
Abstract
A series of 18 patients suffering from supraorbital neuralgia have been studied through a seven year period. Appropriate investigations ruled out other headaches.
There was a female (67%) preponderance. Mean age at onset was 51.6 years. The mean headache duration was 5.9 years. Five patients had a history of ipsilateral forehead trauma. The main areas of pain were the forehead and orbit. The pain was dull with short sharp or burning exacerbations. The temporal pattern was either remitting (n = 7) or chronic continuous (n = 11). Autonomic accompaniments were generally lacking. Neurological assessment was normal in all but 4 patients who were found to have signs/symptoms of sensory dysfunction in the forehead of the symptomatic side. Trials of different drugs, including migraine and anti-neuralgic drugs, only provided slight relief. Anaesthetic nerve blocks of the supraorbital nerve provided an absolute but transitory relief of pain.
Although aetiology and pathogenesis of supraorbital neuralgia is largely unknown, entrapment of the supraorbital nerve at its outlet and successful decompressive surgery have been previously reported. This and other pathogenic hypotheses are discussed.
Introduction
According to the IASP (1) neuralgia is pain felt in the distribution of a nerve or a nerve root. Supraorbital neuralgia (SN) is pain localized to the territory of the supraorbital nerve with tenderness over its emergence or course, which is absolutely – but transitory – relieved by anaesthetic blockade of the nerve (2). This clear-cut clinical triad has been proposed as diagnostically crucial in SN (2). This headache category is neither included in the current classifications of the IHS (3) nor the IASP (1) probably due to the scarcity of reports.
We have endeavoured to study a substantial number of patients suffering from SN as defined by the abovementioned triad (2). This may strengthen previous knowledge and may add new perspectives on the clinical manifestations and possible therapeutic approach of such a distinctive headache.
Patient series and methods
Eighteen patients (12 females and 6 males) suffering from SN have been studied through a 7-year period. The patients belonged to the same health regional area of 180000 inhabitants covered by Hospital Na Sa de Sonsoles in Avila (Spain). Demographic data of the patients are set forth in Table 1. All the patients fulfilled the triad of protracted unilateral, forehead/ocular pain, tenderness over the supraorbital nerve and absolute alleviation of pain upon repeated blocks of the nerve (2). In addition, an exhaustive diagnostic search for other primary and secondary headaches was negative. All the patients were examined by the authors and most of them also by an Ophthalmologist. Eye examination systematically included intraocular pressure.
Demographic data

M, male; F, female; R, right; L, left;
She suffered from migraine during her youth and episodic tensional headache since she was 40.
Details on previous head trauma are provided in the text.
Supplementary examinations such as CT scan of the head and orbit, brain MRI, orbit, skull and facial X-ray, routine blood (including ESR) and urine analyses were carried out in all the patients.
Anaesthetic blocks were performed with a 1 cc syringe with a 29G × ½′′ disposable gauge and 0.33 × 12 mm inch needle. The anaesthetic agent used was mepivacaine clorhydrate 2%. Total injected volume was 0.5–1 cc. Three patients (nos. 1, 6 and 16) also received placebo (0.9% saline solution) injections on two occasions each.
The anaesthetic injections were given around and immediately above the palpable supraorbital notch, 20–30 mm from the midline. We did not vary the site of injection in successive trials; so, patients who did not respond with absolute pain relief in this particular point of injection, were excluded from this clinical study. For the last block of patients nos. 6, 8 and 16 we used a mixture of mepivacaine clorhydrate and betamethasone in an intent to provide them with a more sustained relief.
Results
There was clear female (67%) preponderance. Mean age at onset was 51.6 years (range: 21–80), and the mean headache duration was 5.9 years (range 1–37 years). Five (28%) patients had a history of forehead trauma on the symptomatic side. Patients no. 7, 13, 14, 15 had a moderate trauma with forehead contusion shortly before (1–15 days) the onset of symptoms. One particular patient (no. 12) had a severe multiple trauma (36 years before the onset of symptoms) with intracranial bilateral frontal haemorrhagic contusion that further developed into a porencephalic cavity in the right frontal lobe and a gliotic scar in the left frontal lobe. Later on this patient presented a bilateral (left-sided predominant) fronto-ethmoidal encephalocele. Remarkable antecedents of all the patients are shown in Table 1.
The main areas of pain were the forehead and orbit (Table 2). The right side was affected in 10 patients whereas the headache was left-sided in 6 patients. One exceptional patient (no. 9) complained of bilateral but asymmetric forehead pain in that at pain maxima, a low-degree pain might occasionally be felt in the opposite supraorbital area. In this particular patient, block of the most painful side (the right one) elicited bilateral pain relief. Other patient (no. 5) suffered from a bilateral SN: he first developed a left SN and after some months, he developed a right SN. Each neuralgia did independently respond to the block of the respective symptomatic nerve.
Pain characteristics

symptomatic periods C, Chronic; E, Episodic; NA: not available.
The pain was generally dull and constrictive. In addition, sharp, piercing or burning exacerbations, lasting from minutes to hours were reported by 50% (9 out of 18) of the patients (Table 2).
According to a 5-point headache severity scale (0 = none; 1 = mild; 2 = moderate; 3 = severe; 4 = intolerable) pain was scored as mild-moderate (n = 10), severe (n = 14) or intolerable pain (n = 5) (Table 2). Patients no. 1 and 8 had even suicidal thoughts.
The temporal pattern at onset was remitting in 7 patients with symptoms lasting from several days to a few months. During symptomatic days the patients were in pain most of the time. Transitions from episodic to chronic pattern were witnessed in 3 patients, with a latency of > 3 months of disease. A chronic-continuous pattern since the onset of symptoms was observed in 11 patients, and remained as such in all but two patients (nos. 5 and 11) in whom a transition from the chronic to the remitting stage was witnessed. Therefore, the prevailing temporal pattern in most patients (n = 12) was either primarily or secondarily chronic.
In most patients there were no noticeable precipitating mechanisms. Generally alcohol, cervical and facial movements as well as routine physical activities neither triggered nor increased pain. Patient no. 7 reported that he could trigger attacks by applying a longlasting and strong pressure over the supraciliar region. Patient no. 16 could trigger the frontal pain with the application of local tactile stimuli over the ipsilateral forehead.
Both general (e.g. nausea, vomiting) and local (e.g. conjunctival injection, lacrimation, nasal stuffiness/rhinorrhea) autonomic accompaniments were generally lacking. When specifically asked nine patients thought that very rarely the most severe attacks could have a variable combination of accompaniments (Table 3) but that they were of modest dimension. Even in these patients the vast majority (> 95%) of attacks were oligosymptomatic. It should be mentioned that we have frequently observed all the patients during symptomatic periods and in none of them autonomic accompaniments were noticed.
Autonomic phenomena
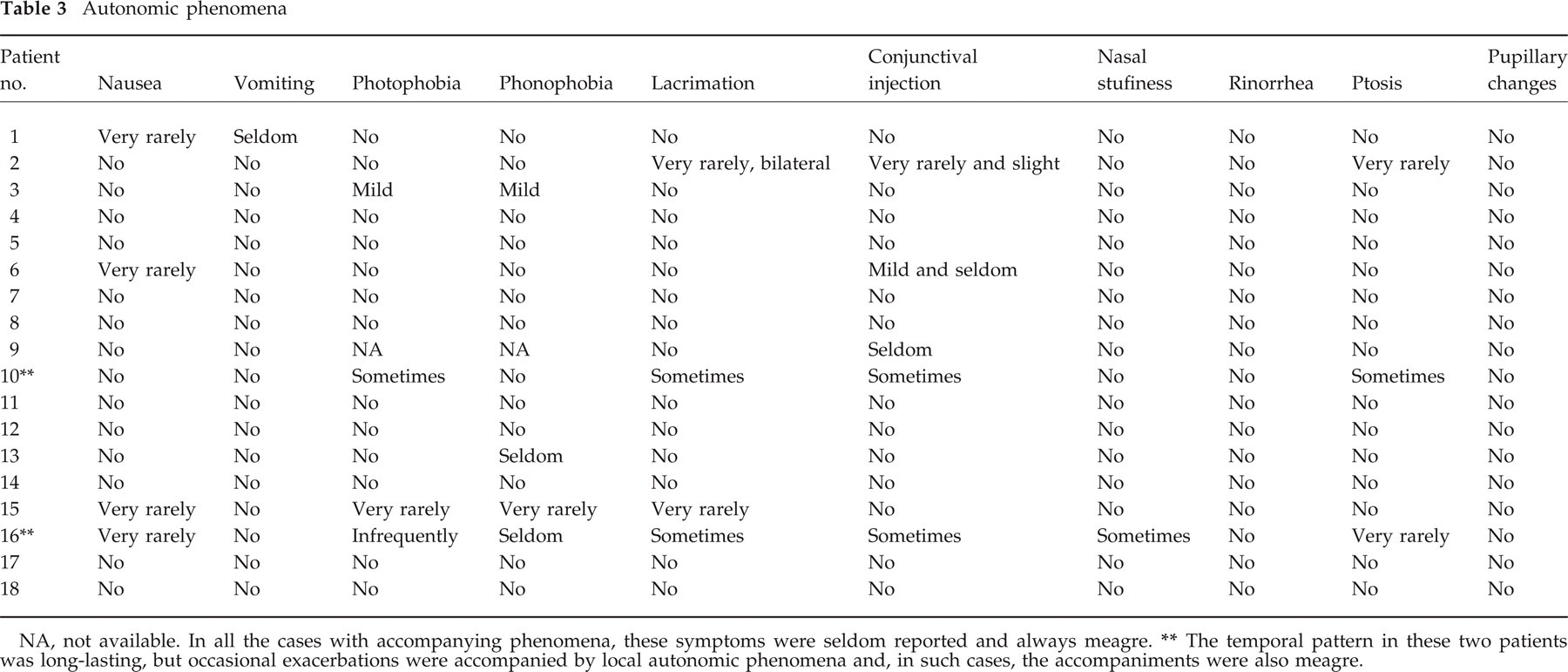
NA, not available. In all the cases with accompanying phenomena, these symptoms were seldom reported and always meagre.
The temporal pattern in these two patients was long-lasting, but occasional exacerbations were accompanied by local autonomic phenomena and, in such cases, the accompaniments were also meagre.
Neurological examination systematically showed considerable pain or tenderness elicited by pressure on the ipsilateral supraorbital nerve outlet in all the patients. Contralateral tenderness was also elicited in patients no. 9 and 12. Patients no. 12 and 16 who reported forehead paresthesias were found to have hypoesthesia in the symptomatic area. Patient no. 7 had hypoesthesia without paresthesias in the symptomatic forehead whereas patient no. 15 had the opposite findings (Table 2). If tested with sensitive methods, a ‘subclinical’ deficiency in the territory of the supraorbital nerve might have been unveiled in more, possibly all, patients.
Supplementary examinations such as CT scan of the head, brain MRI, orbit, skull and facial X-ray, routine blood (including ESR) and urine analysis were all normal or without relevant abnormalities.
No available pharmacological treatment was found (Table 4), and particularly Amitriptyline (n = 14) carbamazepine (CBZ) (n = 6), ergotamine (n = 5), triptans (n = 7) and Indomethacin (150 mg/day) and other NSAIDs (n = 13) were all of no avail or induced only a slight/moderate beneficial effect. There were some exceptions; CBZ induced a substantial alleviation of pain in patient no. 1, ergotamine in patient no. 2, triptans in patients no. 2 and 8 and indomethacin in patients no. 2 and 11. Gabapentin was tried in 6 patients with partial but substantial relief, transforming a severe or intolerable pain to moderate; patients no. 15 and 17 had an important relief and a transformation of a chronic pain into an episodic and intermittent pain.
Drugs and nerve blockade effects
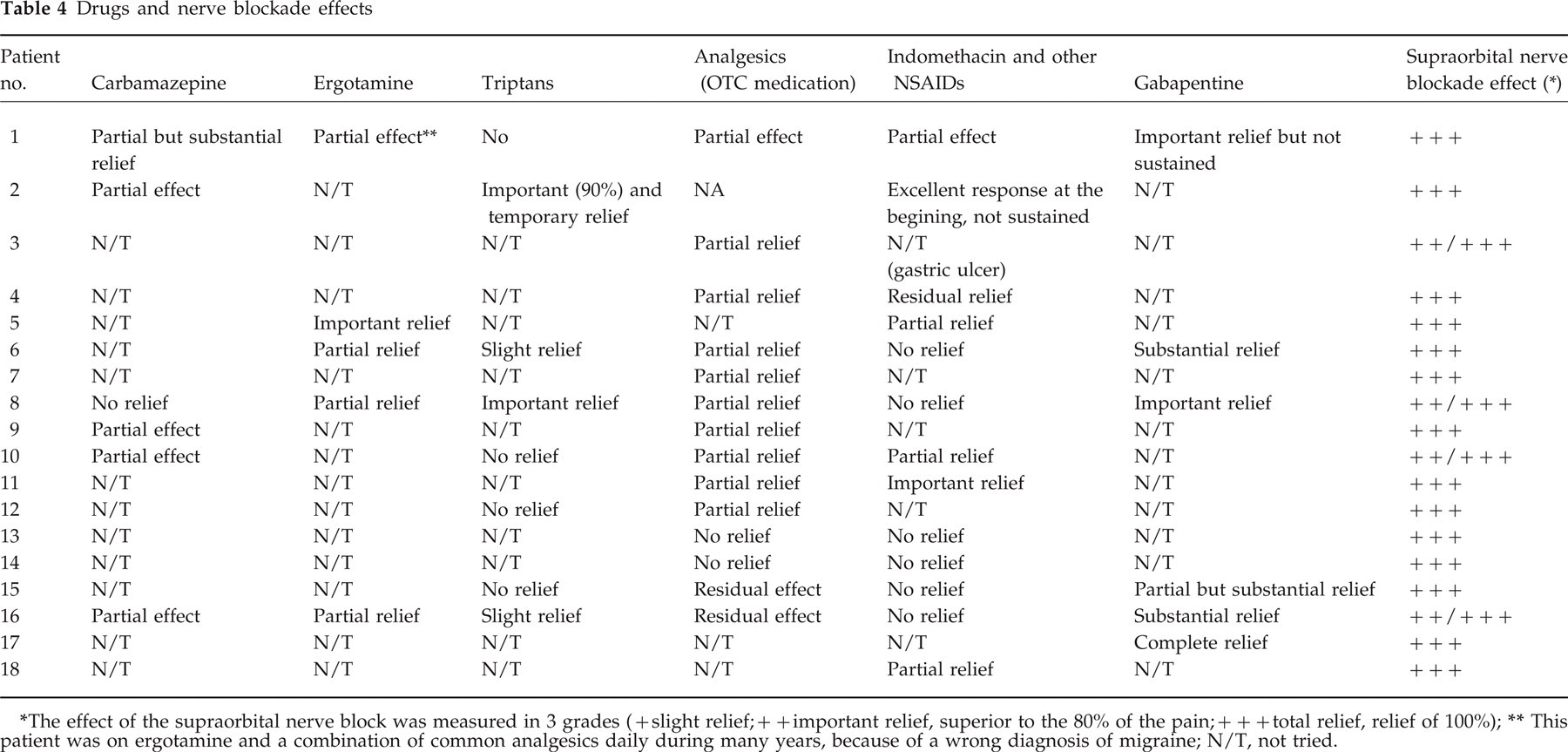
The effect of the supraorbital nerve block was measured in 3 grades (+ slight relief; + + important relief, superior to the 80% of the pain; + + + total relief, relief of 100%);
This patient was on ergotamine and a combination of common analgesics daily during many years, because of a wrong diagnosis of migraine; N/T, not tried.
Repeated (generally 3–4) anaesthetic blocks of the supraorbital nerve systematically provided rapid and absolute relief of pain that usually lasted from 1 to 2 h to several days. In three patients (nos. 3, 4, 9) pain relief after blockade was longlasting (4, 1 and 2 months, respectively). In patients no. 6, 8 and 16 the local injection of a mixture of mepivacaine and betamethasone did not prolong the temporal remission compared to the anaesthetic alone. The three patients treated with 2 placebo injections each obtained only a residual (< 10% improvement) and very short-lasting (a few minutes) relief.
Some patients have been lost to follow up (nos. 3, 4, 9, 10, 11 and 12). Patient no. 12 died some months after developing the SN because of a huge cerebral frontal abscess. Some patients do quite well while on gabapentine (except patient no.1, whose reponse was only transitory), whereas others denied recommended treatments and have resigned to keep on common analgesics.
We had neither access to surgical exploration of the supraorbital notch nor surgical treatment with the procedure described by Sjaastad et al. (2).
Discussion
Appart from the confinement of the pain to the territory of a given nerve, the promotion of symptoms by stimulation of the nerve together with their abolition after local anaesthesia have been claimed as essential features of neuralgias (2, 4). In any region of the organism involved in a painful process, local palpable large nerves and surrounding tissues, may be tender independently of the underlying disorder (5). However, tenderness is much greater whenever the source of the pain is precisely the palpated estructure, e.g. the nerve. Assessment of tenderness depends on the personal experience of the attending physicians who become skilled in such matter over time.
Both supraorbital and supratrochlear nerves are superficially lying between the skin and the frontal bone. Considerable anatomical variations on the course of both nerves have been noted (6–9). Therefore, when performing anaesthetic blocks it is important to ascertain which nerve has been successfully blocked. In our patients, the supraorbital nerve was the target of the blockades which systematically provided complete relief of pain. Nevertheless, we can not absolutely rule out whether the anaesthetic agent could have also reached the supratrochlear nerve. Whether supratrochlear nerve may also be partially responsible for the symptoms remains to be clarified. Anatomical variations may also be the reason why repeated anaesthetic blocks may not invariably lead to a transitory discontinuation of the pain in particular patients who may therefore remain underdiagnosed. Both refinement of the blockade procedure and development of sensitive techniques to in vivo identify the exact position and course of both nerves, may unravel such a problem. Accordingly, we so far prefer the conservative term supraorbital neuralgia instead of neuralgia of the supraorbital nerve.
A rather persistent temporal pattern is observed in other painful syndromes supposedly originated in a nerve or a nerve root such as in postherpetic neuralgia. Conversely, paroxysmal, lightning pain can be originated in the CNS, such as, e.g. tabetic crisis. Therefore, the concept of neuralgia should rely upon topographical considerations (i.e. pain felt in the distribution of a nerve or a nerve root) rather than in the temporal aspects of the pain. This is in agreement with the prevailing concept that painful syndromes should be better classified according to their localization (IASP) (1).
Entrapment mechanism might play a role in SN as in other different facial neuralgias (10). The passage of the supraorbital nerve through the supraorbital notch and location against the frontal bone may render it susceptible to injury (2, 11). In the small patients series with SN who underwent ‘liberation’ operations (2), a compressing factor such as a soft tissue band or bony excrescence was identified, and removed, providing complete and long lasting relief of the pain. According with these findings a surgical exploration of the supraorbital notch seems to be indicated in patients suspected of having SN.
The supraorbital nerve and, less frequently, supratrochlear nerves also may be affected by externally applied moderate pressure on the forehead, such in tightly worn swimming goggles (‘goggle headache’) (12) or by anaesthesia mask (11). There is a considerable number of patients with previous forehead trauma that could account for further development of SN. After leaving the supraorbital notch, the supraorbital nerve is vulnerable to traumatic injury. In some postraumatic cases, the pain starts immediately after the injury, meaning a direct trauma to the nerve. In other cases, neuralgic pain began after a latent interval of several weeks or months; in these latter situations, we could speculate that supraorbital nerve may be involved in slowly developed local fibrosis or neuroma degeneration.
We (unpublished observations) and others (13) have previously demonstrated that blocks of the supraorbital nerve during attacks in patients suffering from regular migraine attacks provide residual alleviation of the pain only in the anaesthesized area, i.e. without resolution of the ensuing attack. None of our patients fulfilled the IHS diagnostic criteria for migraine (3). In particular, none reported pulsatile tinge of the pain neither worsening of the pain by routine physical activities; only some patients rarely reported nausea, vomiting or photophonophobia and even in such cases these accompaniments were of modest dimension; In addition, the temporal pattern exceeded by far the upper limit of the regular migraine attacks.
In our patients, generally, migraine drugs such as triptans and ergotamine did not provide relief. Only two patients had a good response to sumatriptan and one of them to ergotamine. It has previously been reported that triptans may be of help in relieving SN (2). Our experience indicates that a very minority of SN patients did respond to triptans. This is in agreement to the prevailing concept that triptans are powerful vasoconstrictors so it is not expected for a presumably neuralgic pain to respond to such a treatment. However, the supraorbital artery is also passing through the supraorbital notch, and impingement of the nerve by vascular engorgement must therefore be taken into account. An abnormally narrowed bony canal may also facilitate compression between the (swollen or not) artery and the nerve. Further research should also explore this possible vascular mechanism.
In conclusion, supraorbital neuralgia is a relatively infrequent unilateral painful syndrome with usual onset in the middle or late stages of life, and prevailing in the female. Its main characteristics are:
Moderate to severe, strictly unilateral forehead pain;
Recurrent or chronic temporal pattern. The continuous pattern may eventually seem to dominate;
Lack, or paucity, of accompaniments and precipitating mechanisms;
Absolute alleviation of the symptoms upon anaesthetic blocking of the supraorbital nerve;
Tenderness over the emergence or course of the supraorbital nerve on the symptomatic side.