad stabs and was left with residual tenderness. Two to three days later, she felt a pressure over the right first division of the trigeminal nerve which lasted for a few weeks. On top of the background pain, which was on a verbal rating scale of 2–3/10 in severity, she would have stabs up to 10/10 in severity. She had 10 stabs in 24 h, each lasting 30 s to 1 min. Thereafter attacks could be triggered by touching above the eyebrow to the hairline. Alcohol, sleep, lack of sleep, stress and hunger were not triggers. There was some hyperalgesia but no allodynia.
Thereafter she would have periods of 2 weeks with five stabs a day, usually at night, and 2 weeks without attacks.
She had a history of migraine from the age of 20 with generalized throbbing pain associated with nausea, aggravation with movement, phonophobia and photophobia. She would have three or four of attacks per year and they would be aggravated by her menstrual cycle.
She had carpal tunnel syndrome. There was a family history of migraine in her mother. On examination, she had hyperalgesia to pinprick over the right V1 distribution, and marked right supraorbital tenderness. Investigations included normal magnetic resonance imaging of the brain and computed tomography of the orbit and sinuses.
She had taken carbamazepine 500 mg daily, which stopped the stabs but caused cognitive problems. She was treated with gabapentin 1800 mg daily which stopped the stabs almost completely. In the perimenstrual period the supraorbital area was tender and she could trigger attacks by touch. She would have one to three of these stabs a day, each lasting less than a minute. The patient declined the offer of a local anaesthetic blockade to the supraorbital nerve, or a decompression operation. It was decided not to increase the gabapentin to try to suppress her attacks completely, as she was experiencing side-effects of weight gain and cognitive slowing. In the perimenstrual period she would take naproxen 500 mg to prevent triggering of her attacks.
Trigeminal sensation
We tested trigeminal sensation with von Frey hairs (Biotech Instruments Ltd, Illinois, USA). Sensation on the left side of the face was normal both before and after gabapentin. Sensation on the right side of the face is shown in Fig. 1.

Sensation in the face before gabapentin (a), with hyperalgesia and increased sensory threshold to 0.07 g in the right supraorbital region, and a surrounding area of reduced sensation in V1. After 3 months of gabapentin (b), the sensory threshold has improved to 0.02 g. Sensory methods are measured with von Frey hairs (Biotech Instruments Limited).
Blink reflexes
Methods
Nociceptive blink reflexes (nBR) were recorded before and 3 months after treatment with gabapentin 1800 mg daily. At both visits sensory and pain thresholds were obtained (6). We used a pair of custom-built concentric electrodes (7) to stimulate all divisions of the trigeminal nerve. Six monopolar square wave pulses were delivered at intervals of 10–20 s. Pulse duration was 0.3 ms and stimulation intensity 2.5 mA (two times pain threshold at the first visit). Muscular responses were recorded bilaterally from surface electrodes (gold-plated silver) placed infraorbitally (different electrode) and 1 cm behind the lateral corner of the eye (indifferent electrode). Sampling rate was 2.5 kHz and sweep length 150 ms (1401 ADC; Cambridge Electronic Design, Cambridge, UK). Area under the curve (AUC) of the R2 component between 27 and 87 ms was calculated off-line with custom-written software (Matlab 6.5; MathWorks, Natick, MA, USA) and used for comparison.
Results
Sensory thresholds were identical at both visits (0.4 mA). The pain threshold was 35.7% lower on the affected right side at the first visit (right 0.8 mA, left 1.4 mA) and they were identical on the second visit (0.9 mA). For AUC R2 see Fig. 2 and Table 1. On the affected side the AUC R2 of the ophthalmic division was increased by 98% compared with the ipsilateral mandibular division (contralateral: 7% less). This increase reduced to only 10% after treatment with gabapentin (contralateral: 30% less). The maxillary division was increased by 275% on the affected side and 160% on the unaffected side (after gabapentin: 172% vs. 165%).
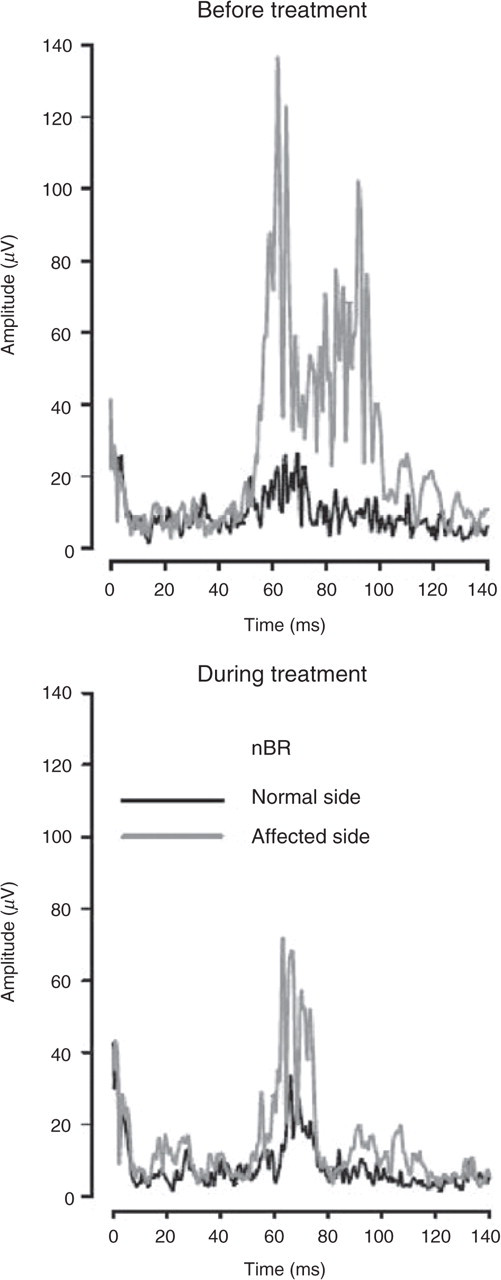
Nociception specific blink reflex (nBR) ipsilateral (affected) and contralateral (normal side) to symptomatic supraorbital neuralgia. Traces are shown before and after treatment with gabapentin. There is a marked reduction of the nBR on the pain-producing side after treatment.
Effect of gabapentin on area under the curve (AUC) of the R2 component of the nociception specific blink reflex (µV × ms)

Discussion
SON is defined by the IHS as ‘an uncommon disorder characterized by pain in the region of the supraorbital notch and medial aspect of the forehead in the area supplied by the supraorbital nerve’ (4). The results from the blink reflex study in our case imply that some central dysfunction occurs in this syndrome and illustrate the utility of objective measurement methods when studying drug effects in rare conditions.
SON has been described by Sjaastad and colleagues (1) in a series of five patients with generally unilateral pain in the forehead or ocular area and local tenderness in the supraorbital nerve. SON was further characterized in the Vågå epidemiological study, where 12 patients out of a sample population of 1828 were found to have SON (5) and further diagnostic criteria have been proposed.
Surgical exploration of five patients found tight fibrous bands crossing the supraorbital nerve; these were cut. There was an average 85% improvement in symptoms over 6 years after the decompressive surgery (1). A larger series of 18 patients who underwent repeated local anaesthetic nerve blockade had rapid and absolute relief of the pain for 1–2 h up to a few days in most patients, with three patients experiencing relief for months at a time (2). These findings would support the theory of a role for nerve entrapment in the pathophysiology of SON.
As for pharmacological measures, there has been some success with gabapentin, with relief ranging from partial to complete in six patients (2). Gabapentin is a useful drug in chronic neuropathic pain, with doses up to 3600 mg/day significantly reducing pain compared with placebo (3). Carbamazepine has a well-established beneficial effect in trigeminal neuralgia (3). In the patients with SON, carbamazepine had no effect in one patient (2), possibly a slight effect in one patient (1) and partial relief in the five others who tried carbamazepine (2). Simple analgesics had partial relief in 10/14 patients and non-steroidal anti-inflammatory drugs had a partial to excellent response in 7/13 patients (2).
In order to test trigeminal pain pathways, a concentric electrode was developed to study blink reflexes and the effect of the medullary R1 and R2 responses to head pain (7). It has been used to study sensitization of trigeminal nociception, which has been demonstrated in migraine (8) but not in sinusitis (9), suggesting that the facilitation of trigeminal nociception may be specific to migraine rather than a consequence of peripheral pain. The R2 component was increased in the affected first distribution of the trigeminal nerve and to a lesser extent also in the second distribution. This increase corresponds well with the clinical findings with von Frey hairs and the facilitation of the nBR found in migraine patients during a migraine attack (9). In our case the nBR was superior in detecting the segmental spread of the trigeminal dysregulation from the ophthalmic to the maxillary division. After treatment with gabapentin this increase was reduced, which correlated well with the clinical improvement of the patient. Gabapentin has been shown to reduce nociceptive reflexes in paroxysmal pain symptoms in multiple sclerosis (10). It is also used in the treatment of migraine (11, 12) and it is possible that in this case its effect was to reduce the sensitizing effect of migraine on the SON.
To our knowledge, this is the first case of SON which has been investigated with blink reflex studies. The results show abnormalities in both the ophthalmic and maxillary divisions on the affected side, which improved after gabapentin treatment. The fact that the abnormalities spread to areas other than that innervated by the supraorbital nerve may be due to the patient's diagnosis of migraine, which would facilitate trigeminal nociception. During migraine attacks, sensitization and cutaneous allodynia may develop and spread to sites distant to the original pain (13). This may account for our patient's increase in facial sensitivity during her perimenstrual phase and triggerability of attacks during that time.
In summary, this is a case of supraorbital neuralgia on clinical grounds, which is responsive to gabapentin. The blink reflex study shows an increase in blink reflex responses on the affected side, which improved with gabapentin treatment.