
Abstract
This study examined the clinical picture of probable medication-overuse headache (MOH) and the presence of any features peculiar to Japan. In a retrospective study of 47 patients, type of primary headache, type of medicine overused, method and result of withdrawal were investigated. Among the 47 patients, 80.9% had migraine only, and 85.1% overused combination medications. While 36 patients (76.6%) succeeded in withdrawal, five patients (10.6%) failed. One patient (2.1%) had not improved by 2 months after withdrawal and was diagnosed with chronic migraine and chronic tension-type headache without MOH. The remaining five patients (10.6%) dropped out. All dropout patients were recommended abrupt inpatient withdrawal, but chose abrupt outpatient withdrawal. As features peculiar to Japan, many patients with probable MOH overused combination analgesics, particularly females.
Introduction
Chronic headache caused by frequent use of analgesics, ergots or triptans represents a well-recognized disorder. In 1988, the Internal Headache Society (IHS) defined drug-induced headache as chronic headache occurring after administration of large quantities of analgesics or ergots, and disappearing after withdrawal of the substance (1). To emphasize the regular intake of pharmacotherapies, medication-overuse headache (MOH) was defined in the internal classification of headache disorders 2nd edition (ICHD-II) in 2004 (2) and subsequent revision (3). MOH can be divided into eight subforms: ergotamine-overuse headache; triptan-overuse headache; analgesic-overuse headache; opioid-overuse headache; combination analgesic-overuse headache; medication-overuse headache attributed to combination of acute medications; headache attributed to other medication overuse; and probable MOH. Combination analgesic medications are those containing simple analgesics combined with opioids, butalbital and/or caffeine. MOH can technically only be diagnosed after completion of withdrawal. Patients who overuse medication can thus only be diagnosed with probable MOH on first consultation.
MOH is a common worldwide problem in clinical practice. This problem is also seen in Japan, although few Japanese studies have examined MOH in the absence of analgesic-abuse headache (4). Opioids cannot be used for headache without terminal cancer pain and no barbiturate-containing combination products are available in Japan. Therefore, neither opioids nor barbiturates are contained in combination analgesics that are available in Japan. Frequencies of overused medications in Japan may thus differ from those in other countries.
This study aimed to clarify the clinical picture of probable MOH and reveal any features peculiar to Japan.
Methods
Subjects comprised 47 consecutive patients (41 women, 6 men; mean age, 42.0 years; range, 20–75 years) who were diagnosed with probable MOH according to ICHD-II on first consultation. Patients with secondary headache other than MOH were excluded. Type of primary headache, type of overused medication, method of withdrawal, and result of withdrawal were examined. Primary headache was diagnosed according to ICHD-II. Type of overused medication was classified according to ICHD-II criteria as: ergotamine; triptan; analgesic; opioid; combination analgesic; combination of acute medications; or other medication. Method of withdrawal was classified as: abrupt outpatient withdrawal; abrupt inpatient withdrawal; or tapering outpatient withdrawal. We initially recommended that overused medication should be discontinued abruptly on an outpatient basis. Patients with low motivation or who took tranquilizers, were depressed or had failed previously to withdraw were recommended to undergo treatment as inpatients. If the patient disagreed with abrupt outpatient withdrawal, abrupt inpatient or tapering outpatient withdrawal was attempted. Amitriptyline 10–20 mg daily was prescribed for management of rebound headache. Fluid replacement, antiemetics and tranquilizers were used to treat withdrawal symptoms. For management of primary headache, we prescribed lomerizine 10–20 mg/day for prophylaxis of migraine and triptans to treat migraine attack. Success of withdrawal was judged based on complete resolution of chronic headache and analgesic use on < 10 days/month within 2 months after discontinuation of overuse medication. Patients who stopped regular treatment without permission and could not be contacted were evaluated as dropout cases.
Statistical analysis
StatView version 5.0 for Windows software (SAS Institute, Cary, North Carolina, USA) was used for statistical analysis. Age, sex, type of primary headache, type of overused medication, method of withdrawal, result of withdrawal and prognosis after withdrawal were compared. Comparisons between two samples were made using the χ2 test, Kruskal–Wallis test and Mann–Whitney U-test whenever applicable. Values of P < 0.05 were considered statistically significant.
Results
Among the 47 patients, 38 patients (80.9%) displayed migraine only, two patients (4.3%) had tension-type headache only, and seven patients (14.9%) had combined migraine and tension-type headache. The overused medication was combination analgesic in 40 patients (85.1%), analgesic in four patients (8.5%), ergotamine in one patient (2.1%), triptans in one patient and a combination of acute medications in one patient. No patients overused opioid or other medications. Combination analgesic was overused by females significantly more often than by males (Table 1). Abrupt outpatient withdrawal was recommended for 37 patients (78.7%) and all these patients agreed to this approach. Abrupt inpatient withdrawal was suggested for and agreed to by two patients (4.3%). Another six patients (12.8%) were recommended abrupt inpatient withdrawal, but chose abrupt outpatient withdrawal. Finally, two patients (4.3%) were recommended abrupt inpatient withdrawal, but chose tapering withdrawal. While 36 patients (76.6%) succeeded in withdrawal, five patients (10.6%) failed. One patient (2.1%) had not improved by 2 months after withdrawal and was diagnosed with chronic migraine and chronic tension-type headache without MOH. The remaining five patients (10.6%) dropped out. All dropout patients were recommended abrupt inpatient withdrawal, but chose abrupt outpatient withdrawal. The two patients who chose tapering withdrawal were not able to withdraw from overuse medication (Table 2). The overused medications of patients who failed comprised combination analgesics (n = 3), ergotamine (n = 1) and analgesic (n = 1) (Table 3).
Type of overused medication and sex
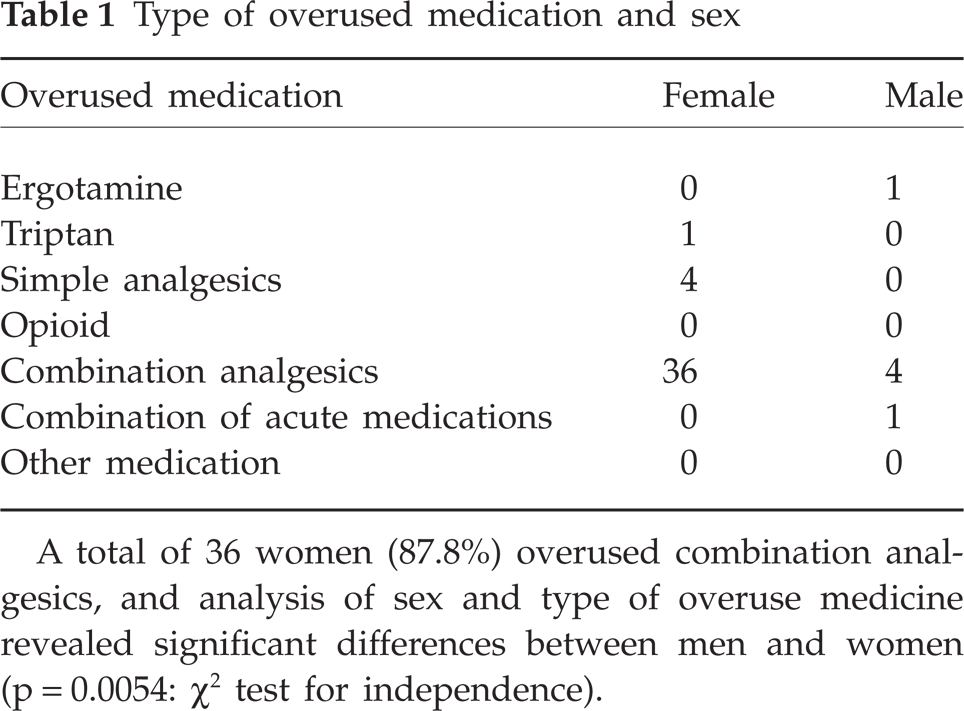
A total of 36 women (87.8%) overused combination analgesics, and analysis of sex and type of overuse medicine revealed significant differences between men and women (p = 0.0054: χ2 test for independence).
Method of withdrawal and results

Out: abrupt outpatient withdrawal. In: abrupt inpatient withdrawal. Tapering: tapering (outpatient) withdrawal. No patients who attempted tapering withdrawal were able to withdraw from overuse medication.
Results of withdrawal and type of overused medication

Combination analgesics are those containing simple analgesics combined with caffeine or other agents. Combination of acute medications represents intake of any combination of ergotamine, triptans and/or analgesics.
Discussion
Among the 47 patients with probable MOH, 80.9% of primary headaches were migraine. In a previous study, migraine was present in 76.8% of patients with analgesic-abuse headache (4) and 73% of patients with MOH (according to IHS criteria) (5). Our findings were similar to these studies regarding proportions of primary headache. Conversely, distributions for type of overused medication have differed substantially between reports. Our study showed that the majority of cases involved combination analgesics (85.1%), with only 2.1% involving triptan. A study by Pini et al. found that combination medication and analgesics were occupied about 40% (6), while another study showed that 48% overused analgesics and 38% overused triptans (7). A recent report noted that the majority of patients overused more than one type of medication (8). In that report, barbiturate-containing combination products were involved for 48% of patients and opioids were involved for 33.3%. Differences in frequently overused medications may reflect differences in social and cultural factors. Triptan has only entered the market relatively recently in Japan (injection since 2000 and tablet since 2001). The finding of triptan overuse in only 2% in this study was thus probably unsurprising. In Japan, 56.8% of migraine sufferers use over-the-counter medicine alone, with only 5.4% taking prescribed medicine alone (9). Many over-the-counter analgesics in Japan are combination medications. Moreover, combination medication is more likely to trigger rebound than single analgesic (5, 10). These factors could explain the finding of combination medication overuse in many patients.
Our study showed that females were significantly more likely to use combination medications. This may be due to the fact that many combination medications are sold for headache and menstrual pain.
Strategies for dealing with withdrawal from medication overuse can be divided roughly into out- and inpatient programs. Suhr et al. (10) reported that neither method of withdrawal therapy nor kind of medication overused exerts a major impact on long-term results after successful withdrawal therapy. Hering and Steiner (11) reported that withdrawal can be achieved in outpatients with adequate explanation and close follow-up. Opioids and barbiturates should be tapered to avoid risk of severe withdrawal syndrome (12, 13). In Japan, over-the-counter combination medications contain analgesics (e.g. aspirin, acetaminophen, ethenzamide, ibuprofen, isopropylantipyrine) and other substances such as caffeine, bromovalerylurea and allylisopropylacetylurea. Opioids and barbiturates are not contained in combination medications. As no danger of withdrawal syndrome due to opioids or barbiturates was present, we recommended abrupt outpatient withdrawal for all patients without low motivation, tranquilizer use, depression or previous failure to withdraw.
Mean success rate of withdrawal therapy within a time window of 1–6 months is 72.4% (12), similar to our own finding of 76.6%. Tapering withdrawal yielded poor results in a previous study (4), and patients using tapering withdrawal also displayed poor prognosis in this study. Inpatient withdrawal was recommended for these patients. Furthermore, five of the six patients who were recommended inpatient withdrawal and disagreed eventually dropped out. Finally, the success rate of patients who did not agree to hospital treatment was only 12.5%. Given these results, we should more positively recommend hospitalization to patients with low motivation or who take tranquilizers, are depressed or have previously failed to withdraw.
We prescribed lomerizine for prophylaxis in migraine. Lomerizine is a calcium-channel antagonist that was developed as an antimigraine drug in Japan (14). Lomerizine is recommended as the first-line prophylactic drug, as this agent is licensed as a preventive drug for migraine in Japan. Efficacy of lomerizine at 12 weeks was 48–71% (15, 16), and long-term efficacy (mean follow-up, 17.7 months) was 74% in our small prospective study (17). Further studies are needed to clarify the efficacy of lomerizine for relapse.