
Abstract
There are multiple risk factors for chronic daily headache (CDH), but they are usually assessed in an isolated form without an adequate control for confounders. CDH is considered a variant of episodic headache, but studies have not gathered enough evidence to evaluate simultaneously CDH and episodic in the same population. We set out to establish simultaneously the factors associated with chronic daily or episodic headache in a population setting, using a cross-sectional survey in a random sample of 1505 adult urban inhabitants (Bucaramanga, Colombia). The survey asked questions about headache, family and personal history of disease, and consumption or abuse of caffeine, alcohol, hypnotics and analgesics. The association among independent variables and CDH or episodic headache was made with multinomial logistic regression. Female gender, arterial hypertension or cranial trauma history, and a high score in the depression scale are associated with episodic headache and CDH. Parents with CDH, the complaint of multiple arousals during sleep and use of hypnotics are associated with CDH, but not with episodic headache. Age < 36 years, alcoholism and snoring are factors associated only with episodic headache. Chronic daily headache and episodic headache have several common risk factors, but there are other factors not shared by both conditions.
Introduction
Chronic daily headache (CDH) is a frequent disorder, with a worldwide prevalence of 3.9–4.7% (1–3). It produces severe disability in a quarter of patients suffering from the condition (3), leading to overuse of analgesic medications in 24–34% (1, 3, 4), with only 25–50% seeking medical assistance (2, 3). These four items consolidate CDH as a public health problem, but it is necessary to know its risk factors to clarify the pathophysiology of the disorder and to guide treatment, as well as to facilitate the development of prevention strategies.
Multiple risk factors have been described for CDH in different clinical or population settings (1–29). However, these risk factors have been evaluated in an isolated form or together with a few other risk factors, in such a way that the interaction cannot be determined among the different factors and potential confounding cannot be discarded. On the other hand, it is assumed that chronic migraine and chronic tension-type headache are transformations from their homologous episodic headaches (30, 31) with common pathophysiological pathways in each case; nevertheless, no additional evidence has been gathered through empirical studies where episodic headache and CDH are assessed simultaneously in the same population.
The objective was to show the simultaneous evaluation of associated factors with CDH or episodic headache in the population of Bucaramanga.
Subjects and methods
This was a cross-sectional survey made in the urban area of Bucaramanga, Colombia, which was previously approved by the Review Board of the Universidad Autónoma de Bucaramanga. The sample was selected in two simple random stages. In the first one, 1841 households were selected among the 64 206 registered in the Municipality Territorial Arrangement Plan (32). In a second stage, in each household, all 18–65-year-olds were identified, one of whom was selected by simple randomization. It was hypothesized that CDH had an annual prevalence of 3 ± 1%, for which a sample of 1473 people was required, previewing a 95% confidence and an extra 20% for non-answers. All literate people accepted to participate in the study were included, except those who had some major disability inhibiting their ability to complete the survey (e.g. blindness, mental retardation).
Each individual was personally contacted and asked to complete a self-report survey designed to inquire about headaches and CDH, emphasizing clinical characteristics of primary headache (if applicable), family history of CDH, personal clinical background of arterial hypertension, overuse of analgesics, caffeine consumption, alcoholism, depression, vital stressor events, insomnia symptoms, snoring, and use of hypnotics. To evaluate if primary headache had migraine characteristics, the validated Spanish version of the Diagnostic Questionnaire for Migraine (33) was applied, whereas to test for depression the validated Spanish version for Zung's Self-rating Depression Scale (34) was used. Before beginning the survey we made a facial validation of the entire questionnaire with six experts in neurology or mental health. Later, a pilot study was conducted in order to prove its reliability and some adjustments were made to improve the understanding of the questions.
CDH was considered when the inhabitant reported to have any type of headache for >15 days a month during at least the previous 3 months; episodic headache was considered if the headache was less frequent than 15 days a month or had an evolution <3 months (35). Medication overuse was considered, according to the International Headache Society classification (35), if a patient took simple analgesics >3 days a week, or ergotamine, triptans, or a combination of analgesics >2 days a week during the last 6 months. Alcoholism was defined as the consumption of any alcoholic drink regularly and a history of problems produced by alcohol intake. The vital stressor events considered were to have had a recent loss, difficulties at work, economic difficulties, relationship problems, family difficulties and any other problems that people in the study considered to have affected them in the last 3 months.
The population was described in proportions; a confidence interval of 95% (95% CI), means and SD and interquartile range (IQR) according to the variable type used. These estimates and the statistical tests were adjusted by sampling effect in the ‘Svy’ module of STATA 9.0 (36), and were considered significant when differences showed a type I error <0.05. The association between independent variables and episodic headache or CDH was determined initially by comparing each patient group (without headache, with episodic headache, and with CDH) with the other two; a multinomial logistic regression model was then developed, following Greenland's recommendations (37). Briefly, to develop this model, all variables with any significant association or a P-value <0.2 were included, beginning by gender and the most significant one. If the second variable had significant association or changed the gender odds ratio in >10%, this second variable was accepted into the model, but was otherwise rejected. This process was repeated sequentially until all variables were analysed.
Results
Of 1664 households, 1628 had inhabitants with inclusion criteria, of whom 1505 agreed to participate, giving a participation rate of 92.4% (Fig. 1). Participants' ages varied between 18 and 65 and 1062 were women (70.6%). The median age in men was 34 (IQR 24–45), whereas it was 36 among women (IQR 26–47; P = 0.008). Three hundred and fifty-four (23.5%) had some grade of elementary education, 818 (54.4%) had gone through high school education and 333 (22.1%) had had superior education. There was a higher proportion of women with only primary education (26.6%) than men (16.0%; P < 0.001). A total of 438 persons lived in the low socioeconomic stratum (29.1%), 991 in the medium (65.8%) and 76 in the high stratum (5.5%). The proportion of men interviewed in each stratum was different, accounting for 23.7% in the low stratum, 30.6% in the medium and 47.4% in the high stratum (P < 0.001). This situation showed some grade of selection bias, because the male ratio is different in our sample than in the 2004 local census. To correct this bias, a weighting factor was used to weigh the contribution of each group determined by gender and socioeconomic stratum according to this census (36).
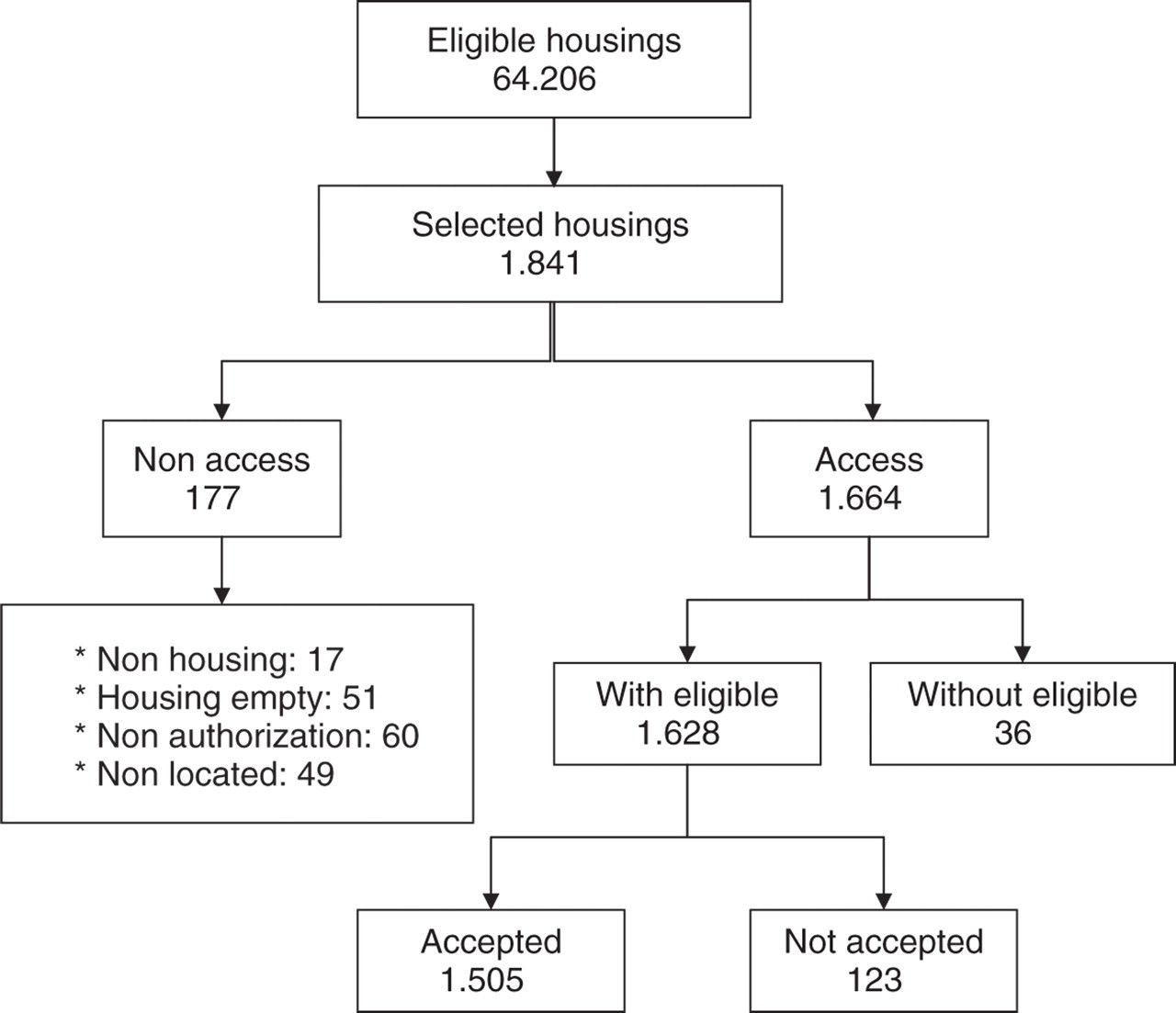
Participant flow chart for the survey.
Fifty-eight percent (95% CI 53.3, 60.7) of participants reported having had a headache episode at least once during their lifetime, being more frequent among females (64.2%, 95% CI 61.1, 67.4) than males (44.0%, 95% CI 39.0, 49.0; P < 0.001). In turn, 13.7% (95% CI 11.8, 15.6) of the participants described clinical characteristics of migraine, also more frequent in women (17.5%, 95% CI 15.0, 20.0) than in men (5.2%, 95% CI 3.0, 7.4; P < 0.001). Finally, 8.4% (95% CI 6.9, 10.0) of the participants reported CDH, but at a higher incidence for women (10.2%, 95% CI 8.2, 12.3) than for men (4.4%, 95% CI 2.3, 6.5; P < 0.001).
The age when headaches had begun was similar among people with CDH (21.2 years, 95% CI 49.5, 23.0) and those that had episodic headache (21.8 years, 95% CI 20.9, 22.6; P = 0.520). However, people with CDH had a longer history of headache (15.8 years, 95% CI 13.4, 18.3) than those with episodic headache (13.1 years, 95% CI 12.2, 14.0; P < 0.001).
Female gender, lower social stratum, family history of alcoholism, CDH, depression, personal history of arterial hypertension, cranial trauma, suicide attempt, vital stressor events, overuse of analgesics, and insomnia complaints were associated with episodic headache when compared with populations without headaches. These same factors and a lower educational level were positively associated with CDH when compared with same population (Table 1).
Adjusted proportions and means of explored factors potentially associated to CDH and episodic headache


NSAIDs, Nonsteroidal anti-inflammatory drugs.
Among people with any headache type, female gender, older age, lower educational level, lower social stratum, migrainous headache, CDH, family history of depression, arterial hypertension, cranial trauma or personal history of suicide attempt, vital stressor events, overuse of analgesics, depression and insomnia complaints were positively associated with CDH (Table 1).
However, in the model generated by multinomial logistic regression, the only persisting positive association factors with episodic headache were female gender, personal history of arterial hypertension or cranial trauma, alcoholism, insomnia, snoring and a higher score in the depression scale, whereas older age appeared as a negatively associated factor. In this same model, female gender, personal history of arterial hypertension or cranial trauma, a history of parents with CDH, complaints of multiple arousals during sleep, use of hypnotics and higher depression scale score were the remaining factors with a positive association with CDH (Table 2).
Multivariate model by multinomial logistic regression to episodic headache and CDH (OR and 95% confidence interval)

The relating category is 18–25 years.
Score between 0 and 80; the referent score is 0 points.
Discussion
This study has shown that in the Colombian general population, some factors are associated with episodic headache as well as CDH. In turn, other factors are associated only with CDH or episodic headache. These conclusions are based on a model generated by multinomial logistic regression that not only controls for confounding and adjusts selection bias, but also keeps in mind the presence of three categories in the outcome variables.
Although this is a cross-sectional study in which a temporary relationship of cause–effect cannot be determined among every associated factor and headache, female gender and parents with a history of CDH clearly precede the development of episodic headache or CDH and can be considered as risk factors. The risk of CDH is three times higher and of episodic headache is twice higher among women, results consistent with previous reports (1–4). The risk increment among women has not been explained by the psychosocial characteristics of females (38), and our results support this hypothesis, because the risk is independent of many of the surveyed factors determined by gender. On the other hand, the higher risk for CDH among women may be due to biological factors, since the recurrent changes of female hormones during the menstrual cycle alter the risk of headache attacks in patients with non-aura migraines and tensional headaches (39–41). Alternatively, men have some protective effect for episodic headache and CDH for similar reasons.
Besides female gender, family aggregation can also be considered to be a risk factor. It was found in this study that people whose parents had CDH have three times more risk for CDH than the general population, but this background is not a risk for episodic headache. This observation has been reported in previous studies (22, 23). This family association may be due to genetic or environmental factors shared by the family; however, family aggregation has not been explained by environmental factors common to the family (22), but by genetic factors (8, 10, 21).
Contrary to family aggregation and gender, it is not possible to outline any temporary relationship with episodic headache or CDH for other investigated associated factors, as each has a different potential explanation. In the first place, the association found between arterial hypertension and episodic headache or CDH had been previously noted in clinical populations (6, 10, 27, 42). Different explanations have been proposed for this comorbidity, as there are many common pathophysiological pathways and genotypes, where headache can be a symptom of hypertension or an adverse effect of antihypertensive medications, or hypertension can be a complication of the overuse of analgesics (27). However, other studies have not found this association (11, 43) or they have found a negative association between hypertension and non-migrainous headache (44). These discrepancies are possibly due to differences in methodology, the population evaluated, or both, indicating the need for future studies to clarify the association and the causal relationship between hypertension, episodic headache and CDH.
Secondly, a history of cranial trauma is 1.6 times higher in episodic headache patients and 3.5 times higher in CDH patients than in the general population. The association between CDH and cranial trauma history had been reported previously (3, 5, 24–26). The mechanism of this association is unclear, but an inverse relationship has been observed between the severity of the cranial trauma and the occurrence of CDH (45); apparently the presence of primary headache before the trauma does not affect the post-traumatic headache risk (25). Our results differ from those of Bekkelund and Salvesen in Norway (46), although this discrepancy can be partly explained by the relatively high prevalence of cranial trauma history among people surveyed in Bucaramanga.
A third associated factor among the population studied regarding episodic headache, as well as CDH, is the score of the Zung's Depression Scale, which is consistent with previous observations (3, 8, 9, 16–21, 47–56). Both migraine and depression or anxiety disorders are more frequent in women and young adults, where genetic factors are important (48). Alterations in monoamine or endorphin systems and chanelopathy are common to these dysfunctions (47, 48). Even though a bidirectional temporary relationship between migraine and depression had already been demonstrated (47), our study has contributed with new information that suggests a gradient dose–response in this causal relationship, with a prevalence that gradually increases with the headache's frequency increment (Table 1).
The relationship between sleep disorders and headache is complex. The results of this study indicate that CDH is associated with complaints of multiple sleep disturbances and the use of hypnotics, since they are more frequent in patients with CDH than in patients with episodic headache or in the population without headache. On the other hand, conciliation insomnia is associated with episodic headache but not with CDH. In the general population (7) and in clinical settings (57, 58) there is an independent association between sleep disorders and headache. Our results contrast with a case–control study made in a clinical setting (11). This discrepancy is possibly explained by differences in methodology.
The association between headache and sleep disorders can have multiple explanations (59). A first explanation is that sleep disorders can produce headache, whereas its treatment alleviates it (60, 61). Nevertheless, the association between headache and some specific sleep disorders, such as obstructive apnoea during sleep, is controversial (62–65). A second explanation is that headache is also frequent in patients with chronic painful syndromes, fibromyalgia and depression or anxiety disorders that frequently cause sleep disorders (59). However, the results of our study have demonstrated that insomnia complaints are associated to episodic headache or CDH independently of depression and vital stressor events. A third explanation of these associations is that headache can cause sleep disorders (57–59).
In adults, lower age has been associated with episodic headache, because the primary headache prevalence, especially migraine, is higher in young people and diminishes with age (66, 67). This explains the finding that an age =36 years is a factor negatively associated with episodic headache. The age of onset of CDH is older than that of primary headaches, which possibly explains the lack of protection for CDH in older patients.
We found an association between episodic headache, but not CDH, and alcoholism or snoring. The association between alcohol consumption and new daily persistent headache compared with patients with migraine has already been demonstrated (10). However, in population-based studies this association has not been documented between alcohol consumption and headache (7) or migraine (49). In turn, snoring has been associated with CDH (15), but, to our knowledge, no population-based studies have reported this association with episodic headache.
Finally, the prevalence of CDH found in this population is significantly higher compared with that previously reported (1–3). The definition of chronic headache could explain, in part, the higher frequency in CDH, since we only required headache occurrence for >15 days a month during at least the last 3 months, instead of 6 months as required in previous studies (1, 3).
There are some discrepancies between our results and previous studies. To begin with, several factors have been associated with CDH: lower social stratum and educational level (1, 3, 5, 13, 14), migraine (3), overuse of analgesics (3, 5, 8, 11, 12), history of alcohol consumption (10), snoring (15) and a history of vital stressor events (1, 5, 7–9). The apparent association in our bivariate analysis disappears in the multivariate one because these factors really are confounding ones or indicate a sequential regression of events, as has been found in other studies (7, 49, 68). In the other hand, caffeine consumption has been reported as a risk factor for CDH (10, 69); however, we have found no such association in our study. Nonetheless, it is not possible to discard caffeine given the great quantity of variables. The size of our sample is not large enough to demonstrate differences in some of these variables on multinomial analysis.
One of the causal factors frequently mentioned in the CDH literature is the overuse of analgesics (3, 5, 8, 11, 12, 28, 29). This study found a high proportion of people with CDH that exhibit this behaviour. However, the cross-sectional nature of the study prevented the examination of this association due to the possibility that the presence of CDH and the overuse of analgesics are two consequences of a common event without being necessarily related in a cause–effect fashion. For this reason, and given the considerable risk of reverse causation, the overuse of analgesics was not included in the multivariate analysis.
The results of this study should be seen with caution. The main limitation is the case definition, since the type of primary headache and CDH was not determined, the presence of arterial hypertension was based on the person's information without measuring the arterial pressure, and the diagnosis of depression and insomnia was based on a test rather than on clinical interview. For these reasons, this survey could express the test population's beliefs about the cause of headaches rather than a real association. This can be especially important for arterial hypertension or cranial trauma. In another way, the information given by the proband on the state of the relatives' illness can have low sensibility, specificity and predictive values (23). In spite of these methodological limitations, this design allows us to study the problem in the general population with a large sample size using low cost indicators, in such a way that this study should be seen as exploratory, the results outlining a hypothesis that needs to be confirmed with more sophisticated and specific researches.
The participation rate in this survey was very high; this has already happened in Colombia. For example, in our validation studies (33, 34) we found similar rates to those detailed in this paper. Also, the World Health Organization World Mental Health Survey Consortium studies, with 28 participating countries, identified Colombia as the country with the highest participation rate (70). The reason may be that in Colombia population surveys are fairly new and are not rejected by the public.
A very interesting finding in this study was the differential behaviour of the factors associated with episodic headache or CDH. Female gender, arterial hypertension history, cranial trauma antecedent and the score of Zung's Depression Scale are factors associated with both conditions, with a dose–response gradient showing higher prevalence with the increment of headache frequency (Table 1). These results suggest that episodic headache and CDH behave as a continuous spectrum of severity (e.g. episodic migraine–chronic migraine or episodic tension-type headache–chronic tension-type headache). However, some factors are associated only with CDH, but not with episodic headache. In turn, other factors are associated with episodic headache but not with CDH. These discrepancies in the associated factors between the two entities indicate the possibility that CDH is different from the primary homologous episodic headache; or, alternatively, that the induction mechanisms of primary episodic headaches and transformation mechanisms from primary episodic headaches to CDH are different, ruled by the influence of different risk factors. A finding that supports this hypothesis is the fact that there are differences in gene expression in patients with acute attacks of episodic migraine and chronic migraine (10).
In conclusion, this survey has shown that the episodic primary headache and CDH share some common associated factors. However, there are associated factors that are exclusive to primary headache or CDH. These results suggest that CDH is related to primary homologous headaches, but the pathophysiological mechanisms are different.