
Abstract
The timing and clinical relevance of diffuse pachymeningeal enhancement (DPE) in the magnetic resonance imaging (MRI) examination of patients with spontaneous intracranial hypotension (SIH) remain undetermined. We reviewed 53 consecutive SIH patients (30 F/23 M, mean age of onset 41.7 ± 11.3 years) in a tertiary hospital. Thirteen (24.5%) patients did not have DPE on their initial cranial MRIs. They had significantly shorter latency between the time of MRI examinations and the time of headache onset compared with those with DPE (6.5 ± 4.4 vs. 20.4 ± 16.3 days, t-test, P < 0.001). Eight of these 13 patients received a follow-up MRI (mean duration 30.3 ± 16.6 days, range 6-59 days) and six of them revealed DPE. Among patients with DPE, the enhancement disappeared as early as 25 days after headache onset. The outcome did not differ between patients with and without DPE. The presence of DPE was associated with the timing of the MRI examination.
Introduction
Spontaneous intracranial hypotension (SIH) is a syndrome characterized by postural headache. However, its manifestations are protean and sometimes characterized by atypical presentations, such as postural dizziness, exertional headache or mental decline (1), which may result in underdiagnosing this headache disorder (2) and highlights the importance of diagnostic imaging, especially cranial magnetic resonance imaging (MRI). The characteristic cranial MRI findings of SIH include diffuse pachymeningeal enhancement (DPE), brain descent and pituitary gland enlargement (1, 3). DPE is the most characteristic finding of SIH. Nevertheless, 7–29% of patients with SIH do not show DPE on their MRIs (4–6).
The determining factors related to DPE on brain MRIs in patients with SIH are not yet clear. One study failed to find any differences between SIH patients with and without DPE (7). One study has reported that a normal initial MRI might be related to a poor outcome (8). It has been our experience that patients without DPE on their initial MRIs usually show DPE at later evaluation. We therefore retrospectively investigated a large group of patients with SIH to determine whether the timing of MRI performance is related to DPE.
Methods
We retrospectively reviewed consecutive patients with SIH at Taipei-Veterans General Hospital (Taipei-VGH), a tertiary medical centre in Taiwan, between January 1998 and February 2007. Because there is no effective ‘gatekeeper’ for the healthcare delivery system in Taiwan (9), most of our SIH patients were self-referred or via our emergency department. Each patient completed a structured headache intake form during their first visit to our headache clinic or when admitted to our ward.
For study inclusion, the patients had to meet all the criteria for ‘headache attributed to spontaneous low CSF pressure’ proposed by the International Classification of Headache Disorders, 2nd edition (code 7.2.3) (ICHD-2) (10), except for criterion (D): headache resolves within 72 h after epidural blood patching (EBP) because not all patients received EBP. We excluded patients who had prior dural punctures, epi- or peridural anaesthesia, ventriculoperitoneal shunt or other causes of CSF fistula.
MRI examination
The MRI examination, both with and without administering intravenous contrast medium [gadopentetate dimeglumine (Gd) 0.1 mmol/kg b.w.], was performed on a 1.5-T system to all patients with the same methods. Brain images were obtained in the transverse plane with T1- and T2-weighted spin-echo sequences. The section thickness was 8 mm, with an acquisition matrix of 256 × 256. In order to evaluate DPE, post-Gd-enhanced T1-weighted images in the transverse plane were also obtained. We defined positive DPE as bilateral, diffuse, smooth and continuous pachymeningeal enhancement. The iter, i.e. the opening of the cerebral aqueduct, and cerebellar tonsil displacements were measured on the sagittal T1-weighted MRI scan to determine the degree of brain descent (11). The prepontine cistern space was defined by measuring the distance from clivus to mid-pons. The timing of the performance of the MRI studies was documented in relation to the onset of SIH symptoms, i.e. the appearance of postural headache. Some patients received heavily T2-weighted MR images to detect CSF leakage (12).
Treatment
Patients with SIH were given conservative treatments, such as hydration, and medications, including caffeine, theophylline, fludrocortisone and/or analgesics. If conservative treatments failed, EBP were performed. None of the patients received surgical repair for CSF leakage.
Follow-ups
We evaluated the recovery time based on reviewing patients' charts. We also conducted the Migraine Disability Assessment Score (MIDAS) questionnaire (13) either in person or by telephone interview to evaluate their current headache disability.
Statistics
SPSS Version 11.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Means were compared using unpaired t-test, and proportions were compared using χ2 or Fisher's exact tests when appropriate. All P-values were two-tailed, and statistical significance was defined as a P-value of <0.05.
Results
Patients
During the study period, 53 consecutive patients (23
Demographic, clinical and imaging findings of study patients with spontaneous intracranial hypotension
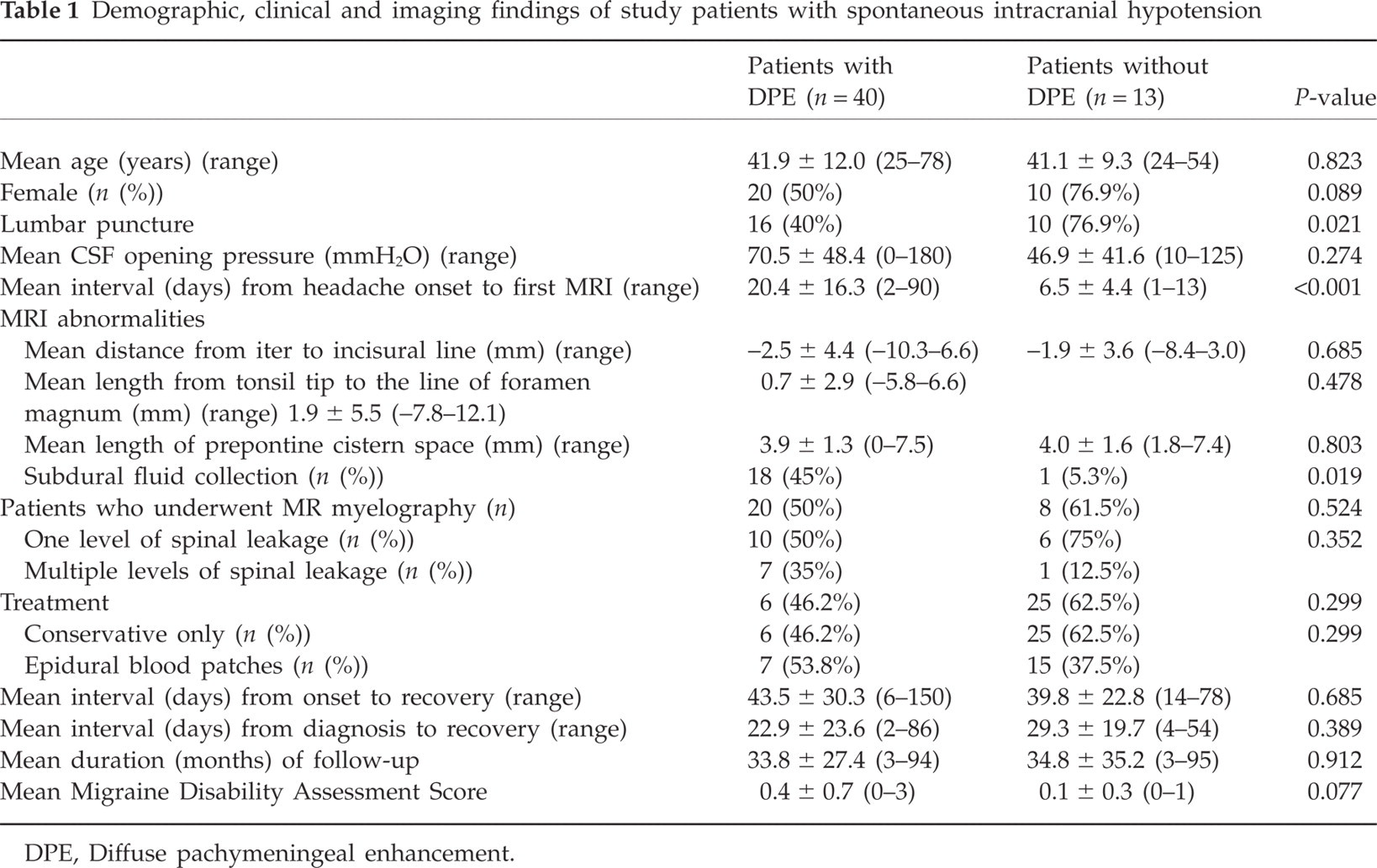
DPE, Diffuse pachymeningeal enhancement.

Gadolinium-enhanced coronal magnetic resonance imaging in a 52-year-old woman with spontaneous intracranial hypotension. (a) Day 11 after headache onset, no abnormal pachymeningeal enhancement. (b) Day 28, prominent bilateral pachymeningeal enhancement. (c) Day 58, pachymeningeal enhancement is regressed. (d) Day 267, pachymeningeal enhancement disappears.
The degree of brain descent and prepontine cistern space did not differ between patients with and without DPE in their initial MRIs. Patients with DPE in their initial MRIs had a significantly higher proportion of subdural fluid collections (including subdural haematoma and non-haemorrhagic subdural collections) compared with those without enhancement (45.0% vs. 5.3%, Fisher's exact test, P = 0.019). Twenty-eight patients underwent MR myelography examination (12), 24 of whom showed at least one leakage site. The proportion of negative findings, single leakage site and multiple leakage sites did not differ between patients with and without DPE.
The mean duration of follow-up was 34.1 ± 29.2 months (range 3–96 months). Overall, 50 patients (94.3%) had a good outcome after hydration and/or EBP within 3 months. Only three patients did not have satisfactory outcomes, and one of them did not have a DPE in the initial MRI. The MIDAS questionnaire was completed in 48 patients (90.6%); only 10 still had some infrequent, non-orthostatic headaches, and all MIDAS scores were between 0 and 5, i.e. ‘minimal disability’ (13).
Discussion
To our knowledge, this is the largest study to evaluate the timing of appearance of DPE in patients with SIH. Consistent with a previous study (18), we found that absence of DPE could not exclude the diagnosis of SIH. In contrast with two previous studies (7, 8), we found patients without DPE in their initial MRIs usually had both a shorter latency between MRI examination and their headache onset and a lower proportion of subdural fluid collections.
Our previous study found that the latency between the MRI examinations and headache onset was longer for patients with subdural fluid collections compared with those without (16). The lower frequency of subdural fluid collections in patients without DPE in their initial MRIs suggested that they might either be in the early stage of SIH or have a less severe disease.
It is thought that the development of DPE is due to a compensatory pachymeningeal venous engorgement and therefore results in a greater concentration of gadolinium in the dural vasculature and interstitial fluid (3). The finding that some patients did not show DPE initially but developed them at a later time suggests that development of DPE may take a certain amount of time in some patients. These patients might not have quantitatively sufficient compensatory venous engorgement to result in DPE at the beginning. In two patients, we also found that the DPE disappeared even though CSF leakage persisted. Therefore, a new balance might be achieved between whole intracranial CSF and blood volume, and accordingly the compensatory venous engorgement disappears.
Our findings showed that the timing of DPE varied widely, which demonstrates the high degree of variability in the disease course. This explains why previous studies (7, 8) have failed to find an association between the timing of MRIs and meningeal abnormalities. Two previous studies have also shown that patients with DPE had a longer time interval from headache onset to MRI examination compared with patients without (Chung et al.: 18.9 ± 19.7 days vs. 10.7 ± 9.2 days; Schievink et al.: 4 weeks vs. 3 weeks) (7, 8). The small case number and wide range in duration of MRI examinations may have also caused the results to be statistically insignificant.
For the four patients who had a DPE in their second MRI and had a lumbar puncture before their second MRI, we can not exclude the possibility that the lumbar puncture might have contributed in part to the appearance of the DPE. However, two patients who did not receive lumbar punctures still showed DPEs later.
Our data have shown that SIH patients with a normal initial cranial MRI had at least a similarly good outcome to those with abnormal MRIs. This finding is different from the study results of Schievink et al., who have reported a better outcome (97%) in patients with an abnormal MRI than in those (14%) with a normal MRI (9). They also found that all patients with a normal initial MRI had multiple spinal CSF leaks, which explained their poor prognosis (8). Two points might explain the discrepancy between their study and our study. One point of discrepancy is the selection bias; the patients presented by Schievink et al. were seen in a neurosurgical centre with a focus on the surgical repair of CSF leaks. Therefore, their findings may not generalize. Second, the number of patients with a normal cranial MRI is only a small part of the total SIH patients. Larger numbers of patients are needed before any conclusions can be drawn.
In conclusion, the appearance of DPE was related to the timing of MRI examination and was possibly due to disease severity. Some patients took a longer time to develop DPE. Whether the appearance of DPE in the initial brain MRIs is related to the outcome needs to be examined with further prospective controlled studies.
Footnotes
Acknowledgements
This study was supported in part by a grant from Taipei Veterans General Hospital (V96C1-013).