
Abstract
In a recent, hospital-based report, we described a small series of 5 patients with unilateral, more or less chronic, severe forehead pain, that could be transitorily abated by anaesthetic blockade of the supraorbital nerve and more permanently abated by ‘liberation’ operation directed towards the nerve exit area at the supraorbital notch. However, epidemiological data on supraorbital neuralgia are lacking. Among 1838 18-65-year-old inhabitants in Vågå (88.6% of the eligible ones), there were 10 who presented the following clinical picture: (1) Unilateral forehead/ocular pain, not diagnosed or diagnosable as any other, particular, unilateral headache; (2) Steadfast unilaterality; (3) Increased tenderness upon pressure over the exit site of the supraorbital nerve (incisura frontalis) on that side —in those who were in an active phase; (4) Foregoing trauma in the forehead/supraorbital rim area, ipsilaterally. In approximately half the cases, there was a moderate, ipsilateral sensory loss. A striking finding was the occurrence of jabs in the symptomatic area, and in synchrony with the neuralgia pain. These 10 inhabitants correspond to a prevalence of 0.5% (or 0.65% if two nontrauma cases are included).
Introduction
Supraorbital neuralgia (SN) is believed to be a unilateral, frontally located and supposedly rare headache. The nosologic standing of this headache has been somewhat vague. SN is thus neither mentioned in the IHS criteria nor by the IASP (1, 2). It is briefly mentioned in various textbooks in the field (3).
Two relatively recent communications may have shed some more light upon this condition:
A small series (4) was composed of five patients with a history of forehead pain, that responded positively to supraorbital nerve blockade. In one exceptional case, the symptoms were on both sides, with positive blocks bilaterally. They all underwent a ‘liberation operation’ locally at the supraorbital notch: The ligament, crossing the nerve and/or bony excrecences with an encroachment upon the nerve were removed. After a mean follow-up time of >6 years (range: 5–8 years), there was an average improvement of approximately 85% (4). The clinical picture in those responding to intervention was characterized by unilaterality without sideshift, increased tenderness over the supraorbital nerve, and relatively long-lasting and intense attacks.
A subsequent report (5) dealt with a more extensive material, 18 patients, all with positive local anaesthetic blockades. Surgical procedures were, however, not a part of the protocol. A picture of mainly unilateral, forehead headache emanated, substantiating the results in the previous series.
Both the mentioned studies (4, 5) were hospital-based studies. Little, if anything, is known about the epidemiology of SN. This will be the principal aim of the present communication.
Although the clinical picture may seem to be outlined, and therapy may be at hand for patients with major complaints, many problems remain. Tenderness over the nerve outlet zone is a sign of supraorbital nerve neuralgia. But, how specific is it? Is there a one-to-one correspondence between nerve tenderness and spontaneous attacks of SN? According to our previous experience, supraorbital nerve branches frequently are palpable in the forehead. But, how frequently can they be felt? How frequently will they be tender to touch? Does forehead supraorbital nerve tenderness correspond to tenderness at the notch – and vice versa? These questions were also focused in connection with the Vågå study.
Materials and methods
A short overview of the Vågå study
The demography and a gross design of the Vågå study have been presented previously (6). Among the 3907 individuals who lived in Vågå, there was a target group of 2074 aged 18–65 years old. All these were invited to participate in the study, and 1838 or 88.6% of them could be included.
The inhabitants were subjected to a structured interview, carried out by the principal investigator (O.S), and based on an elaborate questionnaire. The inhabitants themselves were not even allowed to see the questionnaire. Special, individual traits not infrequently necessitated deviations from the main track of questioning; the term ‘semistructured’ may therefore be an adequate characterization of the interview. A physical examination of face/head/neck was included, and so was a short- or long-version, clinical neurological examination; the latter was carried out if it seemed clinically indicated due to special circumstances. In connection with such special circumstances, also supplementary examinations, like CT or MR examinations, could be carried out.
This study falls into two parts:
Palpation and tenderness assessment of the supraorbital nerve
The supraorbital nerve was palpated along its course in 1828 inhabitants, in order to determine: whether one or more supraorbital nerve branches were palpable, bilaterally; and to determine: the supraorbital nerve tenderness level in general over the nerve branch(es) in the forehead.
Branches of the nerve can generally easily be followed from the supraorbital notch and upwards with the tip of the finger nail. Most frequently, an ascending branch, deviating towards the temporal area can be identified. Occasionally, more medially located branches can also be felt in this way. Both the examiner and the examined individual can feel when the nail passes over the nerve, generally an indolent act, but the examined individual can occasionally hear a weak sound. After a forehead branch has been identified in this way, tenderness over the nerve is assessed. This is done by direct finger pressure over the nerve branch at 90°.
At the supraorbital notch (incisura frontalis) (7), pressure is exerted onto the nerve with the volar surface of the right thumb (dominant side thumb) pointing upwards. The thumb as such is placed between the volar surfaces of the distal phalanges of fingers II & III and ‘glued’ onto them. The distal ends of fingers II & III are in their turn ‘glued’ to the skin right above the supraorbital rim. This arrangement of the test is a precaution to prevent the thumb from gliding in the direction of the eye. The tenderness was graded as – or +, or: in case it was drastically increased, as ++. Personal experience and judgement will always to some extent influence the outcome in tests of this nature. The initial force of 0.5–1.0 kg may be slowly increased up to 3–4 kg (8), but not higher, both over the notch and along the branches in the forehead.
Particular attention was paid to (a) the spreading of pain, e.g. from the notch to the forehead, to (b) any discrepancy between the pain sensations at the notch and over the nerve branches in the forehead and to (c) the duration of the discomfort, if any, and whether it outlasted the force application by more than only a couple seconds.
Similar investigations carried out over the nerve exit in our patient population over years have revealed that with the force applied over the notch and along the nerve, these structures, in our hands, generally are indolent, or: there is minor tenderness. A pain sensation at 0.5–1.0 kg would, according to previous experience, be clearly pathological. One needs to know to what extent this applies to the population at large.
The infraorbital nerve was palpated at its exit and the tenderness assessed in a similar way.
Supraorbital neuralgia
Based on previous experience (4), we would be searching for a headache characterized by a rather intense and long-lasting pain, localized in the forehead/ocular area, with unilaterality without side-shift, a headache not diagnosed or diagnosable as any well-known, unilateral headache, like cluster headache, etc. The forehead localization was a sine qua non. As for pain intensity, we had an open mind, since the individuals in question were from the population at large and not from a hospital clientele. Accordingly, cases of more mild headache not leading to consultation might be found.
The tenderness at the notch could possibly have been a free variable, provided the following triade were present: Forehead headache; unilaterality; and positive response upon supraorbital nerve blockade at the notch.
In the setting of an epidemiological study of this sort, anaesthetic blockade of the symptomatic side supraorbital nerve (4, 9) could not be carried out. Nor were ‘liberation operations’ carried out. Such treatment could in any event only have been carried out on a valid indication. A positive result of such an operation would have settled the matter, diagnostically. These shortcomings may mean that the diagnosis can not be made as definitely as desirable in putative cases.
According to previous experience (4), forehead sensory loss may be part of the picture. Ipsilateral, forehead sensory loss would, accordingly, also be taken into account, diagnostically. There should, furthermore, be a relative painlessness on palpation of the infraorbital nerve.
We therefore at this stage would largely adhere to the following triade diagnostically:
Forehead headache.
Unilaterality of the pain, without side-shift.
Tenderness of the notch area, as a sign of SN in an active phase.
Then, we used two optional criteria: Relative painlessness over the ipsilateral, infraorbital nerve. Ipsilateral, forehead epicritic sensory loss.
By combining the various diagnostic features, including the notch tenderness test, the diagnosis should be more than only suggestive, even in the absence of blockade/invasive treatment.
To which extent were the ‘tenderness-positive’ cases combined with ipsilateral, spontaneous pain? Or, the other way around: Of those with spontaneous, unilateral forehead pain attacks without an evident diagnosis, how many would have a corresponding, increased, ipsilateral, supraorbital nerve tenderness? A particular group would be those with increased tenderness, but without a headache.
One of our five previous cases had had forehead trauma (1). Inhabitants, both with and without forehead trauma were acceptable for the present study, and a distinction between them will be made.
Pain originating in the neck may spread to the forehead. For that reason, also: ‘Features indicative of cervical abnormality’ were estimated according to a special rating (8). The mean ‘feature’ in the Vågå study was 0.79+; > 2.5+ is a clearly pathological value (present in 2.3% in the Vågå study).
Headache intensity was graded from 0 to 6+ (10): 6+‘excruciatingly intense’; 5+‘severe’; 4+‘moderate’; 3+‘mild’; 2+‘heaviness’/‘discomfort’ (which is the first grade with an ailment influencing social life); 1+ minimal unpleasantness, i.e. a purely subjective experience: no influence on social behaviour; a tiny change may be noticed if the individual concentrates on the issue: unpleasantness or not? There is no procrastination. The grades ‘severe’, ‘moderate’, and ‘mild’ correspond to the same designations in the IHS system (1).
Validation studies
In the Vågå study, a routine, blinded control check of 100 records (6), was included. In this situation, identification and tenderness over the supraorbital nerve, one would not expect any variation caused by interpretation problems, but a 100% agreement. This finding will therefore not be further commented upon.
The results as regard identification and tenderness of the supraorbital nerve, in the forehead, and at the notch, respectively, as well as infraorbital nerve tenderness, have been controlled by rechecking 41–40 inhabitants, blindly, after a mean of 14.8 months (range: 4–23 months).
Results
Supraorbital nerve branches
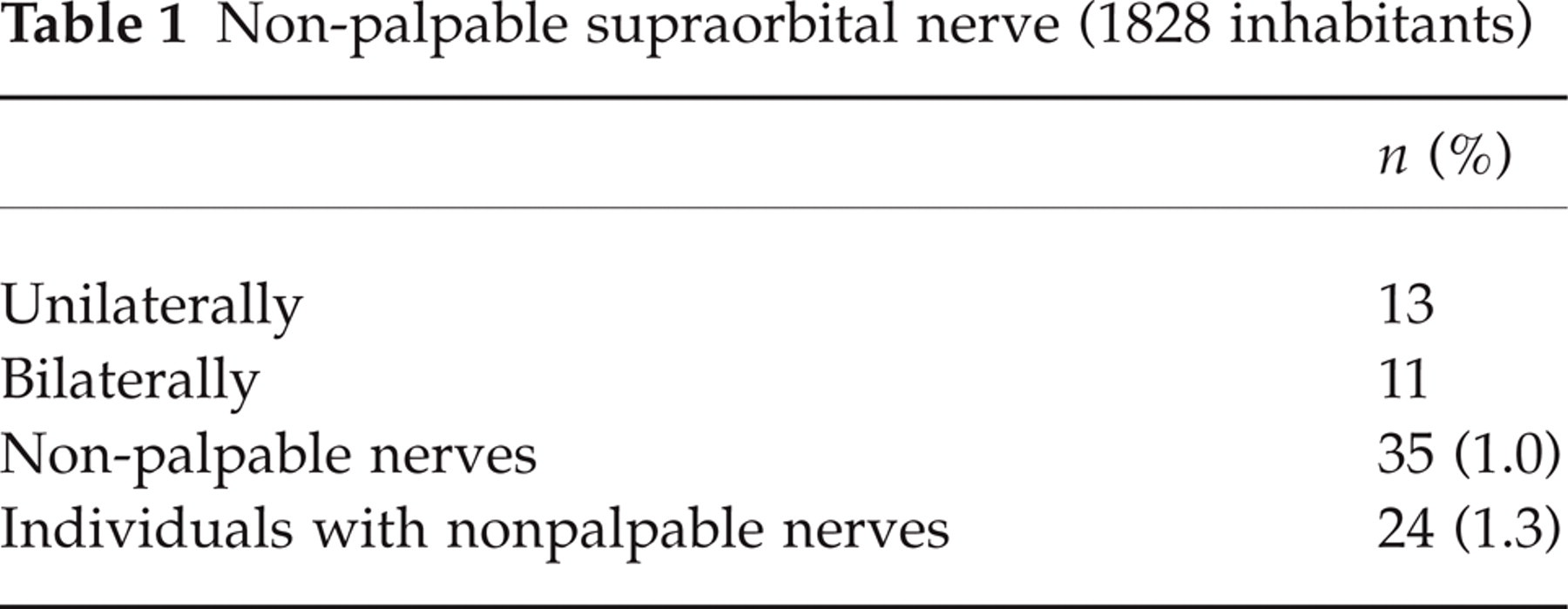
The palpable structure has the form of a string, slim (one mm thick or so), firm, noncompressible, and definitely not exhibiting the characteristics of a vessel. In all probability, this is a nerve branch. The reservations against this assumption are only minimal. And it will in this context be termed ‘nerve’. Such nerve branch(es) could not be felt in 24 individuals (1.3%) (Table 1). The nerve was, in other words, palpable in >98% of the individuals. Not surprisingly, the nerve was more frequently nonpalpable on one side than on both, the difference, nevertheless, being minor. The branch most frequently palpated may seem to correspond to the lateral supraorbital nerve branch in Becser Andersen's neuroanatomic studies (11) see also (12−14).
Non-palpable supraorbital nerve (1828 inhabitants)
Tenderness in the supraorbital notch area and infraorbitally
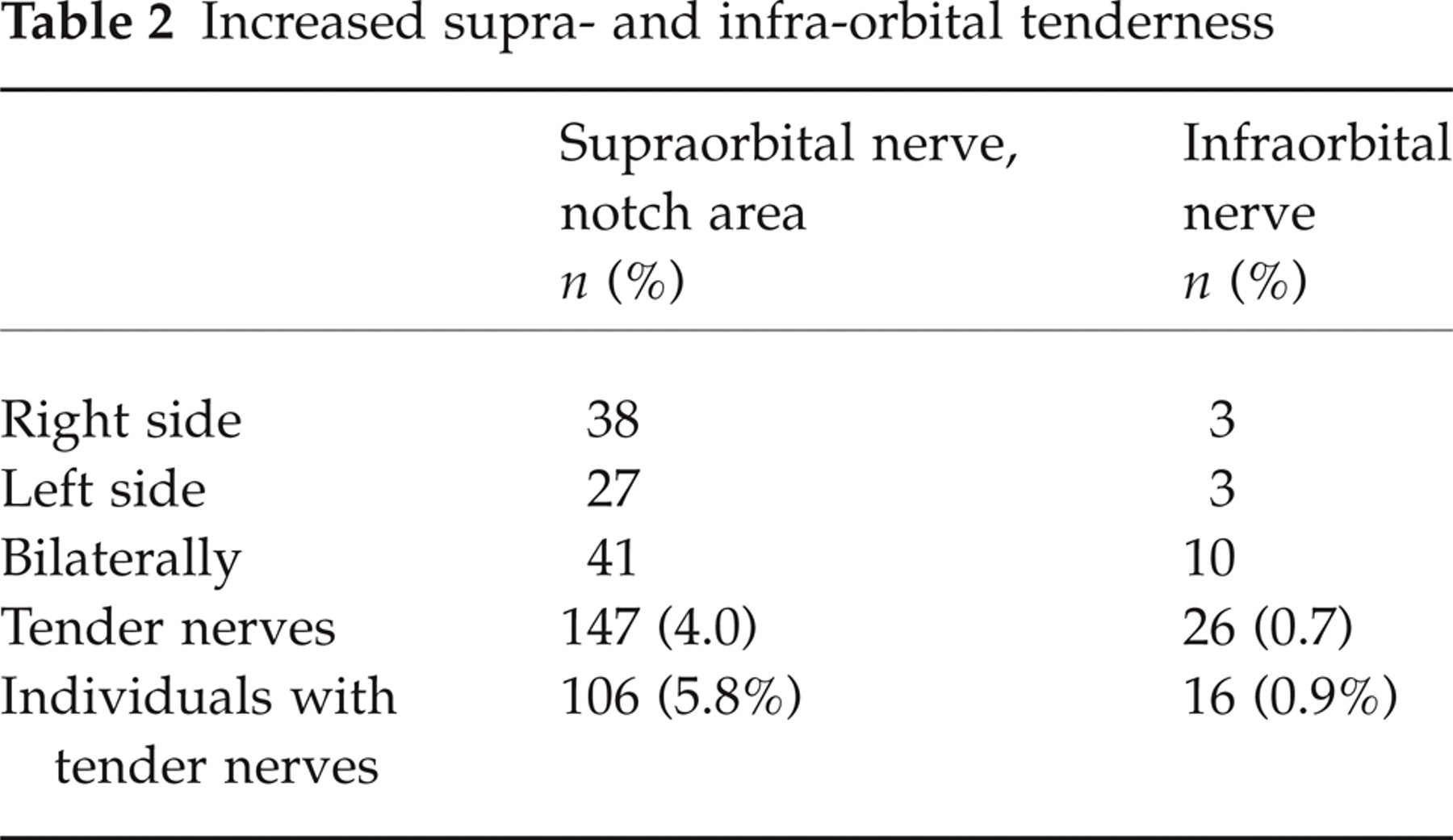
Increased tenderness over the supraorbital nerve exit was, by our standard, present in 5.8% of the inhabitants (Table 2). Tenderness was present more frequently unilaterally than bilaterally. In most of these cases, there seemed to be only a moderate increase in tenderness. Generally, the discomfort on shortlasting pressure did not outlast the stimulus by more than a few seconds. The tenderness (see below) was rather clear in those with persistent SN (Table 3) (also an inclusion criterion), and in three cases, pain radiated from the notch area to the forehead.
Increased supra- and infra-orbital tenderness
Probable supraorbital neuralgia cases
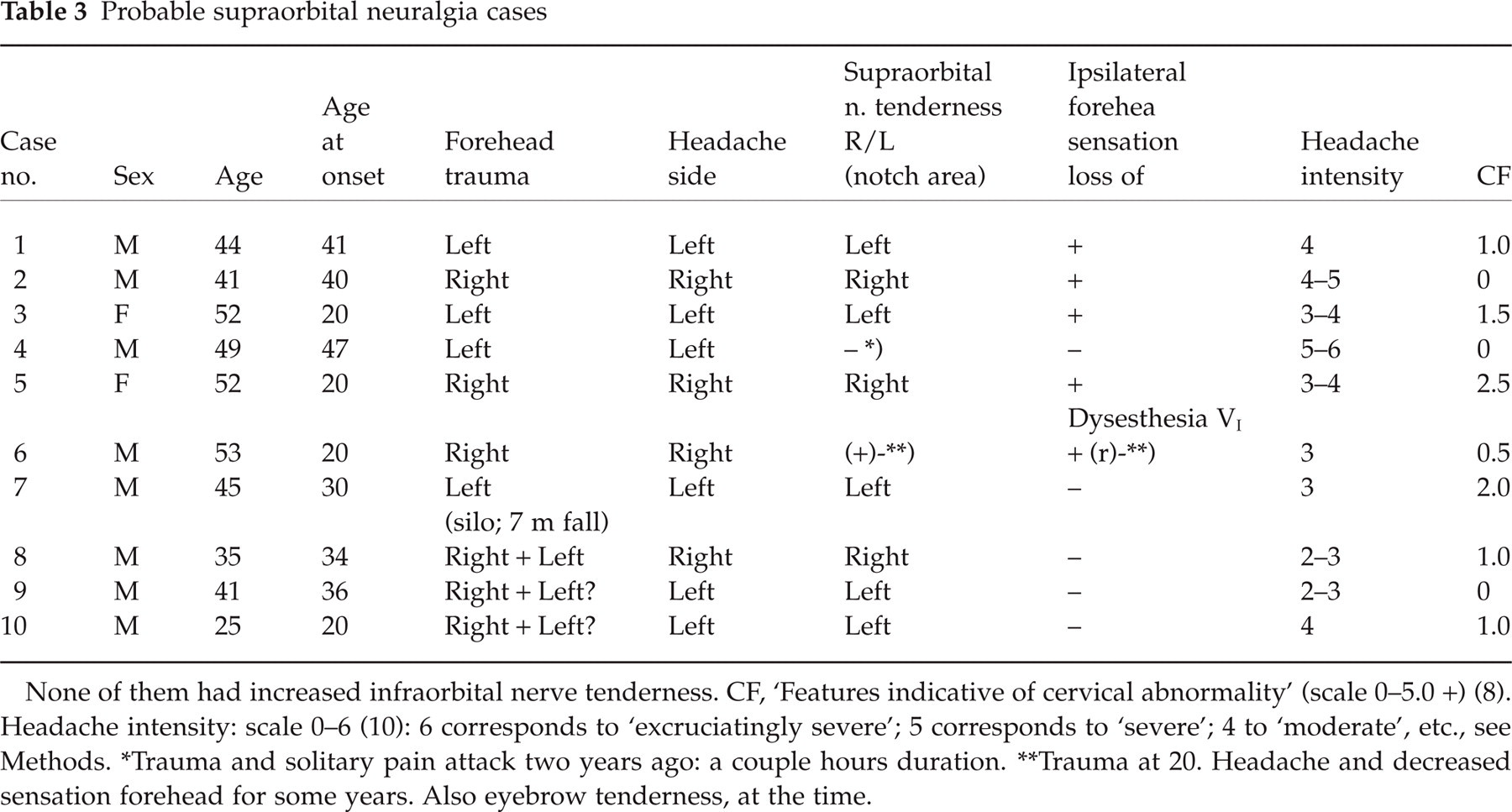
None of them had increased infraorbital nerve tenderness. CF, ‘Features indicative of cervical abnormality’ (scale 0–5.0 +) (8). Headache intensity: scale 0–6 (10): 6 corresponds to ‘excruciatingly severe’; 5 corresponds to ‘severe’; 4 to ‘moderate’, etc., see Methods.
Trauma and solitary pain attack two years ago: a couple hours duration.
Trauma at 20. Headache and decreased sensation forehead for some years. Also eyebrow tenderness, at the time.
Increased tenderness over the infraorbital nerve seemed, by our standard, to be much more rare (Table 2). In six inhabitants, bilateral supra- as well as infra-orbital tenderness was present. It goes without saying that none of these were among the 12 SN patients. It is felt that bilateral, combined tenderness of both supra- and infraorbital nerves is a delicate situation, that should dissuade the clinician from seeking strictly local causes: it may rather point to a generally increased sensitivity in the facial area.
Tenderness over the supraorbital nerve in the forehead
While increased tenderness at the notch was not a rare finding, increased tenderness over the nerve in the forehead seemed to be rare: it was present in five inhabitants. Three of them were in the supraorbital neuralgia group. In one of these, there was also radiation of the pain from pressure at the notch on the symptomatic side. Another of them without trauma, had allodynia in the anterior hair region, symptomatic side; both the notch tenderness and the allodynia were present five days after the last attack. Two nonsupraorbital neuralgia cases had increased forehead nerve tenderness combined with notch tenderness; in one of them there was radiation from the notch. Cases of questionably increased forehead tenderness have been rated as normal.
In SN, there, nevertheless, seemed to be a higher proportion of forehead tenderness, i.e. three of 12 cases, than among non-neuralgia cases, where there were two of 94, i.e. 106–12; (Table 2) (P < 0.01, Fisher's exact test).
Supraorbital neuralgia (SN)
In 12 inhabitants, a clinical SN picture, or at least a picture that we hardly could distinguish from it, seemed to be present, invariably with a strictly unilateral headache. In 10 of these 12 inhabitants, a forehead trauma antedated the headache. These 10 seem to represent a particular group (prevalence of approximately 0.5%) in the Vågå series. They will, accordingly, be treated separately; they are detailed in Table 3.
There seemed to be a fairly good temporal association between trauma and onset of headache. In one 25-year-old male with forehead traumas on several occasions between 16 to 20 years old, headache started directly upon one specific trauma (no. 10, Table 3). In one exceptional case (no. 4), the headache started on the day of a front-to-front collision, lasted two hours or so, and was excessively strong, never to reappear. In those seven with a reportedly unilateral trauma, with a wound/laceration, the headache appeared on that side. In one of the cases (no. 3), small pieces of glass, remnants from the broken windscreen, continued to be extruded from the wound area in the forehead for many years. In three cases, there may have been bilateral traumas (Table 3).
The mean age of onset was approximately 31 years, as against approximately 40 years in our first series (4). In the present series with traumas, there was a male preponderance (M/F ratio: 4.0).
The headache generally seemed to have had a favourable course, even having disappeared in four, within from one day to ‘some years’. In two, there was presently a chronic-fluctuating course (Table 4). In the remainder, there was a low attack frequency, with a possible crescendo curve only in one. The intensity mostly corresponded to 3–4+ (mild–moderate) on a 0–6+ scale (10). In one solitary case, with one solitary attack intensity seems to have been excruciating (no. 4).
Headache specifications

HA, headache; NR, nonrelevant; M-A, migraine without aura; D, days; W, weeks; M, months; Y, years; Chr.-fluct, chronic-fluctuating course.
After one (of several) traumas.
In three of them, there appeared to have been mild lacrimation and rhinorrhea during the attacks, the autonomic phenomena seemingly occurring on the symptomatic side (not shown in the tables).
Two of them had additional headache of some significance (nos. 1 & 10, Table 4). In no. 10, the migraine without aura attacks were temporally limited to childhood and early teens. The SN started immediately upon forehead trauma at 20. No. 1 had, with time, rare and mild migraine with aura attacks, apparently easily distinguishable from the post-traumatic headache, according to the patient.
Supraorbital nerve tenderness was present in all with active SN and in two with an inactive SN (cases 1 & 3). In case 4, with a solitary, a-couple-hours-long episode in the past, the supraorbital pressure test was noncontributory. One previous SN victim (no. 6) claimed that during the symptomatic years he had been tender around the eyebrow, symptomatic side (Table 3).
In half the patients, forehead sensation disturbances either had been present (no. 6) or were present at the time of examination. In one of them (no. 5), there was a sort of dysesthesia in the ocular area (Table 3). It is remarkable that in a couple of cases (nos. 1 & 3), in whom the headache had disappeared, the sensory disturbance still seemed to be present – as a scar? ‘Features indicative of cervical abnormality’ (CF) (Table 3) showed values from 0 to 2.5 + (on a 0–5.0 + scale) (8): mean 0.95+; in comparison with a mean value of 0.79+ in the unselected Vågå series. These values, on the whole, apparently are not definitely abnormal, except for the value in no. 5 which seems to be an elevated value.
In two other inhabitants, both females, not detailed in Table 3, there seemed to be a similar pain, but without any foregoing forehead trauma. In the one (no. 11), the pain story was four years; in the other (no. 12), 22 years. In both, the headache was strictly unilateral, with local tenderness at the notch. Forehead sensation was altered; in the one (no. 12) with allodynia. No. 11, in addition, had migraine with aura. In no. 11, the complaints seemed mild, in no. 12, moderate. There were some reservations against a SN diagnosis in both, in particular in no.11. In both, Hemicrania continua was an actual differential diagnosis. The altered forehead sensation counted against this alternative.
Prevalence and localization of jabs in supraorbital neuralgia
Jabs or stabbing headache (1) were present in 7 of 9 cases of SN with adequate information, i.e. 78% (Table 5). This is a significant increase when compared to jabs in the general population, i.e. 35.2% (15) (P = 0.012; Fisher's exact test). We do not have adequate data for side-shift of jabs in the population at large, but it is clear that this does happen not infrequently. In the seven SN cases with jabs, jabs seemed to appear outside the SN area in only one case of those with adequate information; in other words, jabs appeared on the pain side and in the affected area in five of six (83%) cases (Table 5). In the exceptional inhabitant (no. 4), the solitary, unilateral pain attack was of maximal severity, but lasted only a couple hours. Any regular, additional jabs at the time would hardly have been noticeable. In later years, after the discontinuation of the SN, jabs have occurred haphazardly and on both sides in this inhabitant. He has, nevertheless, been included in the deliberations around localization of jabs. The jabs in the five inhabitants with localized jabs appeared during the pain episodes (Table 5).
Jabs characteristics
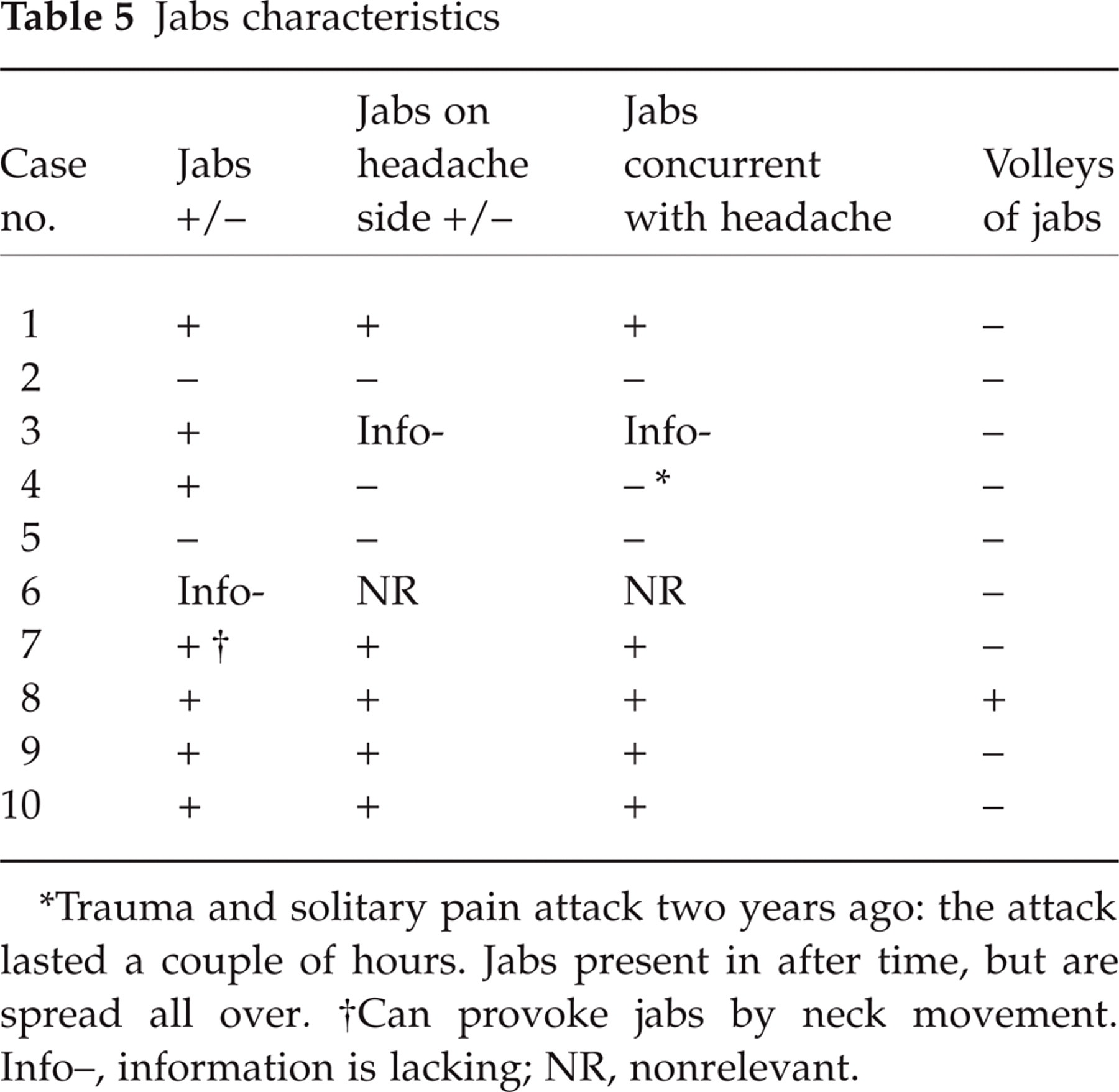
Trauma and solitary pain attack two years ago: the attack lasted a couple of hours. Jabs present in after time, but are spread all over.
Can provoke jabs by neck movement. Info–, information is lacking; NR, nonrelevant.
In the two SN cases without trauma, the one had no jabs. In the other one, the jabs occurred within the zone of the SN, but appeared both with and without the forehead pain. Although this material is a small one, there may be a slight suspicion that SN cases with and without local trauma may behave differently with regard to jabs.
Recheck of inhabitants (n = 41 ∼ 40)
In the 41 inhabitants who were rechecked blindly after a mean of 14.8 months (range: 4–23 months), the supraorbital nerves were invariably palpable bilaterally on both occasions (Table 6).
Re-examination of participants in the study (n = 41, i.e. 82 nerves; or n = 40; 80 nerves) after a mean of 14.8 months, regarding presence of supraorbital nerve on palpation and supra- and infra-orbital nerve tenderness

Statistics, 0.975; 95% CI: [0.868–0.999].
Tenderness over the supraorbital nerve, at the notch, corresponded well on the two sides on both occasions in 39 inhabitants. In one inhabitant, adequate information was lacking on the one occasion. In another one, there was tenderness at the notch – and also along the nerve on the one side – on the first occasion, but not on the second (Table 6). As regards infraorbital nerve tenderness, there was a complete consistency between the results on the two occasions (Table 6).
Discussion
Supraorbital neuralgia was recently characterized as a seemingly intense, unilateral forehead pain, without side-shift, sometimes leading to suicidal thoughts; generally, there was a chronic-fluctuating course; forehead trauma seemed to be present in only the exceptional case (4).
In the present series, there was a male/female ratio of 4.0, as against a ratio of 0.95 in the entire Vågå material (men: 895; women 942) (P = 0.06, Fisher's exact test). For comparison, in a previous series (n = 18), where trauma was present in only 28% of the cases, the male/female ratio was 0.38 (5).
The forehead trauma
Our previous report (4) stemmed from a hospital setting, with a selection of the worst cases. In the present epidemiological study, the clientele a priori could be expected to be a different one, with a milder headache and a lesser tendency to chronicity. The latter expectations seem to be fulfilled in the present study. The unilaterality without sideshift was intact. A decisive difference between the two studies was the presence of a preceding forehead trauma in the last study, in 10 (83%) of 12 cases, the trauma being either solitarily on the symptomatic side or coinvolving the nonsymptomatic side. Various traits count in favour of a decisive role of the forehead trauma in the development of neuralgia in these cases: The fact that the traumas seemed to have been major ones, e.g. case 3, where bits of glass kept being extruded through the forehead skin for years; that the trauma involved the symptomatic side; that scars could be demonstrated in the actual area; and that there was a close temporal connection between trauma and onset of pain.
While trauma was found in only 20% in our first series (4) and in 28% in another series (5), Heyck (3) mentions local trauma in addition to sinusitis as the aetiological factors. Heyck (3) emphasizes the verified case history of local trauma; the verification consisted in finding a scar and a sensibility loss. Traumatic cases may altogether differ from the ones seen in our first series (4). The trauma may be so decisive that it probably would be most proper to group such cases separately. Both aetiology and pathogenesis in the first (4) and the present series are probably at variance. The therapeutic approach may therefore be at variance as well.
An adjuvant diagnostic measure in this situation would be the supraorbital nerve blockade, and a proof would be the removal of the pain upon invasive treatment. Neither of these measures could be adhered to in an epidemiological study like the present one: in Vågå, a local anaesthesia test in general could hardly be included for practical reasons. The episodes occurred haphazardly – and were not necessarily present on the examination day. The complaints were too lenient for invasive therapy to be considered.
In specialized settings, local anaesthetic procedures belong to the armamentarium, and in special cases, invasive procedures should be considered.
The jabs
It was striking that jabs were so frequently present. The jabs seemed to be of the regular type, as far as duration is concerned, i.e. 1–3 s. This duration is the reason why we prefer the term jabs, because ‘idiopathic stabbing headache’ has been defined (by the IHS) (1) as lasting ≤ 1 second. Jabs in connection with supraorbital neuralgia have not previously been explored. In our first series (4), jabs were simply not asked about. In the present series:
Jabs were present in a high percentage of the affected individuals;
Jabs appeared on the side of the neuralgia, in other words, without side-shift;
Jabs occurred synchronously with the neuralgia. In one case, jabs apparently could be provoked, by neck movements (Table 5).
Why could not the jabs in SN in reality be trigeminal tic, specifically VI tic, since both are shortlasting paroxysms? Against such an assumption count the following observations: VI tic is an extremely rare disorder, while the ultrashort paroxysms encountered in the present context were found in seven of nine cases. The intensity of the pain would probably differ widely in the two disorders. Even though the ultrashort pain attacks had lasted for a decade or more in four of the cases (Table 3), the attacks had not spread to the other trigeminal zones, as is usually seen in trigeminal neuralgia, according to Harris (16), The mean age of onset in SN was 31 years, whereas the corresponding age in VI neuralgia cases (n = 19) was 56 years (17). All in all therefore the ultrashort paroxysms in this series in all probability are widely different from those in VI neuralgia.
The present constellations suggest a strong relationship between the jabs and the neuralgia. This close relationship may even be interpreted to indicate that they are of the same nature: Since SN in all probability has a ‘neurogenic’ and not a ‘vascular’ background, this provides evidence that jabs in this situation as well may have a neurogenic background. This may even concern jabs in general. Moreover, for what it is worth: shortlasting, neurogenic pain attacks are well known, e.g. trigeminal neuralgia; it is not well known that equally brief, cephalic, ‘vascular’ pain attacks exist.
What is the significance of nerve tenderness?
All SN patients with active neuralgia had a positive pressure test over the supraorbital incisure on the symptomatic side (inclusion criterion). However, this test seems to be highly unspecific in that it was positive, not only among the SN cases, but also in 94 other cases. So, a positive pain provocation test per se is not diagnostic. It is apparently the combination of a positive test and a typical, ipsilateral pain syndrome that counts. In our setting, i.e. without access to anaesthetic blockades, a diagnosis of SN in the absence of a positive pressure test can hardly be made with the present level of insight.
Forehead tenderness was a rare phenomenon (n = 5). It was, nevertheless, much more frequently present in the notch-palpation-test positive cases with neuralgia (three of 12) than in notch-tenderness positive cases without neuralgia (two of 94). Based on the assumption that the diagnosis of SN be correct in our cases, the following reasoning may be pertinent: Since most SN patients had a negative forehead nerve tenderness test, lack of forehead tenderness over an identified nerve branch can not be used as an exclusion criterion. On the other hand, the combination of symptomatic side forehead and notch tenderness may strengthen the diagnosis. If a positive forehead pain test were put up as a diagnostic sign, one would have to change the criteria for SN.
In cases with a clear forehead trauma and still clinically active SN, one will at times be faced with the combination: supraorbital notch tenderness, but no definitely increased forehead tenderness. To promote further development and understanding in this field, future patients with forehead trauma should be exposed to separate nerve blockades both at the notch and along the nerve branches in the forehead, at different times.
Differential diagnosis and diagnosis
Trigeminal neuralgia and SN may appear in the same area. Generally, however, SN attacks are much more long-lasting than VI neuralgia attacks. The following features will also discriminate between them: 1. The intensity (except in case 4, Table 3) seemed to be less in SN with trauma than what one would expect in VI neuralgia (2). The forehead is a rare location for trigeminal neuralgia (3). There were few and mild autonomic symptoms and signs among SN cases.
More long-lasting SN pain episodes may be mixed up with Hemicrania continua. The fact that specific drugs for the mentioned disorders, carbamazepine and indomethacin, have not been tried in this variant, does only marginally affect this reasoning (tried in no-trauma cases) (4). Criterion no. 4, and possibly also nos. 6 & 8 (Table 7) probably count against both Hemicrania continua and trigeminal neuralgia.
Diagnostic criteria: a proposal
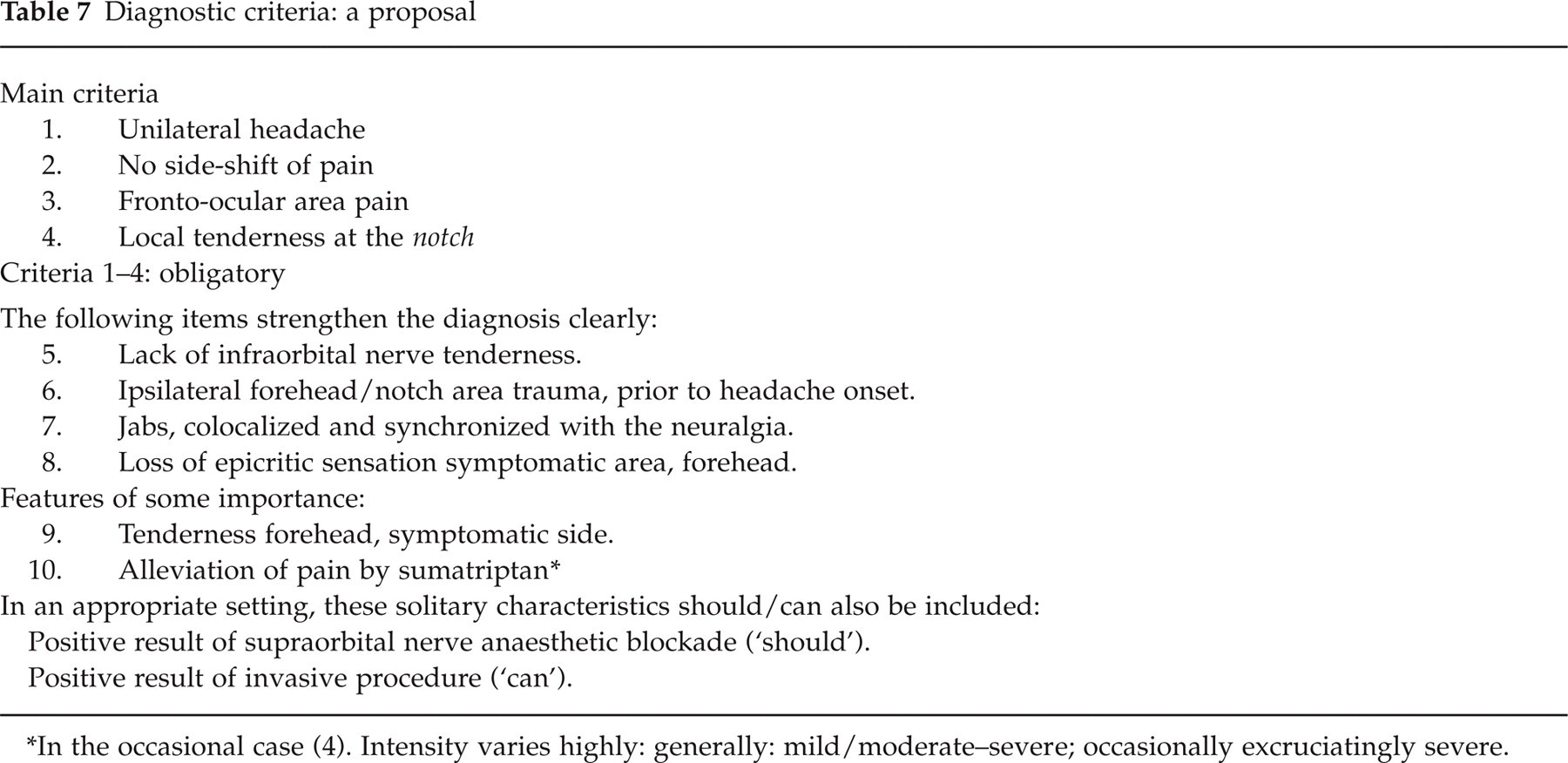
In the occasional case (4). Intensity varies highly: generally: mild/moderate–severe; occasionally excruciatingly severe.
Since anaesthetic blockades have not been carried out, was then the diagnostic work-up adequate? The criteria, as we see them now, are set out in Table 7. All the four main criteria were present in our cases, the exception being no. 4, with the excruciating, one-time episode two years before, and where the notch tenderness presently was lacking. The diagnosis was, nevertheless, considered likely in no. 4. Local trauma is an important diagnostic event, which, when present, may be decisive. It has, however, previously been demonstrated (4, 5) that there may be genuine SN cases without trauma, and such cases are also part of the present communication. Tenderness over the supraorbital nerve in the forehead is not, by far, a sine qua non; but, when present, it renders ample support for the diagnosis. The other way around, there are forehead supraorbital nerve pressure positive cases without a SN. Diagnostically, it is therefore probably correct to start with a unilateral forehead/ocular pain and from there on try to disentangle the problem. To start with increased notch tenderness, which is a not infrequent finding, would probably be awkward. A local, sensory loss is also important. Furthermore, seven of nine sufferers had jabs, and in five of six with adequate information, the jabs were in the stigmatized area, on the symptomatic side. When combining the various features (from Table 7), the diagnosis may probably be made with reasonable certainty.
Footnotes
Acknowledgements
We are indebted to GlaxoSmithKline of Norway, Pharmacia & Upjohn, and the Alf Harborg Foundation, Department of Neurology, St. Olavs. Hospital, Trondheim, Trondheim University Hospitals, for generous support during the various phases of the investigation. The authors are also grateful to the personnel at the Vågå Health Centre at Vågåmo for their aid. Last, but not least, we thank the inhabitants of the Vågå commune for their collaboration.