
Abstract
We recently reported an increase in prevalence and frequency of tension-type headache (TTH) over a 12-year period in the young Danish population. The aim of the present study was to analyse whether this increase was related to increased pain sensitivity. The study was a cross-sectional replicate of a large Danish population study. It compared 113 subjects aged 25-36 years in 2001, with 221 comparable subjects in 1989. Tenderness was considerably higher in 2001 than in 1989. When stratified according to presence of headache, the increase in tenderness was clinically and statistically significant only in women with frequent TTH. The pressure pain threshold was significantly lower in 2001 compared with 1989 in women with frequent TTH. The increase in tenderness in the population may predict an even higher prevalence of TTH in future. The changes support the hypothesis of central sensitization in TTH.
Introduction
Mechanisms responsible for increased pain sensitivity in tension-type headache (TTH) are clinically very important for prevention and treatment strategies, but unfortunately not well understood. Prolonged nociceptive input from the periphery may sensitize the central nervous system (CNS) and, thereby, lead to increased pain sensitivity and a change from episodic tension-type headache (ETTH) to chronic tension-type headache (CTTH) (1–4). However, the pathophysiological mechanisms have almost exclusively been studied in highly selected patients from headache clinics.
In 1989, a population-based study of primary headache disorders and pain perception was conducted, combining diagnostic headache interview and examination of muscle tenderness and measurement of pressure pain thresholds (PPT) in 1000 persons drawn randomly from the general population in Denmark (5, 6). In 2001, we initiated a study designed as an extension of the 1989 study, including both a cross-sectional replicate study and a follow-up study of the 1989 cohort. In a recently published paper from the cross-sectional part of the study, it was reported that the prevalence and frequency of TTH had increased in the young general population over the 12-year period (7). The suggested pathophysiological mechanisms in TTH make it interesting to analyse whether this increase was related to increased pain sensitivity, which was the aim of the present study.
Materials and methods
The 1989 cohort
One thousand residents in the County of Copenhagen, aged 25–65 years, were randomly selected from the Danish Civil Registration system. In total, 735 of 975 (75.4%) eligible participated in the headache diagnostic interview and examination of muscle tenderness and pain threshold. The age and gender distribution of the participants was representative of the cohort and of the background population. Methods and results from this study are described in detail elsewhere (5, 6, 8). Of the 975 eligible subjects, 294 corresponded to the age span (25–36 years) of the participants in the present cross-sectional part of the 2001 study.
The 2001 cohort
In the cross-sectional replicate of the 1989 study, 300 new subjects aged 25–36 years were selected by the same criteria as in 1989. The 300 new subjects were, as in 1989, invited to participate in a headache interview and in a clinical examination of total tenderness score (TTS) and PPT. If no response was obtained, completion by telephone of a reduced version of the headache interview was attempted, and in these cases no clinical examination was performed. Detailed methodological information is presented elsewhere (7). Of the 300 new subjects, three were not eligible due to errors in the address list.
Interview
The headache interview consisted of a semistructured face-to-face interview focusing on primary headaches. All interviews were conducted by a medical doctor both in 1989 and in 2001. Each different form of headache within the last year was diagnosed based on the 1988 International Headache Society criteria (9). According to ICHD-2 (10), ETTH was subsequently subdivided in infrequent ETTH (IETTH) and frequent ETTH (FETTH) (for detailed description see (7)).
To study the pure primary headache diagnoses, migraineurs with coexisting FETTH or coexisting CTTH were excluded from the analysis of migraine and subjects with coexisting migraine were excluded from the analyses of FETTH and CTTH.
In the present paper the category ‘no headache’ includes subjects without primary headache or with IETTH, the category TTH thus includes subjects with FETTH or CTTH and the category ‘coexisting headaches’ includes subjects with both TTH and migraine.
Examination
The examination was performed using a standardized method by the same examiner through the entire study and was recorded on computer-ready forms. The examiner in 1989 was a specially trained dentist (M.S.) and in 2001 a specially trained nurse (V.T.). No information about the subject's headache history was available to the examiners and each subject was unknown to them. The participants were examined sitting in a comfortable dental chair with headrest.
Palpation method (TTS)
As in 1989, pericranial tenderness was evaluated by palpation of eight pairs of muscle and tendon attachments (frontal, temporal, masseter, lateral pterygoid, sternocleidomastoid and trapezius muscles, mastoid process and neck insertions). The tenderness was scored according to the TTS (11) with a scale from 0 to 3, which has previously proved to be reliable (12). For each participant a TTS was calculated by summation of the scores from the eight right- and left-sided locations (maximum possible score = 48) and a local tenderness score for each of the eight pairs of pericranial locations was calculated by summation of right plus left side. Prior to the study in 2001, a palpometer was used to train the observer to exert a palpation pressure of moderate intensity (140 U). The palpometer has been described in detail elsewhere (13)
Pressure pain threshold (PPT)
As in 1989, PPT was measured at the anterior part of the temporal muscle where palpation had revealed it to be most prominent. Measurements were performed at the non-dominant side (ambidextrous were measured on the left side) using a pressure algometer (Somedic AB, Hörby, Sweden) with a circular stimulation probe (0.5 cm2) and a pressure loading rate of 0.68 N/s (14). PPT was defined as the pressure at which the sensation changed from pressure alone to a combination ofpressure and pain. A median value of three measurements was used to calculate the individual PPT.
Data analysis and statistics
The primary end-point was differences in TTS and PPT between 1989 and 2001 in total population. Secondary end-points were to analyse if the differences in TTS and PPT were related to headache diagnoses. Distribution of the data was analysed by Kolmogorov–Smirnov test for normal distribution. Normally distributed data (TTS) are presented as mean values and differences between groups are presented as mean difference (Δ) with 95% confidence intervals (CIs) in parentheses.
Data (PPT) that were not normally distributed were transformed into decadic logarithms to achieve normal distribution (secondary normalization). Analyses were performed on these log-transformed data. Mean values of the transformed data were back-transformed to the original scale of measurement, whereas the mean difference (Δt) between groups and the CI (in parentheses) are presented in transformed values. T-test for independent samples was used to test differences in TTS and PPT between groups. When normalization of the data was not possible (local tenderness score), data were analysed by non-parametric statistics (Mann–Whitney test).
The participation pattern and the differences in headache frequency between groups were analysed using the χ2 test. Statistical analyses were performed using SPSS, version 12.0 software (SPSS Inc., Chicago, IL, USA). Five percent was taken as the level of significance.
Results
Study population
Baseline characteristics of the study population are presented in Table 1. In 1989, 221 of the 294 (75%) eligible subjects aged 25–36 years participated in the headache interview. Of these, 217 also participated in the clinical examination of TTS and PPT (in the following classified as participants in the 1989 study). In 2001, 207 of the 297 (70%) eligible subjects participated in the headache interview. Of these, 113 also participated in the clinical examination of TTS and PPT (in the following classified as participants in the 2001 study). The participants were representative of the study population with regard to gender both in 1989 and in 2001 (χ2: 1989, P = 0.8; 2001, P = 0.1). Whereas almost all (98%) (217/221) who completed the headache interview in 1989 participated in the clinical examination, only 55% (113/207) did so in 2001. However, there was no difference in headache profile between subjects who completed only the headache interview and participants in the 2001 study (χ2: P = 0.5).
Study population

N, Number of subjects (male/female ratio), [% of the participants].
TTH, Tension-type headache; CTTH, chronic tension-type headache; FETTH, frequent episodic tension-type headache.
In 1989, 12 of the participants had pure migraine, 54 had pure TTH, 13 had coexisting headaches and 138 had no headache. In 2001, seven participants had pure migraine, 39 had pure TTH, 12 had coexisting headaches and 55 had no headache. Because the number of participants who had migraine or coexisting headaches was very low, we have stratified only according to presence or absence of TTH when relation to headache is analysed in the following.
In women, the prevalence of CTTH among subjects with TTH was significantly higher in 2001 compared with 1989 (1989: CTTH : FETTH = 1 : 35; 2001: CTTH : FETTH = 6 : 22; χ2: P = 0.02), whereas no such difference was seen in men (χ2: P = 0.7).
Gender differences
Compared with men, women were significantly more tender [1989: 13.1 vs. 6.6, Δ = 6.5 (4.5, 8.4), P < 0.001; 2001: 20.5 vs. 10.2, Δ = 10.3 (6.6, 14.0), P < 0.001] (Table 2 and Fig. 1) and had a lower PPT [1989: 185 kPa vs. 232 kPa, Δt = −0.098 (−0.159, −0.036), P = 0.02; 2001: 173 kPa vs. 233 kPa, Δt = −0.130 (−0.207, −0.053), P = 0.01] (Table 2 and Fig. 2) both in 1989 and 2001. Genders were therefore analysed separately in the following.

Total tenderness score in 1989 and 2001 in men and women. Mean values ± SEM. ∗∗∗Significant difference at the 0.001 level.

Pressure pain thresholds in 1989 and 2001 in men and women. Mean values. ∗∗Significant difference at the 0.01 level. NS, Not significant.
Total tenderness score and pressure pain threshold according to gender
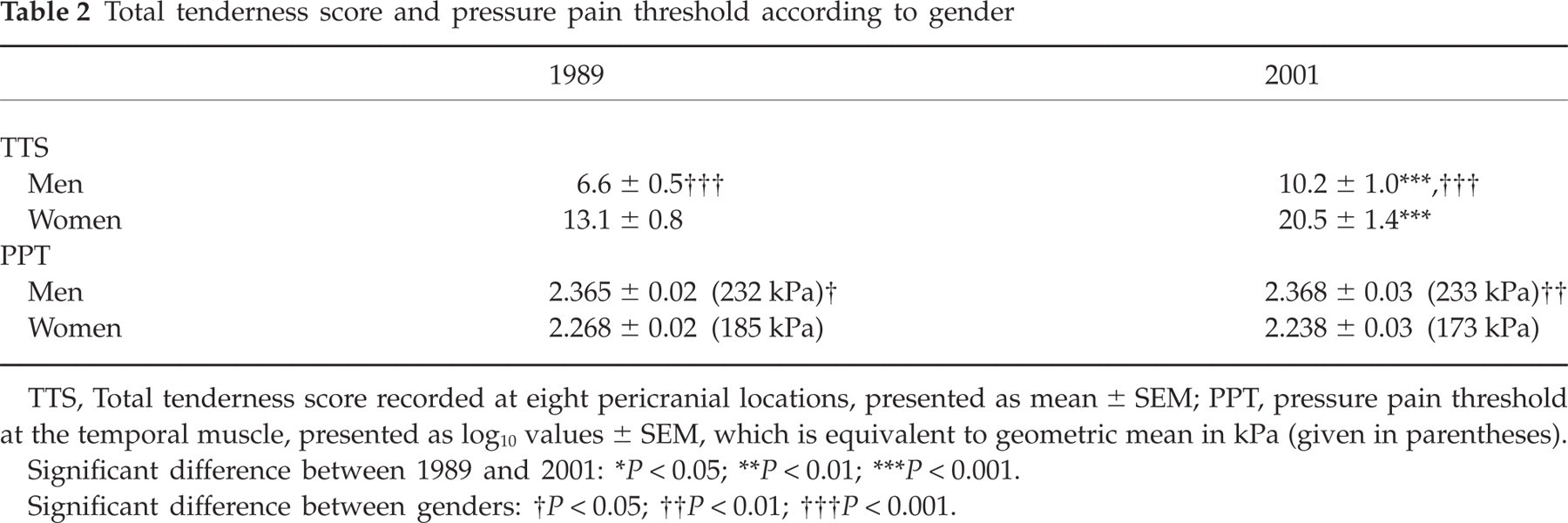
TTS, Total tenderness score recorded at eight pericranial locations, presented as mean ± SEM; PPT, pressure pain threshold at the temporal muscle, presented as log10 values ± SEM, which is equivalent to geometric mean in kPa (given in parentheses).
Significant difference between 1989 and 2001:
P < 0.05;
P < 0.01;
P < 0.001.
Significant difference between genders:
P < 0.05;
P < 0.01;
P < 0.001.
TTS
Subjects with TTH were significantly more tender than subjects without headache both in 1989 [men: 10.5 vs. 5.7, Δ = 4.8 (1.2, 8.4), P = 0.01; women: 15.6 vs. 10.7, Δ = 4.9 (1.1, 8.8), P = 0.01] and in 2001 [men: 14.6 vs. 8.4, Δ = 6.2 (0.7, 11.7), P = 0.03; women: 27.6 vs. 12.8, Δ = 14.8 (9.4, 20.2), P < 0.001] (Table 3 and Fig. 3).
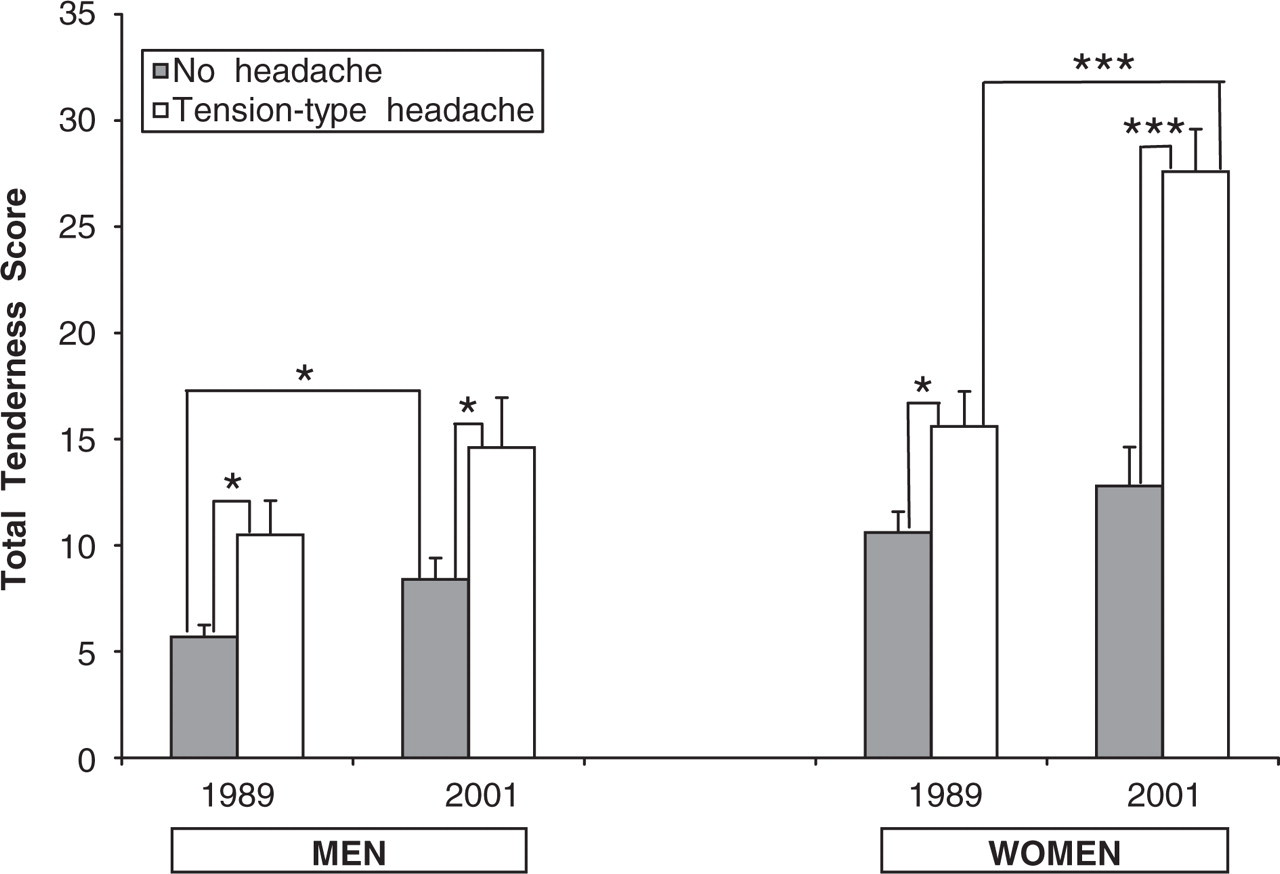
Total tenderness score in 1989 and 2001 according to headache profile. Mean values ± SEM. ∗Significant difference at the 0.05 level; ∗∗significant difference at the 0.01 level; ∗∗∗significant difference at the 0.001 level.
Total tenderness score and pressure pain threshold according to headache

TTS, Total tenderness score recorded at eight pericranial locations, presented as mean ± SEM; PPT, pressure pain threshold at the temporal muscle, presented as log10 values ± SEM, which is equivalent to geometric mean in kPa (given in parentheses).
Significant difference between 1989 and 2001:
P < 0.05;
P < 0.01;
P < 0.001.
Significant difference between TTH and no headache:
P < 0.05;
P < 0.01;
P < 0.001.
Tenderness was significantly higher in 2001 compared with 1989 both among men [10.2 vs. 6.6, Δ = 3.6 (1.3, 5.8), P = 0.001] and among women [20.5 vs. 13.1, Δ = 7.4 (4.2, 10.7), P < 0.001] (Table 2 and Fig. 1). When stratified according to the presence of TTH (Table 3 and Fig. 3), the tenderness increased in all groups but only significantly so in men without headache [8.4 vs. 5.7, Δ = 2.7 (0.5, 5.1), P = 0.02] and in women with TTH (27.6 vs. 15.6, Δ = 12.0 (6.8, 17.1), P < 0.001].
PPT
In 2001, women with TTH had a significantly lower PPT compared with women without headache [144 kPa vs. 205 kPa, Δt = −0.154 (−0.265, −0.043), P < 0.01] (Table 3 and Fig. 4). Elsewhere, nodifferences in PPT between subjects with and without TTH were found either in 1989 or in 2001.

Pressure pain thresholds in 1989 and 2001 according to headache profile. Mean values. ∗Significant difference at the 0.05 level; ∗∗significant difference at the 0.01 level; ∗∗∗significant difference at the 0.001 level.
No changes in PPT from 1989 to 2001 were found (men: 232 kPa vs. 233 kPa, P = 0.95; women: 185 kPa vs. 173 kPa, P = 0.34) (Table 2 and Fig. 2). However, when stratified according to the presence of TTH, PPT was significantly lower in 2001 compared with 1989 in women with TTH [144 kPa vs. 179 kPa, Δt = −0.096 (−0.190, −0.002), P = 0.046] (Table 3 and Fig. 4).
Tenderness score for each palpated location
The trapezius muscle, neck insertions and the lateral pterygoid muscle were all highly tender both in 1989 and in 2001. Tenderness increased in all three muscles over the period, significantly so in the trapezius muscle (P < 0.001) and in the neck insertions (P < 0.001).
Discussion
The major finding of this study was that the increase in prevalence and frequency of TTH among the young general population in Denmark over a 12-year period (7) was related to a significant increase in tenderness of pericranial myofascial tissues. When stratified according to the presence of TTH, the increase in tenderness was clinically and statistically significant only in women with frequent headache.
The most prominent abnormal finding in patients with TTH is a high degree of tenderness in pericranial muscles (6, 11, 15), which is positively correlated to intensity and frequency of headache (6, 16). Thus, the present finding of an overall increase in tenderness in the study population is in perfect agreement with the results of previous cross-sectional studies mentioned above. Determining changes over time requires comparable study designs and methodology in order to compare results reliably. A major strength of this study was the use of the nationwide Danish Civil Registration System, enabling the sampling of a representative cohort in 2001 comparable to the 1989 cohort. Other important strengths were the exact replication of design, the blinding of the observer with regard to tenderness and pain thresholds, and that all headache diagnoses were conducted by medical doctors both in 1989 and in 2001. The degree of tenderness elicited by palpation is, however, dependent of the pressure intensity exerted by the observer, and considerable variation in palpation pressures between observers has been reported (12, 13). Training the observer with a palpometer to exert a standardized palpation pressure can reduce the interobserver variation (12, 13), but unfortunately the palpometer was not yet available in 1989. Potential observer variation in the evaluation of TTS can therefore not be ruled out. Stratification according to the presence or absence of TTH showed, however, a much higher increase in tenderness over the 12-year period among subjects with TTH compared with subjects without headache, especially in women, where the increase was both clinically and statistically significant. The increase in tenderness among subjects with TTH is in agreement with a higher frequency of TTH in 2001 than in 1989. The TTS variation between groups partly contradicts that the increase in TTS is caused only by observer bias. Men without headache constitute a large part of the study population, thus the modest but significant increase in tenderness in this group presumably reflects the overall increase in the total study population.
It is not known for certain whether the increased tenderness is a primary or secondary phenomenon of the headache. It may be caused partially by sensitization of peripheral nociceptors in myofascial tissues. However, firm evidence for peripheral abnormalities is still lacking and it has become clear that central factors, in particular central sensitization, may also play an important role. Based on the available data on patients with TTH, it has been hypothesized that frequent nociceptive input from muscles in the cephalic region of patients with ETTH induces sensitization of sensory afferents and second-order neurons in the trigeminal nucleus caudalis and dorsal horn of the cervical spinal cord. If this process is not blocked, the neuronal plastic changes may spread to supraspinal structures and result in sensitization of third-order neurons in the thalamus and neurons in the somatosensory cortex and lead to CTTH and generalized hyperalgesia (3, 4, 17). This hypothesis is further supported in a recent study demonstrating a decrease in grey matter brain structures involved in pain processing in patients with CTTH (18). The decrease was positively correlated with duration of headache and the authors interpreted the data as being the consequence of central sensitization generated by prolonged input from pericranial structures.
The hypothesis is also in agreement with the consistent findings of increased pericranial tenderness in both ETTH and CTTH (6, 11, 15), but decreased pain thresholds only in CTTH patients (15, 19–21), due to CNS sensitization, and not in ETTH patients (6, 22), where CNS sensitization is not yet (or only partly) established.
According to the suggested hypothesis, increased tenderness is a risk factor for developing TTH rather than a consequence of the disease. One may therefore fear that the overall increase in tenderness in the population will lead in future to an even higher prevalence, not only of TTH but also of other myofascial pain conditions (e.g. fibromyalagi, local pain syndrome and low back pain). This suggests a public health problem and emphasizes the need for prevention strategies to reduce tenderness in the general population. Prevention strategies must focus on individual, work-related as well as societal factors. Among work-related factors, physical work with a heavy load, the strain of work and awkward work postures have been described as contributing to musculoskeletal pain (23, 24). The universal use of computers in 2001 in contrast to 1989 may also be of importance.
As mentioned, decreased pain threshold is seen only in subjects with CTTH, whereas subjects with ETTH have a normal pain threshold. Subjects with CTTH constitute only a minor proportion of the population and it was therefore expected that no overall change in PPT in the population over the 12-year period was found. Stratified according to presence or absence of TTH, the pain threshold was significantly lower in 2001 compared with 1989 in women with TTH. This is in agreement with the significantly higher prevalence of CTTH among women with TTH in 2001 compared with 1989.
In 2001, women with TTH had a significantly lower PPT than women without headache. Thiscan again be explained by the high prevalence of CTTH among women with TTH in 2001. Previously, decreased pain threshold has been documented only in clinical studies including a relatively large number of subjects (16) and, to our knowledge, this is the first time decreased pain threshold in subjects with frequent TTH has been documented in the general population.
One can argue against the differential participation rate in 1989 compared with 2001. The lower participation rate in 2001 may be explained by a general tendency in the young population towards a declining willingness to spare time for participation (25, 26). However, no difference was detected in headache profile between subjects who completed only the headache interview and participants in the 2001 study, and it is therefore unlikely that the lower participation rate in 2001 has induced major selection bias.
In conclusion, our study has demonstrated that the increase in prevalence and frequency of TTH in the young general population in Denmark over a 12-year period was related to an overall marked increase in tenderness and in a decrease in pressure pain thresholds in women with frequent TTH in contrast to subjects without headache. The overall increase in tenderness in the population may predict an even higher prevalence of TTH in the future. The present changes in tenderness and pressure pain thresholds support the hypothesis of sensitization in CTTH based on data from smaller clinical studies. The findings emphasize the major need for prevention strategies to reduce tenderness and TTH in the general population.
Conflict of interest
None declared.
Acknowledgements
We thank Mrs Mette Sadolin (MS) and Mrs Vibeke Thomsen (VT) for skilfully conducting the clinical examinations. The study was supported by grants from The East Denmark Health Science Research Forum, The Danish Medical Association Research Fund, The Danish Health Insurance Foundation, The Danish Hospital Foundation for Medical Research, The Danish Headache Society, The Cool Sorption Foundation, GlaxoSmithKline A/S, Merck Sharp Dohme A/S, Pfizer A/S, Lundbeck Pharma A/S and H. Lundbeck A/S. The funding sources have not been involved in the conduct of the study.