
Abstract
Associations between headache, including migraine, and gastrointestinal (GI) symptoms were studied in a large questionnaire-based cross-sectional study (the Head-HUNT Study). The headache questionnaire was completed by 43 782 individuals, who answered all the questions concerning nausea, reflux symptoms, diarrhoea and constipation. In the multivariate analyses, adjusting for age, sex, educational level, medication use, depression and anxiety, a higher prevalence of headache was found in individuals with much reflux [odds ratio (OR) 2.4, 95% confidence interval (CI) 2.2, 2.6], diarrhoea (OR 2.4, 95% CI 2.1, 2.8), constipation (OR 2.1, 95% CI 1.9, 2.4) and nausea (OR 3.2, 95% CI 2.6, 3.8) compared with those without such complaints. All the GI symptoms investigated seemed to be approximately as common among persons with non-migrainous headache as among migraine sufferers, but the association between headache and GI complaints increased markedly with increasing headache frequency. This may suggest that headache sufferers generally are predisposed to GI complaints.
Introduction
Both headaches and gastrointestinal (GI) symptoms such as nausea, acid regurgitation, diarrhoea and constipation are common in the general population and account for substantial healthcare utilization. However, the scientific literature about the comorbidity of headache and GI complaints is scant (1).
Population-based studies have shown positive associations between migraine and irritable bowel syndrome (IBS) (2), colitis and peptic ulcer (3). However, in one study migraine has been associated with peptic ulcer only among smokers (4). Although a pathogenic role for Helicobacter pylori (Hp) infection in migraine has been suggested (5), most studies have not demonstrated any association between Hp infection and migraine (6, 7). Coeliac disease has also been linked with migraine (8), but it remains to be confirmed by larger epidemiological studies.
Clinic-based studies have demonstrated a higher prevalence of gastro-oesophageal reflux (9) and idiopathic dyspepsia (10) among migraineurs. However, in a recent clinic-based study on patients with dyspepsia referred for upper GI endoscopy, migraine prevalence was lower among patients with reflux-like/ulcer-like dyspepsia and higher only among those with dysmotility-like dyspepsia or nausea/vomiting (11). Furthermore, upper endoscopy and oesophageal pH monitoring in migraineurs have shown a low prevalence of abnormal findings (11, 12).
As regards a possible association between non-migrainous headache and GI symptoms, hardly any reports are available. Further knowledge about associations between headaches and GI complaints is important, as comorbidity may alter the clinical course of the disorder and the chance of correct diagnosis by affecting the time of detection, prognosis and choice of therapy (3).
The aim of the present study was to investigate possible associations between GI complaints and headache in a large-scale, population-based, cross-sectional health study.
Methods
Study population
All inhabitants aged ≥20 years in Nord-Tr⊘ndelag County in Norway were invited to participate in the Nord-Tr⊘ndelag Health Study between 1995 and 1997 (‘Helseunders⊘kelsen i Nord-Tr⊘ndelag’ = HUNT). The target population, including participants and non-participants, has been described in detail previously (13). Briefly, of the 92 566 eligible individuals, 64 560 (70%) participated. Two questionnaires, including >200 health-related questions, were administered to the participants. The first questionnaire (Q1) was enclosed with the invitation letter, and the second (Q2) was filled in after a medical examination. The Q1 included questions about GI complaints and the Q2 included 13 questions about headache (13). These questions were mainly designed to determine whether the person suffered from headache or not, to determine frequency of headache and to diagnose migraine according to a modified version of the migraine criteria of the Headache Classification Committee of the International Headache Society (1988) (14).
A total of 51 383 subjects completed the headache questionnaire Q2 and constituted the ‘head-HUNT’ study. Of these 51 383 individuals, 45 453 (88.5%) completed at least one question about GI complaints and 43 782 (85.2%) completed all the questions about GI complaints.
The HUNT study was approved by the Regional Committee for Medical Research Ethics and by the Norwegian Data Inspectorate.
Headache diagnoses
Subjects who answered ‘yes’ to the question ‘Have you suffered from headache during the last 12 months? ‘were classified as headache sufferers (13). Based on data from the subsequent 12 headache questions, they were classified into two groups of either migraine or non-migrainous headache. The diagnoses were mutually exclusive. Persons were classified as migraineurs if they reported having migraine or fulfilled the following three criteria: (i) headache attacks lasting 4–72 h (<4 h was accepted for those who reported visual disturbances often before headache); (ii) headache with at least one of the following three characteristics: (a) pulsating quality; (b) unilateral location; or (c) aggravation by physical activity; (iii) during headache, at least one of the following symptoms: (a) nausea; or (b) photophobia and/or phonophobia. Headaches that did not fulfil the criteria for migraine were classified as non-migrainous headache.
Based on a question about headache frequency during the last year, headache frequency was divided in three categories: <7 days/month, 7–14 days/month and >14 days/month. The classification of the subjects has been described in detail previously and has been validated by interview diagnoses (15).
Gastrointestinal complaints
Q1 included questions about different GI symptoms such as: ‘have you suffered from nausea during the last 12 months?’. The same kind of question was also asked about heartburn/acid regurgitation (reflux symptoms), diarrhoea and constipation, and the subjects were asked to rate the intensity of these symptoms as ‘no’, ‘some’ or ‘much’. Heartburn and acid regurgitation are the cardinal symptoms of gastro-oesophageal reflux disease (16).
Statistical analysis
The association between headache and GI complaints was estimated using multiple logistic regression with odds ratio (OR) and 95% confidence intervals (CI). The interaction coefficients were tested using Wald test statistics. Potential confounders such as gender, age (10-year categories), duration of education (≤9 years, 10–12 years and ≥12 years), depression, anxiety, and medication use were adjusted for. Medication use was based on questions in Q2: ‘Have you taken any medication daily or almost daily during the last 12 months?’ Those who answered ‘yes’ were asked about type of medication (analgesics, sleep medications, tranquillizer, antidepressants, antasthmatics, cardiovascular medication, iron supplement, vitamins, fish oil or other medicines) and how many months they had used it. Anxiety and depression were assessed by The Hospital Anxiety and Depression Scale (HADS) (17–19). Other variables such as alcohol consumption, smoking and body mass index (BMI) were also evaluated as potential confounders.
The ORs for the association between levels of headache frequency and different GI symptoms were performed for each headache diagnosis (migraine and non-migrainous headache) separately where headache-free individuals were used as the reference group. When appropriate, the GI complaints were treated as single ordinal variables (categories 1, ‘no’; 2, ‘some’; and 3, ‘much’) and were incorporated in a test for trend (approximately a χ2 statistic with one degree of freedom) in the logistic analyses to evaluate the probability of a linear relationship between degree of GI complaints and headache (‘dose–response relation’). Likewise, headache frequency categories were incorporated in a test for trend, evaluating the probability of a linear relationship between headache frequency and reflux symptoms, diarrhoea, constipation and nausea, respectively. The trend test was considered statistically significant at P < 0.05. Differences between means were tested with one-way
Results
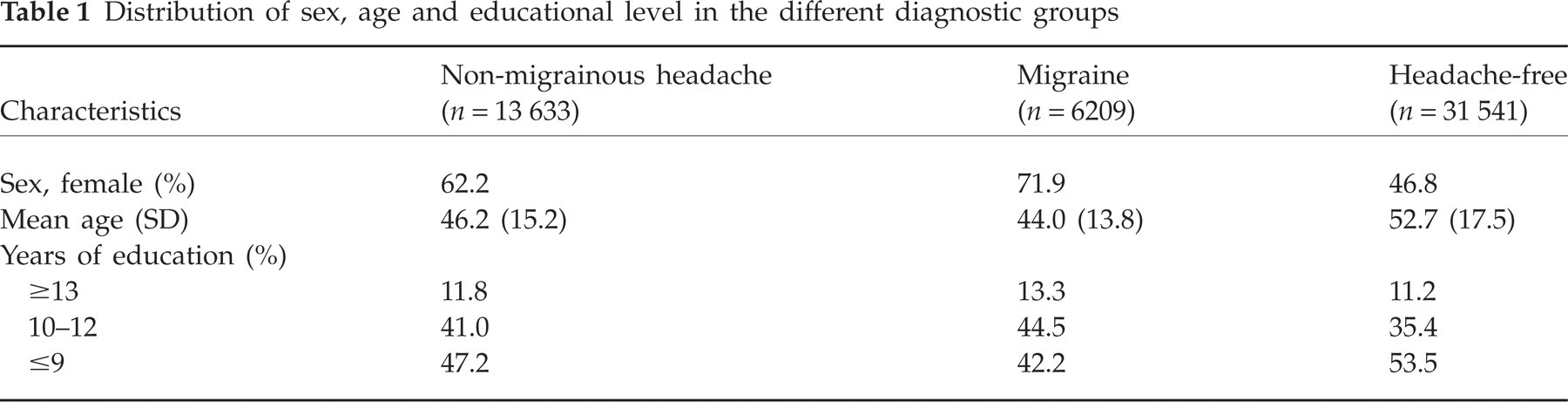
Table 1 presents the demographic data for the different headache groups. There were more women than men in the headache groups compared with headache-free individuals, and this was most pronounced for those with migraine. The mean age was higher in the group of headache-free individuals compared with the groups with migraine or non-migrainous headache. There were also slight differences in the educational level between the groups.
Distribution of sex, age and educational level in the different diagnostic groups
Among the GI symptoms, reflux was the most common in both genders. Constipation and nausea were more prevalent in women (respectively, 30.7% and 18.0%) than in men (respectively, 13.9% and 8.6%), whereas reflux and diarrhoea were more equally distributed among men and women (reflux, respectively, 33.3% and 29.6%, and diarrhoea 16.9% and 17.2%).
As shown in Fig. 1, higher headache prevalence was found in all age groups among those with much reflux symptoms compared with those with some or no such complaints (unadjusted analyses). There was significant interaction by gender regarding non-migrainous headache for all GI complaints, with higher ORs for non-migrainous headache in men than women, e.g. OR for non-migrainous headache among men with some reflux 1.7 (95% CI 1.6, 1.8), much reflux 2.0 (1.8, 2.3). The corresponding ORs for women were 1.5 (1.4, 1.6) and 1.7 (1.5, 1.9). However, the results in the multivariate analyses are shown for men and women together as there were no major gender differences. After adjusting for gender, age, educational level, medication use, anxiety and depression, there were linear trends (P < 0.0001) of increasing prevalence of headache (both migraine and non-migrainous headache) with increasing intensity of GI symptoms. This was most clearly demonstrated for nausea, headache being more than three times more likely (OR 3.2, 95% CI 2.6, 3.8) among individuals with ‘much’ nausea compared with those without nausea (Table 2). The associations between headache and GI symptoms were reduced after adjustment for potential confounding by medication use, anxiety or depression. For example, the OR for all headache types in much diarrhoea was 3.0 (95% CI 2.6, 3.4) after adjustment for only sex, age and education. The corresponding OR was 2.7 (95% CI 2.3, 3.1) after adjustment for medication use in addition and 2.5 (95% CI 2.1, 2.8) after adjusting for all the covariates.
Prevalence odds ratio (OR) of headache (dependent variable) among different groups with gastrointestinal complaints. Not all individuals answered all questions

Odds ratio adjusted for sex, age, education, depression, anxiety and use of medication calculated in multiple logistic regression. P-trend value <0.0001 for all the variables.

One-year prevalence of headache (%) related to age in those with no, some, and much reflux symptoms.
In addition, there were strong linear trends (P < 0.0001) of higher prevalence ORs for all the GI complaints with increasing headache frequency (Table 3). The OR for each of the symptoms reflux, diarrhoea and constipation was increased more than two times for those with headache >14 days/month compared with those without headache. For nausea the corresponding OR values were 6.7 (95% CI 5.2, 8.5) for migraine and 4.8 (95% CI 4.0, 5.7) for non-migrainous headache compared with those without headache.
Prevalence odds ratio (OR) of different gastrointestinal complaints (dependent variables) related to headache frequency and compared with headache-free subjects

Odds ratio adjusted for sex, age, education, depression, anxiety and use of medication calculated in multiple logistic regression. P-trend value <0.0001 for all the variables. The gastrointestinal symptoms were considered to be present if there were some or many of the symptoms.
Discussion
In this large-scale, population-based, cross-sectional study we found higher prevalence of headache in individuals with much reflux symptoms, diarrhoea, constipation or nausea than in those without such complaints. There were no major differences between migraine and non-migrainous headache regarding the association with GI complaints. The association between headache and GI complaints increased markedly with increasing headache frequency.
The strengths of the study were the large and unselected population and the use of validated headache diagnoses. The question on acid regurgitation/heartburn (reflux) has also been validated (20) and the use of questionnaires to assess these symptoms is well validated as a reliable measurement of the true occurrence of reflux (21, 22). However, there are several limitations to the study. First, other GI symptoms have not been validated and no further GI investigations were performed, so the reported complaints may have represented different disorders. However, one would expect that functional GI disorders, being very prevalent in the general population, are responsible for the described GI symptoms among the majority.
Furthermore, the questionnaire-based headache diagnoses were not optimal compared with the interview diagnoses (15). The bias caused by misclassification can either exaggerate or underestimate the true differences between headache groups. Most likely, due to diagnostic inaccuracy, there were migraine patients in the group of non-migraineurs and vice versa, making the two groups more similar than they really were. The impact of non-participants has been discussed in more detail previously (13). The fact that headache and GI complaints were among many other objectives of HUNT makes selective participation due to headache or GI complaints unlikely. In addition, the prevalence of migraine in the current population is consistent with data from other population-based studies in Western countries (23). Furthermore, the prevalence of GI symptoms in the current population is comparable to that found in other studies (24–28).
Our results seem to be in accordance with previous population-based and clinic-based studies concerning comorbidity of migraine and GI conditions (2, 3, 9–11). Furthermore, headache has been reported as a significantly more frequent symptom in various unexplained clinical conditions such as IBS, fibromyalgia and chronic fatigue syndrome (29–32).
In the present study, headache frequency seems to have had a greater impact on the association with GI complaints than the headache diagnoses. The GI symptoms investigated in this study seem to be approximately as common among persons with non-migrainous headache as among migraine sufferers, which may suggest that headache sufferers generally are predisposed to other pain syndromes and somatic complaints (33). An exception was nausea, which was more prevalent among migraineurs (Table 3). This is not surprising, as nausea is among the diagnostic criteria for migraine.
Information bias should be considered as an explanation for the findings in the present study. In studies on self-reported complaints the results may be influenced by a tendency to report different symptoms in some individuals (34, 35). Those who report their headache complaints might be more likely to report other complaints such as GI symptoms. This may create strong associations that are explained by personality traits rather than by biological mechanisms (34, 36). However, the findings in the present study were in line with other studies using different methods (2, 3, 9, 11).
Since the study is cross-sectional it cannot be determined whether frequent headache causes GI complaints or whether other risk factors or a shared susceptibility causes this association. Autonomic nervous system (ANS) dysfunction, which has previously been linked to both headache and GI complaints, might be a common mechanism (37–43). The association between headache and GI symptoms may also be related to interactions between the nociceptive system and the ANS. There is anatomical and functional evidence of convergence between nociceptive and viscerosensory systems involved in reflexes and homeostatic and behavioural control of autonomic outflow (44). Several studies, mostly clinic based, have demonstrated autonomic dysfunction in migraineurs during headache-free intervals, as well as during migraine attacks (42). In disorders such as IBS and functional dyspepsia psycho-social factors, dysregulation of the ANS, altered intestinal motility and increased visceral sensitivity have been demonstrated. The latter is thought to result from dysregulation of the bidirectional communication between the gut with its enteric nervous system and the central nervous system—the brain–gut axis (37–40, 45–49).
Other possible explanations might be that GI complaints lead to headache, or, vice versa, that the GI complaints represent manifestations of the GI component of migraine. In the study of Meucci et al. there were completely normal endoscopic findings in 90% of migraineurs with nausea/vomiting or other dysmotility-like symptoms, and their symptoms were considered related to their migraine attacks and not to any GI disorder (11). The GI symptoms may also represent side-effects caused by medicines against headache. It is well known that opioid analgesics may cause constipation and nausea, and various GI symptoms are common side-effects of NSAIDs. Furthermore, psychological factors may also be a common denominator for headache and GI symptoms, as both are strongly associated with anxiety and depression (50–53). The strength of the associations between headache and GI complaints was gently reduced after adjusting for medication use (54, 55), anxiety, and depression (assessed by HADS) in the multivariate analyses. However, one cannot exclude the possibility that if more extensive data about medication use and psychological factors had been available, the strength of association would have been even more attenuated after adjustment.
In conclusion, the observed association between GI complaints and chronic headache may have clinical implications. It is important to consider the total burden of discomfort in these patients in order to provide for the best treatment, and the prognosis as to overall function may be determined not only by headache, but also by the comorbid conditions. Further research about the aetiology of association of headache and GI complaints is needed.
Footnotes
Acknowledgements
The Nord-Tr⊘ndelag Health Study (The HUNT Study) is a collaboration between HUNT Research Centre, Faculty of Medicine, Norwegian University of Science and Technology (NTNU), Verdal, Norwegian Institute of Public Health, and Nord-Tr⊘ndelag County Council.