
Abstract
We present a prospective study of 240 patients with medication overuse headache (MOH) treated with drug withdrawal and prophylactic medications. At 1-year follow-up, 137 (57.1%) patients were without chronic headache and without medication overuse, eight (3.3%) patients did not improve after withdrawal and 95 (39.6%) relapsed developing recurrent overuse. Age at time of MOH diagnosis, regular use of benzodiazepines, frequency and Migraine Disability Assessment (MIDAS) score of chronic headache, age at onset of primary headache, frequency and MIDAS score of primary headache, ergotamine compound overuse and daily drug intake were significantly different between successfully and unsuccessfully treated patients. Multivariate analysis determined the frequency of primary headache disorder, ergotamine overuse and disability of chronic headache estimated by MIDAS as independent predictors of treatment efficacy at 1-year follow-up.
Introduction
The clinical features of drug-induced headache were first described for ergotamine intake in 1951 (1) and since the 1970s also for analgesics and other compounds. There is now substantial evidence that all drugs used for the treatment of headache can cause medication overuse headache (MOH) in patients with primary headache disorders (2). The overuse of analgesics or symptomatic migraine drugs in patients with a pre-existing primary headache disorder is often associated with the development of a new type of headache or worsening of migraine or tension-type headache causing chronic daily headache (CDH). The International Classification of Headache Disorders (ICHD) recognizes MOH as a separate headache entity and, in the second edition, defines ergotamine, triptan, analgesic, opioid and combination medication overuse as intake of these drugs on ≥10 days/month and simple analgesics on ≥15 days/month for >3 months (3). These criteria have been further revised by adding a new subform of MOH attributed to combination of acute medications that takes into account patients overusing medications of different classes but not any single class (4).
MOH is a largely underdiagnosed health condition, but its prevalence is increasing worldwide and it has become the third most frequent type of headache (2, 5). According to recent epidemiological studies, the prevalence in the general population is 1–1.4%, with peak prevalence in women in their 50s. In this age range, in fact, 5% of women meet the diagnostic criteria of MOH (6, 7).
Drug withdrawal is the treatment of choice for MOH, with various treatment strategies (2, 8) followed by the establishment of prophylactic medication. The literature contains few long-term observational studies investigating the risk of relapse into overuse. Schnider et al. (9), reporting the longest follow-up to date, found that 39.5% of patients relapsed into drug overuse. In a prospective study, conducted after the introduction of the triptans into clinical practice, Katsarava et al. (10) showed that relapse into overuse occurred within 6 months of detoxification in 31% of patients, and within a year in 36%; the same author, in a subsequent study (11), reported a relapse rate of 45% at 4 years. Overall, the literature data seem to indicate that there is a high risk of relapse in the first year following detoxification.
The aims of the present study were the evaluation of treatment efficacy in a sample of MOH patients treated in our Headache Centre and the identification of possible predictors of treatment failure.
Patients and methods
Five-hundred and thirty-five patients with CHD were examined between January 2000 and July 2005 at the Headache Centre of the Institute of Neurology, Clinical Centre of Belgrade, Serbia, the tertiary national referral centre. Chronic headache with medication overuse were diagnosed in 321 (59.9%) of these patients according to ICHD-II criteria (3) and the revision of these criteria (4).
Patients with a previous history of overusing medications different than those currently being overused (n = 22) were excluded. Fifty-nine patients were lost for follow-up, so a total of 240 subjects were eligible for the study.
For every MOH patient the following information was recorded from different sources. Demographic data, features of chronic headache disorder [frequency expressed as number of days with headache per month, pain intensity measured by visual analogue scale (VAS) 0–10, daily headache duration expressed in hours, disability measured by Migraine Disability Assessment (MIDAS)], type of overused medications, daily drug intake and side-effects of overuse; concomitant use of benzodiazepines; overuse of caffeine defined as daily intake of more than three cups of coffee, smoking and lack of physical activity, as well as positive family history for headaches, were obtained from patients' headache diaries and headache questionnaires. The features of chronic headache disorder were re-examined on every 3-month follow-up by a neurologist–headache specialist (J.Z-T.). The clinical features of primary headache disorder (age at onset, frequency expressed as number of days with headache per month, pain intensity measured by VAS 0–10, daily headache duration expressed in hours, disability measured by MIDAS) were collected retrospectively, from the patient's personal history, i.e. from medical records whenever possible. The primary headache was diagnosed as migraine if the diagnostic criteria for migraine, according to ICHD-II criteria (3), were satisfied. Otherwise, the diagnosis of tension-type headache was applied.
Overused medications were non-steroidal anti-inflammatory drugs (NSAIDs) including acetylsalicylic acid; combination medications (COM) containing paracetamol or aspirin combined with caffeine; ergot compounds containing ergotamine-tartarate solely or combined with caffeine; and triptans. All medications were classified as migraine specific (ergots and triptans); or non-specific (NSAIDs, COM or opioids). All patients underwent neurological examination and brain imaging by computed tomography or magnetic resonance imaging.
The treatment of acute medication overuse at the Headache Centre includes in- and out-patient detoxification from offending agents and initiation of preventive drug therapy. During interview following the establishment of MOH diagnosis, the mechanisms of overuse headache and features of withdrawal headache were explained to the patient. All the patients were strongly advised to withdraw overused medication and those who considered that they could not do so by out-patient treatment were admitted to hospital. The patient was then submitted to infusion-detoxification therapy daily throughout the period of hospitalization (average 8 days). Our treatment protocol includes repetitive dihydroergotamine infusions, metoclopramide for nausea and diclofenac for pain control adjusted according to the patient's cardiovascular status. Preventive therapy is initiated during the hospital stay. The choice of preventive drug was based on physician assessment and patient's comorbidity. Standard preventives were used: amitriptyline, fluoxetine, propranolol, verapamil or divalproex sodium. The decrease of headache frequency by ≥50% or return of headache features to primary headache disorder associated with discontinuation of medication overuse were considered as an effective treatment at 1-year follow-up. These patients formed Group 1. Patients who had not improved after detoxification or were returned to a pattern of medication overuse within 1 year formed Group 2.
Both groups were compared regarding treatment outcomes by demographic data, headache features, overused medication and detoxification strategies.
The data are presented as arithmetic mean ± SD or as percentages. The Kolmogorov–Smirnov test was applied to assess the normality of the studied continuous data. Independent-samples t-test and χ2 test were used to compare data between the two groups. The significance level for the analysis was set at 5% (P < 0.05). Univariate and multivariate logistic regression (stepwise method) was applied to determine the outcome predictors. The outcome variable was treatment effectiveness at 1-year follow-up, as defined above. The criterion for variables inclusion in multivariate model was statistical significance at the level of P ≤ 0.05, obtained by univariate analysis.
Results
Our sample consisted of 240 patients diagnosed with MOH. Of the 240 subjects included in this study, 182 (75.8%) were female; mean age 41.5 years (range 17–76); mean follow-up period 3.4 years (range 1–6). Diagnosis of primary headache was migraine in 161 (67.1%) and tension-type headache in 79 (32.9%) patients.
The majority of patients were overusing one substance (55.0% of patients), but 108 (45.0%) overused two or more different compounds at a time: two (33.8%), three (10.4%) or four (0.8%).
The most common overused medications were NSAIDs 62 (25.8%) followed by COMs 52 (21.7%) for patients with overuse of one medication and the same medications in reverse order: COM 95 (88.0%) and NSAIDs 85 (78.7%) for patients with overuse of more than one medication. Ergotamine compounds alone were overused by 16 (6.7%) patients and by 39 (36.1%) in combination with other overused medications. Only one (0.4%) patient overused only opioid medicatons or triptans, whereas these medications were overused in combination with other medications by six (5.6%) and 20 (18.5%) patients, respectively.
Non-specific analgesics were the most common overused medications, overused by 170 (70.8%) patients, whereas 22 (9.9%) overused only migraine-specific medications and 48 (20.0%) overused non-specific as well as specific medications.
At 1-year follow-up, 137 (57.1%) patients were without chronic headache and without medication overuse and formed Group 1. One hundred and three (42.9%) patients had CDH with medication overuse, including eight (3.3%) patients who did not improve 1 month after withdrawal and 95 (39.6%) who relapsed developing recurrent overuse within the first year following detoxification (Group 2).
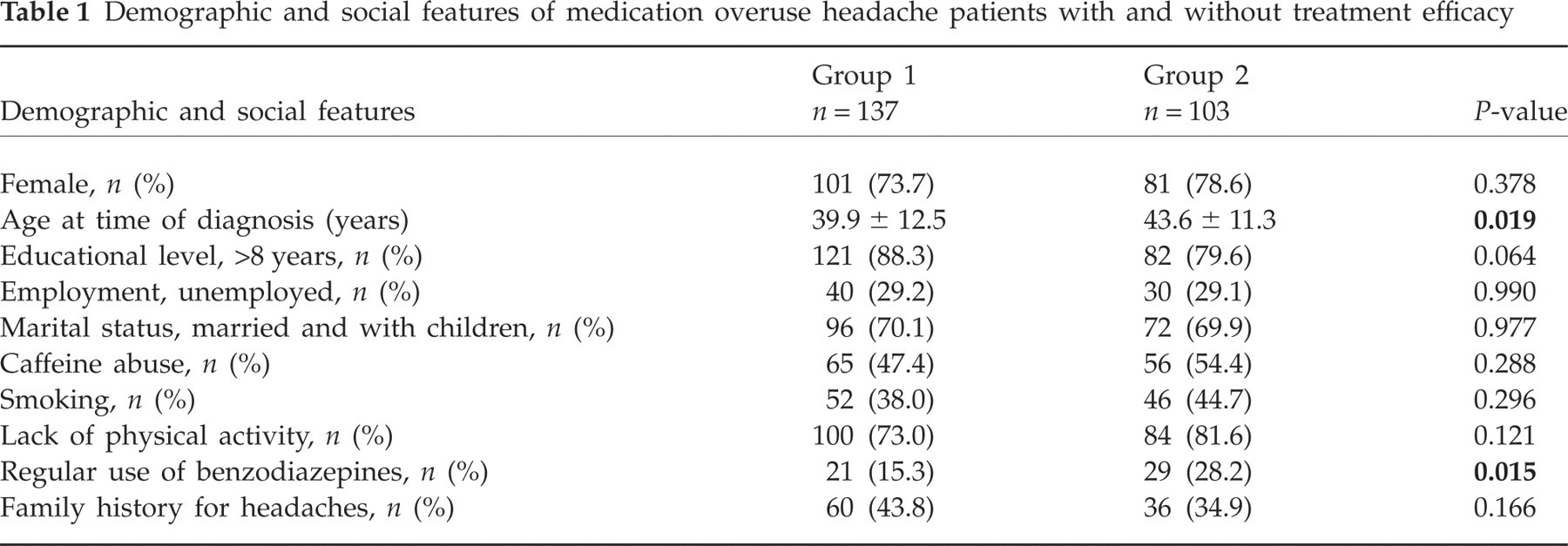
Unsuccessfully treated MOH patients were older (43.6 ± 11.3 years) than those successfully treated (39.9 ± 12.5 years, P = 0.019). Regular use of benzodiazepines was more frequent in unsuccessfully (28.2%) than in successfully treated patients (15.3%, P = 0.015). No significant difference was found in other demographic and social features between the two groups (Table 1).
Demographic and social features of medication overuse headache patients with and without treatment efficacy
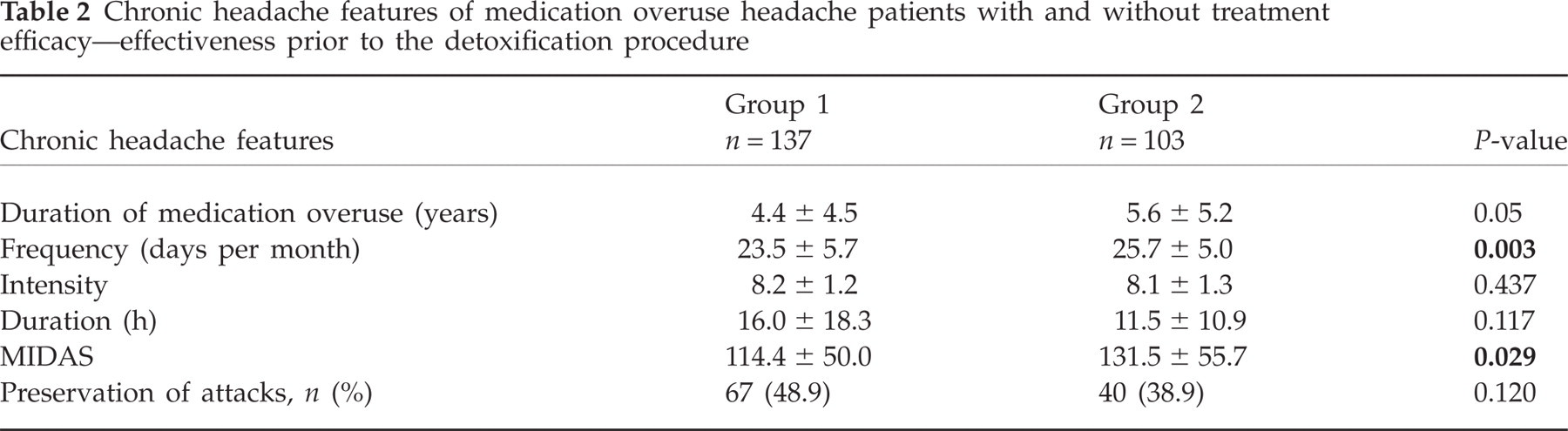
The mean monthly headache frequency (25.7 ± 5.0 vs. 23.5 ± 5.7, P = 0.003) and mean MIDAS (131.5 ± 55.7 vs. 114.4 ± 50.0, P = 0.029) were higher in unsuccessfully treated than in successfully treated patients. No significant difference was found in duration of medication overuse, headache intensity or duration of daily headaches (Table 2).
Chronic headache features of medication overuse headache patients with and without treatment efficacy—effectiveness prior to the detoxification procedure
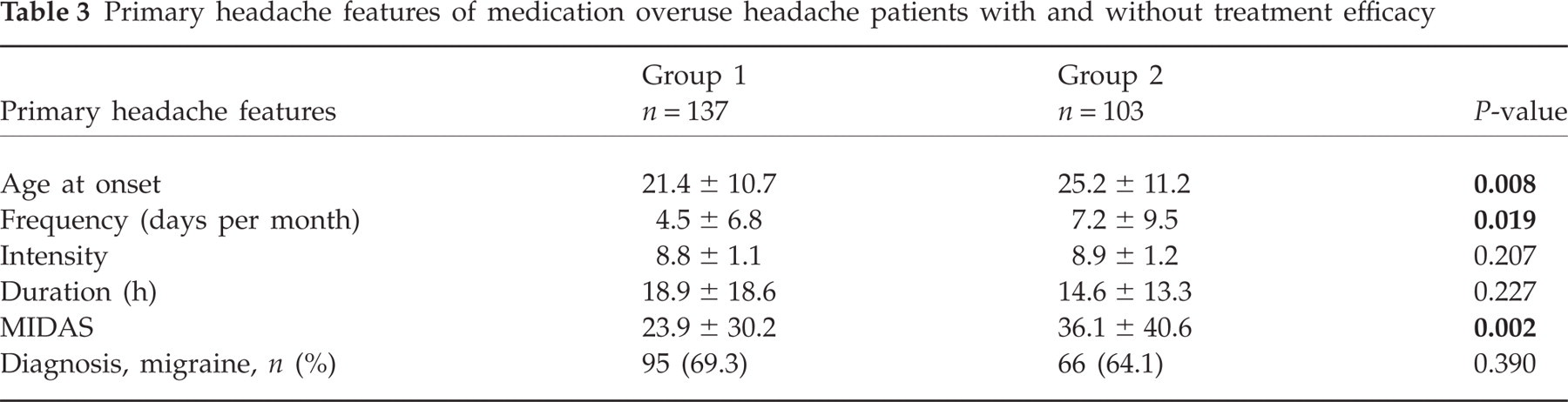
Unsuccessfully treated patients were older at onset of primary headache disorder (25.2 ± 11.2) than successfully treated patients (21.4 ± 10.7, P = 0.008). Mean primary headache frequency (7.2 ± 9.5 vs. 4.5 ± 6.8, P = 0.019) and mean MIDAS (36.1 ± 40.6 vs. 23.9 ± 30.2, P = 0.002) were higher in unsuccessfully treated than in successfully treated patients. No significant difference was found in intensity or duration of primary headache disorder. Migraine was equally represented in both groups (Table 3).
Primary headache features of medication overuse headache patients with and without treatment efficacy
Ergotamine overuse was more frequent in unsuccessfully treated (29.1%) than in successfully treated patients (18.2%, P = 0.047). No significant difference was found in other types of overused medication between the two groups. Daily drug intake was significantly higher in unsuccessfully treated (2.0 ± 1.5) than in successfully treated (1.6 ± 1.3, P = 0.006) patients. Gastrointestinal disturbances, as a consequence of medication overuse, were presented in both groups of patients, complicated in two patients with gastrointestinal bleeding and loss of consciousness (Table 4).
Overused medications of medication overuse headache patients with and without treatment efficacy

NSAIDs, Non-steroidal anti-inflammatory drugs; COMs, combination medications.
No significant difference was found in detoxification strategy between successfully and unsuccessfully treated patients, and out-patient treatment was equally presented, 35% (48/137 vs. 36/103, P = 0.989) in both groups.
Age at time of MOH diagnosis, regular use of benzodiazepines, frequency and MIDAS of chronic headache, age at onset of primary headache, frequency and MIDAS of primary headache, ergotamine compound overuse and daily drug intake were significantly different between the two groups and were further analysed by multivariate method. The results of multiple logistic regression analysis are presented by Table 5. Primary headache frequency, ergots overuse and chronic headache MIDAS had significant independent effects on treatment outcome.
Variables extracted by multivariate analysis

Odds ratio.
95% confidence interval.
Discussion
The group examined in this study consisted of 240 MOH patients and was representative of 60% of patients with CDH treated during a 5-year period in our Headache Centre. Epidemiological studies have shown that approximately 4% of individuals have >15 days of headache per month (12), and at least 30% overuse acute medications, which suggest that the prevalence of MOH is 1% in the population (13). The relative frequency of MOH is much higher in tertiary care centres. In Europe, up to 10% of patients referred to headache clinics have this diagnosis (14), but this could be even greater, as reported by Bekkelund in a recent survey of patients treated in a Norwegian neurological centre, where he found that 28% of consecutive headache patients used analgesic drugs on a daily basis (15). In the USA up to 60% of patients seen in headache clinic have MOH and the proportion of these patients did not changed over the 15-year period (16).
Demographic and social features of our MOH patients are similar to those of MOH patients reported by others (2, 5, 6, 16): >70% were female, age at time of diagnosis was about 40 years, duration of medication overuse varied between 3 and 4 years and great majority were well educated, employed and married.
The type of medications overused by our patients was different from that overused by MOH patients that had been analysed by other authors, confirming the statement that the use of drugs that lead to MOH varies substantially from country to country and is influenced by cultural factors (2). The majority of our patients (55%) were overusing the same single substance over the years. The most common overused medications were simple and combined analgesic medications overused by >80% of our MOH patients. Only a small proportion of patients (3%) overused opioid medications. Combination analgesic medications with butalbital and codeine are not in such common use in our country as in the USA (16). The regular use of benzodiazepines was analysed separately, showing significant influence on treatment outcome on univariate, but not on multivariate analysis. Analysis of specific acute migraine medications revealed that a significant proportion of patients (23%) still overused ergotamine and that triptans were overused by only 9% of our MOH patients. Contemporary studies from European authors have shown decreasing numbers of ergotamine-induced headache and increasing numbers of triptan-induced headache (2, 10, 14). However, ergotamine overuse remains an important problem in Europe and South America (17, 18).
Treatment success, defined as absence of daily headaches and medication overuse, was detected in 57% of our MOH patients at first-year follow-up. In meta-analysis including 17 studies with 1101 patients, performed by Diener and Limmroth, the mean success rate of withdrawal therapy within the time window of 1–6 months was 72.4% (2). The somewhat lower success rate obtained by the present study could be explained by patient bias, because our Headache Centre serves as a tertiary referral centre for difficult-to-treat headache patients from the whole country. In our patients the relapse rate of recurrent overuse with development of chronic headache was nearly 40% during the first year, comparable to results of other studies. Rates of relapse of 22–44% were found during the first year of an initially successful withdrawal therapy (10, 19, 20).
According to results obtained by our study, the frequency of primary headache disorder (P = 0.008), ergotamine overuse (P = 0.012) and disability of chronic headache estimated by MIDAS (P = 0.045) are independent predictors of treatment efficacy at 1-year follow-up. The patients with lower primary headache frequency had better treatment outcome. Development of MOH in patients with migraine and tension-type headache leads to the conclusion that MOH is an interaction between an excessively used therapeutic agent and a susceptible patient (3). In the present study the data concerning the chronic headache features were collected from patients' diaries, whereas the data of primary headache features are obtained retrospectively from patients' personal histories and so should be interpreted with caution. However, treatment failure in the patients with high primary headache frequency, as well the small but important number of patients who could not be successfully detoxified, favour the hypothesis that there is a subgroup of patients with primary headache with a less benign course of the disorder. The other features of primary headache such as pain intensity and attack duration, disability and age at onset were not predictive of treatment outcome in our patients. According to our results, the type of primary headache disorder was not predictive of outcome. Patients with tension-type headache as their primary headache entity had a significantly higher relapse rate than those with migraine in the studies of Katsarava et al. (10, 11).
Ergotamine overuse was an unfavourable predictor of treatment outcome in our patients. At 1-year follow-up, 29% of patients with treatment failure overused ergots in comparison with 18% of patients who where MOH free. Katsarava et al. found that the patients who overuse analgesics, predominantly combination analgesics, have significantly higher relapse rates than those who overuse ergots or triptans (10). Only a minority of our patents overused specific antimigraine drugs. On the other hand, multiple receptor properties of ergotamine with multiple types of action leading to effective pain control could also be responsible for more profoundly altered pain control mechanisms in CDH patients (21). The overuse of other medications, the number of overused medication, duration of overuse and daily drug intake did not influence the treatment outcome in our patients.
The third predictor of treatment outcome was the chronic headache MIDAS of our patients. Successfully treated patients had a 20 points lower MIDAS score than those who were unsuccessfully treated. The MIDAS questionnaire is an extensively studied and well-validated measure of headache-related disability (22). This score was constructed to assess disability for episodic headache disorder, but can also be used for patients with chronic headache disorders (23, 24). At first glance, MIDAS in mostly dependent on headache frequency; however, MIDAS entered the final predictive model, whereas the chronic headache frequency was significant only on univariate analysis. This result suggests that the functional impairment is present even on days without headache in MOH patients. There is limited knowledge about headache-related disability in chronic headache with medication overuse and how this disability subsequently influences treatment. On the other hand, the clinical evidence suggests that successful treatment has more wide-ranging positive benefits beyond mere symptom reduction, even for this difficult-to-treat population (25).
It is also worth noting that there was no difference between numbers of MOH patients treated successfully by advice and of successfully treated in-patient MOH subjects. This result of our study is in accordance with those obtained by other studies (26) and allows patient choice of the mode of treatment.