
Abstract
The aim was to evaluate the test-retest reliability of the French translation of the Migraine Disability Assessment (MIDAS) and Headache Impact Test (HIT)-6 questionnaires as applied to episodic and chronic headaches and to assess the correlation between these two questionnaires. The MIDAS and HIT-6 questionnaires, which assess the degree of migraine-related functional disability, are widely used in headache treatment clinics. The French translation has not been checked for test-retest reliability. MIDAS involves recall, over the previous 3 months, of the number of days with functional disability with regard to work and to home and social life. HIT-6 involves a more subjective and general assessment of headache-related disability over the previous 4 weeks. We expect that there may be greater impact recall bias for chronic headaches than for episodic headaches and considered it important to be able to determine if the reliability of these questionnaires is equally good for these two patient populations. Given that both questionnaires have the same objective, that of assessing headache impact, it was thought useful to determine if their results might show a correlation and if they could thus be used interchangeably. The study was approved by an external ethics committee. The subjects were patients who regularly visit the Clinique de la Migraine de Montréal, which specializes in the treatment of headaches. The MIDAS and HIT-6 questionnaires were completed by the patients during their regular visit. Twelve days later, the same questionnaires were mailed with a prepaid return envelope. Sixty-five patients were required in both the episodic and chronic headache groups, assuming an 80± questionnaire return rate. One hundred and eighty-five patients were enrolled, and 143 completed the study, 75 with episodic headaches and 68 with chronic headaches. The questionnaire return rate was 78.9±. On average, questionnaires were completed a second time 21 days after the first, with a median of 19 days. The Shrout-Fleiss intraclass correlation coefficients for MIDAS and HIT-6 were, respectively, 0.76 and 0.77 for episodic headaches and 0.83 and 0.80 for chronic headaches. The Pearson correlation coefficient between the MIDAS and HIT-6 questionnaires was 0.48 for episodic headaches and 0.58 for chronic headaches at the first compilation and 0.42 and 0.59 at the second compilation. The test-retest intraclass correlation of the French versions for both MIDAS and HIT-6 questionnaires indicates moderate reliability for episodic headache and substantial reliability for chronic headache. The correlation between the MIDAS and HIT-6 questionnaires is weak for episodic headaches, but approaches a level of ‘good’ for chronic headaches.
Introduction
Only recently has attention been paid to the functional impact of migraine and headache, and it has been slow to be applied in clinical settings. The first questionnaire developed to document this impact was the HimQ (1). Its validity (comparison with a migraine diary) and reliability (test–retest) were documented in 1998. Migraine Disability Assessment (MIDAS) was derived from HimQ, which was not very user friendly for routine application (2). MIDAS targets headache days only and involves headache recall over the previous 3 months. It differs from quality-of-life evaluation questionnaires that examine overall quality of life without differentiating between headache and non-headache days. The objectives of the authors of the MIDAS questionnaire were to stratify patients in order to identify those requiring special attention in terms of treatment and to develop a reliable tool to monitor the course of patients in clinical and epidemiological research.
Headache Impact Test (HIT)-6 was developed after MIDAS. The main objective is to identify and stratify patients requiring special attention in terms of treatment. The headache recall period is 4 weeks vs. 3 months in the case of MIDAS and does not include days of absence or disability, but rather a semiquantitative assessment of disability. HIT-6 is routinely used on websites.
The validity of the English (3), Japanese (4) and Turkish (5) versions of MIDAS has been compared with that of a headache diary. The questionnaire's test–retest reliability has been checked in these three languages and in Italian (6), but not in French. The authors' headache treatment clinic is looking for a rapid and convenient tool for documenting the clinical outcome, whether favourable or unfavourable. MIDAS and HIT-6 might enable this objective to be met.
Since the reliability of the French versions of these questionnaires had not been checked, the objective of this study was to do so before using the questionnaire systematically to evaluate and follow patients who suffer from headaches. In addition, the reliability of these questionnaires had been checked only for episodic headaches. We question the accuracy of recalling the functional impact associated with a large number of headaches, i.e. > 45 per 3 months. The second objective was therefore to check the test–retest reliability for chronic headaches. The last objective was to determine if there is a correlation between the MIDAS and HIT-6 questionnaires. Since HIT-6 is easier for patients to complete, we wanted to determine if these two questionnaires could be used interchangeably.
We did not consider it essential to check the reliability of the questionnaires compared with that of a headache diary, as it was felt that the previous studies that had demonstrated this correlation did not need to be repeated.
Methods
The study was approved by an external ethics committee (Institutional Review Board Services, 21 July 2004). All subjects were regular patients at the Clinique de la Migraine de Montréal and were selected during their usual follow-up interviews. Their condition was stable and did not require any significant adjustment to their treatment.
Questionnaires
The MIDAS questionnaire used is a French translation, from Innovative Medical Research©, of the original English questionnaire. It has not been back-translated and was chosen because it had been widely distributed in Quebec for > 5 years. However, a minor change was requested by the ethics committee. It consisted of changing the order of two parts of the first sentence of each question, namely, ‘Au cours des trois derniers mois, pendant combien de jours …’ (In the last 3 months, on how many days …) instead of ‘Pendant combien de jours au cours des trois derniers mois …’ (On how many days in the last 3 months …). The HIT-6 questionnaire used is the one distributed by 2001 QualityMetric, Inc.© and the GlaxoSmithKline group of companies and has been translated from English to French and to several other languages using a rigorous comparison and back-translation process (7).
Inclusion criteria
The diagnosis of migraine and/or tension-type headache (TTH) was based on 2004 International Headache Society (HIS) criteria. Episodic headaches were defined as a frequency of < 15 days per month, chronic headaches as a frequency of ≥ 15 days per month. The patient's condition had to be stable enough for there to be no significant change in treatment when completing the first questionnaire.
Exclusion criteria
Exclusion criteria were an inability to understand the questionnaire, not being gainfully employed or not being a full-time student, and a significant change in treatment when completing the first questionnaire. A change was considered significant if preventive or abortive medication was introduced. Adjustment to the dose of preventive medication was not considered a significant change.
Conduct of the study
During the patient's regular appointment, the consent form was read and, if applicable, signed. The completed questionnaires were checked by the attending physician. The same questionnaires were mailed 12 days later, together with a prepaid return envelope. There was no financial incentive.
Statistical analysis
At least 54 patients were needed in order to demonstrate good reliability with a 95% confidence interval, i.e. a reliability coefficient > 0.6. The Shrout–Fleiss coefficient (8) was used for the intraclass correlation for the MIDAS and HIT-6, and the Pearson coefficient for correlation between the two questionnaires.
Results
Population
A total of 185 patients were enrolled, 143 (77%) of whom were retained in the study. The questionnaire return rate was 78.9%. Forty-two patients (23%) were excluded because they did not return their questionnaires (39) or because their questionnaires, although returned, were not filled out completely (3).
The second questionnaire was returned a mean of 21.1 days after the first one, with a median of 19 days. Of the patients who were retained, 75 had episodic headaches (< 15 headache days per month), and 68 had chronic headaches (≥ 15 days per month). Of the unreturned questionnaires, 12 (31%) belonged to patients with episodic headaches and 27 (69%) to patients with chronic headaches.
One hundred and five patients (73%) were female and 38 (27%) male. The episodic headache group consisted of 62 (83%) women and 13 (17%) men. The chronic headache group consisted of 41 (60%) women and 27 (40%) men. The mean age of the 143 patients was 43 years (median 45 years). The mean age of the episodic headache patients was 43.7 years (median 46 years) and of the chronic headache patients 42.3 years (median 43 years).
Errors in answering the questionnaires
Patients had no difficulty understanding the questionnaires. For MIDAS, the main answering errors consisted mostly in entering a range instead of a single number. Of the 146 patients who returned their questionnaires, 18 (12%) indicated a range for at least one of the five questions and 38 (26%) indicated a range for question A or B. Some patients hesitated when answering MIDAS question A, not knowing if a headache had to have lasted the entire day or if having a headache part of the day was sufficient to indicate 1 day. Only four patients forgot one box, and two wrote out an answer in words instead of entering a number.
For HIT-6, only one error was found.
Diagnosis
The diagnoses based on IHS criteria (9) were, for episodic headaches, 65 (87%) migraine, and 10 (13%) migraine and TTH. None of the patients presented only with episodic TTH. The diagnoses for chronic headaches were 21 (31%) chronic migraine, eight (12%) migraine and episodic TTH, 31 (45%) migraine and chronic TTH, and eight (12%) chronic TTH.
Scores to questionnaires
See Table 1 for MIDAS and HIT-6-values.
Population

M, Migraine; ETTH, episodic tension-type headache; CM, chronic migraine; CTTH, chronic tension-type headache.
For MIDAS, the scores were similar for both compilations, with a mean of 35.6 and 38.0 for the first and second compilations, respectively. The mean total score on MIDAS for compilation 1 was 23.9 for episodic headaches and 48.6 for chronic headaches. When examining the questions individually, it was noted that the higher score for the chronic headache patients compared with episodic headache patients can be explained by questions 2, 4 and, to a lesser extent, 3 and 5, which concern, respectively, the reduction in productivity at work or school, the reduction in the ability to do household work, days of disability to do household work and the impact on family activities.
For HIT-6, the scores were similar for both compilations, with a mean of 64.0 and 62.7 for the first and second compilations, respectively. The mean total score for compilation 1 was 64.9 for episodic headaches and 63.1 for chronic headaches.
Intraclass reliability by Shrout–Fleiss coefficient for MIDAS and HIT-6
See Table 2 for the values.
Scores to questionnaires
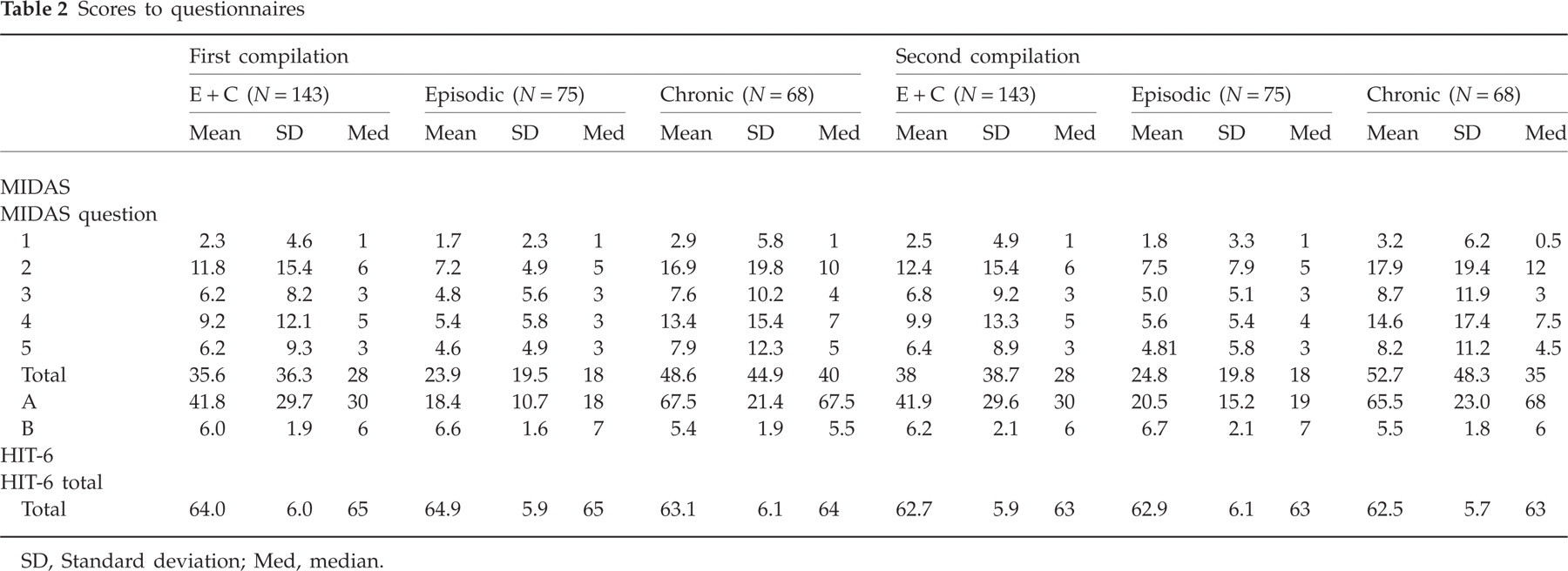
SD, Standard deviation; Med, median.
The intraclass test–retest correlation for the total score on MIDAS indicates substantial reliability for the 143 patients, the coefficient being 0.84, with a slightly higher value for chronic headaches (0.83) compared with episodic headaches (0.76).
For MIDAS question A, which relates to the number of days on which the patient had a headache, the coefficient indicates substantial reliability for the 143 patients (0.84), but fair reliability for chronic headaches (0.52) and moderate reliability for episodic headaches (0.66).
For MIDAS question B, which relates to the severity of headache pain on average, reliability was nearly moderate, with a coefficient of 0.59 for the 143 patients, but slightly correlated for episodic headaches (0.38) and moderately for chronic headaches (0.73).
The intraclass test–retest correlation for the HIT-6 score was nearly substantial for the 143 patients, the coefficient being 0.78, with, once again, a slightly higher value for chronic headaches (0.80) compared with episodic headaches (0.77).
Only a slight intraclass correlation (0.29) was found for the question concerning hospital emergency room visits during the previous year.
Correlation between MIDAS and HIT-6
See Table 3 for the values.
Test–retest reliability for MIDAS, HIT-6 and the question on emergency room visits
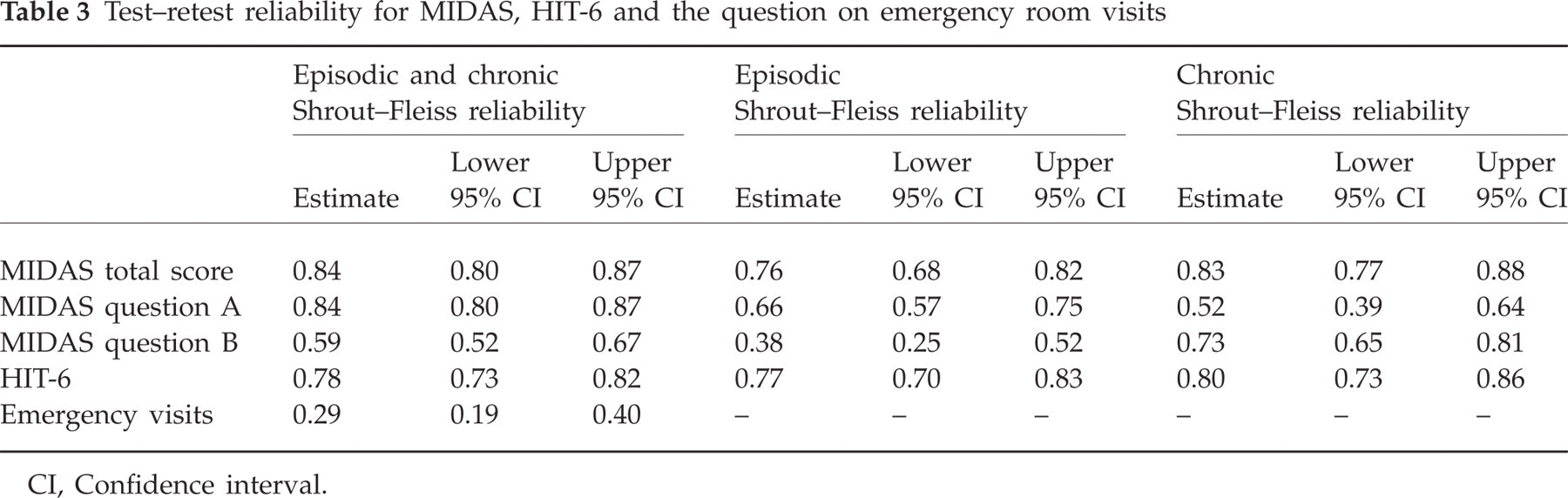
CI, Confidence interval.
Like the Shrout–Fleiss coefficient, the Pearson correlation coefficient was very good for MIDAS (0.84) and HIT-6 (0.80) between the first and second compilations, with a slightly higher value for chronic headaches (0.83) compared with episodic headaches (0.75) in the case of MIDAS. The coefficient was similar for episodic (0.80) and chronic (0.80) headaches in the case of HIT-6.
The correlation between MIDAS and HIT-6 values was low for both the first (0.42) and second compilations (0.44) for all 143 patients. However, once again it was higher for chronic headaches (0.58) compared with episodic headaches (0.48) at the first compilation and was, respectively, 0.59 and 0.42 at the second compilation.
Reliability of the grade-based stratification for the MIDAS questionnaire
See Table 4 for the results.
Correlation between MIDAS and HIT-6

E, Episodic; C, chronic.
The total number of patients in each grade was practically the same at the first and second compilations. Although the number was stable, there was some switching between grades, especially grades II and III. Thus, of the 17 grade II patients at the first compilation, 11 (64%) changed grade at the second compilation, with seven (64%) of them moving to grade III or IV. Of the 25 grade III patients at the first compilation, nine (35%) changed grade at the second compilation, with five of them (56%) moving to grade IV.
Reliability of the score-based stratification for the HIT-6 questionnaire
See Table 5 for the results.
MIDAS grade stratification

The score stratum changes are observed in the lower score ranges. However, because of the number of patients concentrated in the highest range, we do not think that this is interpretable (Table 6).
HIT-6 stratification

Discussion
Questionnaire comprehension and ease of completion
Comprehension of the MIDAS questionnaire was generally good. However, when completing the questionnaire, the patients were frequently reluctant to enter a specific number of days, with the result that there was a tendency to enter a range and sometimes words instead of a number. Clarifications concerning question A were frequently requested to ascertain whether a headache had to have lasted the entire day in order to mark 1 day.
Comprehension of the HIT-6 questionnaire was excellent, as evidenced by the fact that there were no questions or errors.
Population
Both questionnaires were completed within a median of 19 days, which is considered sufficient for preventing recall of the answers on the first questionnaire but insufficient for a change in clinical status. The mean age of the patients was 45 years, which is the age at which the prevalence of migraine is highest, according to a number of epidemiological studies (10, 11). The proportion of approximately three females to one male is consistent with the proportion encountered in epidemiological studies.
Diagnosis
All patients with episodic headaches had a diagnosis of migraine. Ten patients (13%) were also diagnosed with TTH. None of the enrolled patients had a diagnosis of episodic TTH, which is seldom encountered at headache treatment clinics. Accepting the recently proposed criteria of chronic migraine (12), most of our diagnoses of migraine and episodic or chronic TTH could be considered chronic migraine. Thus, nearly 90% of patients with chronic headaches who enrolled in the study fell into this category.
Questionnaire scores
The MIDAS average total score was 35.6 at the first compilation. If episodic headaches are separated from chronic headaches, a mean score of 23.9 and 48.6, respectively, is observed. If the MIDAS five questions are examined, this difference is mainly due to question 2 (mean score of 7.2 in episodic headache patients and 16.9 in chronic headache patients) and question 4 (mean score of 5.4 in episodic headache patients and 13.4 in chronic headache patients), questions in which the patient indicates whether there was a reduction in productivity of ≥ 50%. It is understood that all the patients were, by definition, full-time workers or students, but that they saw their performance diminish in the three functional domains evaluated. Although substantial, the mean number of missed days of work (1.7 days for episodic headache patients and 2.9 for chronic headache patients) was not mainly responsible for the high score and was consistent with keeping one's job.
The grade distribution in the study population at the first compilation was as follows:

This distribution is similar to that reported by Bigal and colleagues (13) in a MIDAS score comparison between chronic and episodic migraines:

The mean score for HIT-6 in our study population was > 60 both for episodic and chronic headaches, which suggests a severe impact in most patients. The distribution was as follows:

Our distribution of HIT-6 scores indicates higher disability than that obtained by Coeytaux and Spierings (14), which shows, as was the case for their population, a severe impact in patients followed at headache treatment clinics:

Intraclass reliability by Shrout–Fleiss coefficient
The test–retest correlation coefficient was excellent for MIDAS and HIT-6 total scores, which means that they have substantial reliability. The correlation coefficient for question A, which concerns the number of headache days during the previous 3 months, was not as good, especially for chronic headaches. Since there were a larger number of headaches, recall was probably more inaccurate and subject to variation. As for question B, which relates to average headache intensity, test–retest correlation was weaker for episodic headaches and good for chronic headaches. We think that patients with chronic headache experience a more stable level of pain than those with episodic headache and variable attacks, with the result that their assessments are more dependent on the experience of more recent headaches.
The test–retest correlation coefficient for emergency room visits was low, but the number of patients who indicated that they had gone to an emergency room in the previous year was also low, i.e. 13/143 (9%). Reports of emergency visits in the migraine population have varied in other studies (15), with frequencies ranging from 14% to 48%. These studies were population based and not regularly followed as was our population.
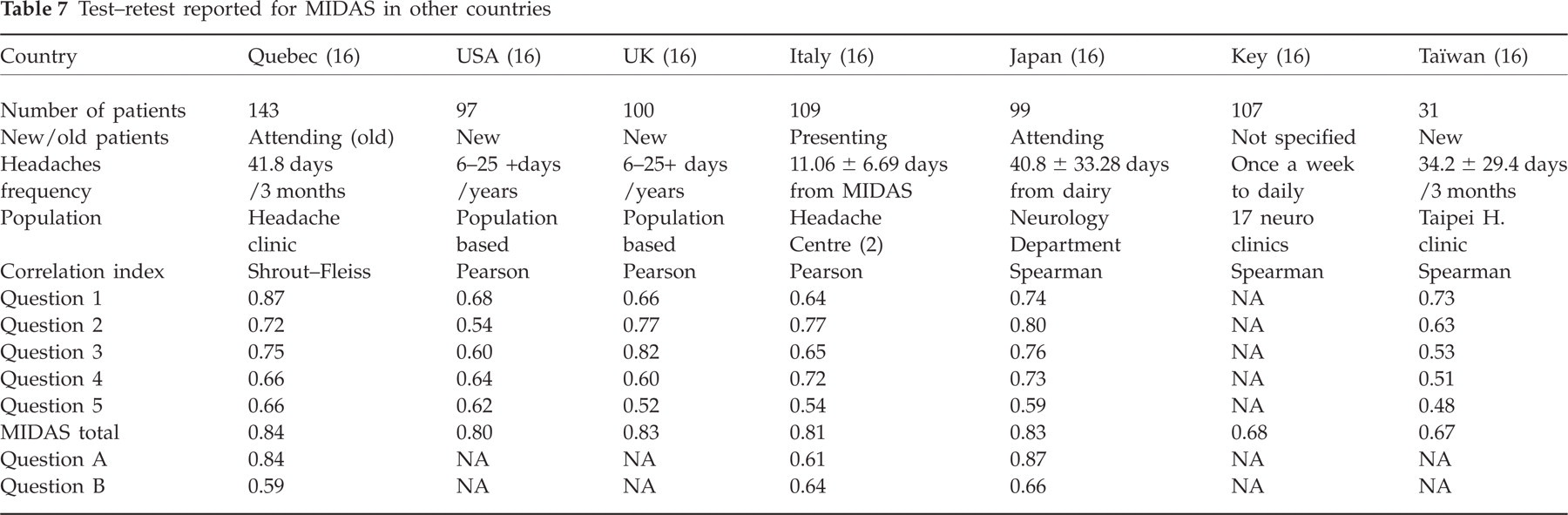
Comparison of coefficient of reliability for MIDAS in other studies (Table 7)
Our coefficients are slightly higher than in other studies, probably because our population of current consulters were more accustomed to following their headaches.
Test–retest reported for MIDAS in other countries
Correlation between MIDAS and HIT-6 by Pearson correlation coefficient
Like the Shrout–Fleiss coefficient, the Pearson coefficient was excellent for MIDAS and HIT-6 test–retest. However, the correlation between these two tests was low, and suggested that they cannot be used interchangeably. We feel that HIT-6 evaluates a more subjective aspect of headache impact, the suffering, whereas MIDAS, since it requires the patient to self-assess the functional impact in terms of days, adds a more quantitative dimension.
Grade stratification reliability of the MIDAS questionnaire
The grade distribution on the MIDAS questionnaire from the first to second compilation was stable, albeit at the expense of changes which, in our opinion, should be taken into account. Thus, 22% of patients changed grade from the first to second compilation, but mainly at the expense of grades II and III, which were the most unstable. For these grades, 60% of the changes were to a higher grade. This change toward a higher grade from the first to second compilation has been observed in the study by D'Amico and collaborators (6), who reported that, from the first to second compilation, seven out of 11 (63%) changes from grade II were to a higher grade.
Six patients changed by two or more MIDAS grades, four to a higher and two to a lower grade. Looking back at their charts, it was seen that the four patients who changed to a higher grade had severe migraine that was not always controlled. One of the two who changed to a lower grade, one had stable chronic TTH and the other had migraine that was not always well controlled. Patients having severe headache after the first MIDAS questionnaire would probably overestimate the previous experience, as stated by Andrasik (16). The reverse was true for lower level pain.
The patients who assessed themselves as grade III or IV were those who should be treated more aggressively. If grade II is unstable, special attention should also be given to these patients.
Conclusion
The French versions of the MIDAS and HIT-6 questionnaires are generally well understood by patients. However, two problems were observed in the case of MIDAS: a tendency to enter a range instead of a discrete number of days and, in subquestion A, reluctance to indicate a day when the headache did not last the entire day. We feel that deleting the word ‘pendant’ (during) would eliminate this problem.
The French versions of MIDAS and HIT-6 have moderate to substantial test–retest reliability and are suitable to be used to monitor the clinical evolution of headache patients. This is true both for episodic and chronic headaches, the correlation coefficient for chronic headaches being higher. With regard to MIDAS question A, the correlation coefficient was slightly higher for the episodic headache group, as the larger number of headaches could cause greater recall inaccuracy. For question B, the correlation coefficient was higher in the chronic headache group. An increase in the number of headaches is usually associated with greater intensity uniformity, which probably results in better recall stability.
MIDAS and HIT-6, both of which assess the functional impact of migraine, are only weakly correlated. We feel that HIT-6 is a more subjective measurement and that it reflects more of the patient's suffering. MIDAS and HIT-6 should not be used interchangeably.
As for the grade-based stratification of MIDAS, we observed, as did D'Amico et al. (6), that grade II patients showed a clear tendency to score themselves as having a more severe grade at the second compilation. Thus, greater attention should be given to this grade than was initially considered.
Given the choice between these two questionnaires for the purpose of following patients in a migraine clinic, MIDAS is more useful than HIT-6. The stratification of patients is more evenly distributed with MIDAS than HIT-6 for those patients who are more severely handicapped by their headache than population-based headache. HIT-6 is more sensitive, but has a ceiling effect.
Acknowledgments
The authors thank GlaxoSmithKline, Janssen-Ortho and Merck, for their unrestrictive support.