
Abstract
The Headache and Pain Clinic (HPC) is a unit of the Zürich Neurology Department, established in 1966. In the present study demographic features, clinical characteristics and medical management of primary and tertiary care patients were compared in two groups of 181 patients each, seen by general practitioners (GPs) or the HPC, respectively, for primary headaches in 1998. There was a preponderance of women and the socially underprivileged in both samples. Chronic headache was overrepresented in the HPC (44.7%). Loss of work for >2 months was found exclusively in the HPC (9.9%). Of the GP patients, 40% were using triptans and 26.5% in the HPC. One-third of both groups had had complementary and alternative medical treatment. Differences in management strategies reflected differences in headache severity and chronicity. Results indicated that remaining shortcomings of diagnosis and treatment of headache in primary care could be minimized by involving GPs in similar non-commercial studies.
Keywords
Introduction
The Headache and Pain Clinic (Kopfwehsprechstunde, HPC) in the Neurology Department, Zürich University Hospital, is a service for the assessment and management of difficult headache problems. Demographic, nosological and therapeutic characteristics of 1625 out-patients were presented and discussed in a previous paper (1). When treatment before and after referral was compared, strikingly different patterns emerged. One salient feature was the referring physicians' preference for acute treatment with simple or combined analgesics. These findings permitted some first insights into the state of information of referring physicians. To give a more precise picture of the characteristics of headache patients in primary care we were interested in patients of general physicians who had not been referred to the HPC. In the present study we compare demographic, nosological and therapeutic characteristics of tension-type headache and migraine patients from the HPC with a group of headache patients from general practitioners (GP) in the Zürich region.
Patients and methods
Demographic features, severity of disorders and medical management in general practice and tertiary care were compared in two groups. For the first group 20 randomly selected GPs from the Zürich region were asked to provide anonymized data of the last 10 patients seen for headaches in 1998. We received datasets of 181 patients. For the second group we selected semirandomly (alphabetically by each first letter of the family name and then alphabetically by the following letters of the family name) the same number of patients from the records for 1998 of the Headache and Pain Clinic.
The following patient data were collected in a standard form, or questionnaire, designed for this purpose: sex, age; marital status, children; native language, educational status; occupation; diagnosis; age at onset of headache; frequency of headache (headache days per month); loss of working days per month and per year; other diseases, and drugs taken for them; special investigations: computed tomographic (CT) scan, magnetic resonance imaging (MRI) and EEG; long-term prophylactic drugs for headache; drugs for acute headache (attacks); drugs discontinued because of adverse effects, or lack of effect; alternative, or complementary treatments; special remarks.
Missing data were obtained by telephone interview, using the same form. However it was not possible to reach every patient for this purpose. Some demographic and clinical data remained missing in <5% of patients and were not included in the analysis. In this study no data have been collected about the participating GPs' interest in migraine and their satisfaction with the conclusions and learning generated by the study.
Student's t-test and Spearman's ρ for correlation were used for statistical analysis with SPSS version 11.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
Demography
Women were overrepresented in both samples: GP, 76.8% women to 23.2% men and in the HPC, 67.4% women to 32.6% men. The age ranged from 8 to 86 years in the GP group, with a mean age of 45.5 years, and from 9 to 75 years in the HPC group, with a mean age of 38.6 years. Of the GP patients 6.6% were aged <20 years (HPC 7.2%), 28.2% between 20 and 39 years (HPC 47%), 44.8% were 40–59 years old (HPC 39.2%) and 18.2% (HPC 6.6%) were aged ≥60 years. Of the GP patients, 22.7% were single, 65.2% were married, 5.5% divorced and 6.1% widowed. Of the HPC patients 34.3% were single, 53% married, 8.8% divorced and 2.2% widowed.
Of the GP sample, 28.5% (vs. 27.1% of the HPC group) had only basic education, 58.7% (vs. 62.7%) had attended trade school and 8.9% (vs. 10.2%) had tertiary education; 3.9% in the GP sample had no formal education. In the GP group there were 71.5% native German speakers, the official language of the region of Zurich (HPC 63.5%). Other native languages spoken were Italian, Albanian, Croat, Turkish and Spanish with >3%, and several others with <3% in both groups (French, Portuguese, Greek and English).
Clinical characteristics
According to the International Headache Society (IHS) criteria (2), GPs diagnosed migraine (M) in 60.2%, tension-type headache (TTH) in 21.5% and in 18.2% both combined (M + TTH). In the HPC 49.7% of the headaches were classified as M, 18.8% as TTH and 31.5% as both combined. Among the women in the HPC 52.5% were diagnosed as M, 13.9% TTH and 33.6% as both combined; men HPC: M, 44.1%; TTH, 28.8%; M + TTH, 27.1%. GPs: women 63.3%, 18.0%, 18.7%, respectively; men 50.0%, 33.3%, 16.7%, respectively. One-third of the GP patients had a positive family history of primary headaches.
The mean age of onset of 25.5 years in the GP group was 3.5 years higher than that in the clinic group. Separated into the three groups of diagnoses the mean age of onset in the GP sample was 24.2 years for M, 30.3 years for TTH and 23.1 for both combined. In the HPC it was 19.6 years for M, 30.6 years for TTH and 20.9 years for both combined (Table 1).
Demographic data of headache subtypes in primary [general practitioner (GP)] and tertiary care [Headache and Pain Clinic (HPC)]

M, Migraine; TTH, tension-type headache.
A subanalysis of the 90 migraine patients of the HPC showed a significant correlation between disease duration and frequency of headaches per month, as well as age of onset and frequency of migraine (Fig. 1). This would support the hypothesis derived from clinical experience in the HPC that onset at younger age and longer history of headache was a predictor of more severe impact at the time of observation (1).

Subanalysis of the 90 migraine patients of the Headache and Pain Clinic. (a) Duration of disease correlates with headache frequency (c = 0.25, P < 0.02). (b) Correlation of onset and frequency of headaches (c =−2.61, P = 0.019).
On average, migraine patients had a lower frequency of headache days per month than TTH patients (Table 1). In the GP sample, 18 (10.0%) patients suffered from chronic daily headache (CDH) (≥15 headache days per month (3)), with either chronic migraine (cM) or chronic tension-type headache (cTTH) as diagnosis (4). In the HPC, 81 (44.8%) patients suffered from CDH, 55 of them had headache every single day (nine patients M, 25 TTH and 22 M +TTH) (see Table 2 and Fig. 2).

Frequency of headaches in primary (GP, □) and tertiary care (Headache and Pain Clinic, ▪).
Incidence of migraine (M), tension type headache (TTH) and both combined (M and TTH) in primary (GP) and tertiary care [Headache and Pain Clinic (HPC)]

Impact: loss of school or work days
In the GP group 75.1% reported no loss of working or school days, and no one lost more than 60 work days per year. In the HPC group 64.6% reported no loss, 25.4% reported up to 60 days and 9.9% had loss of work from >60 up to 365 days.
Special investigations
The most frequent special investigations were: CT scan (16% in GP, 19.9% in HPC before and 11.6% after admission), EEG (15.5% in GP, 12.2% in HPC before and 2.2% after admission) and MRI (4.4% in GP, 6.6% in HPC before and 6.1% after admission). In both groups no pathology was found which would have led to further investigations or interventions.
Treatment
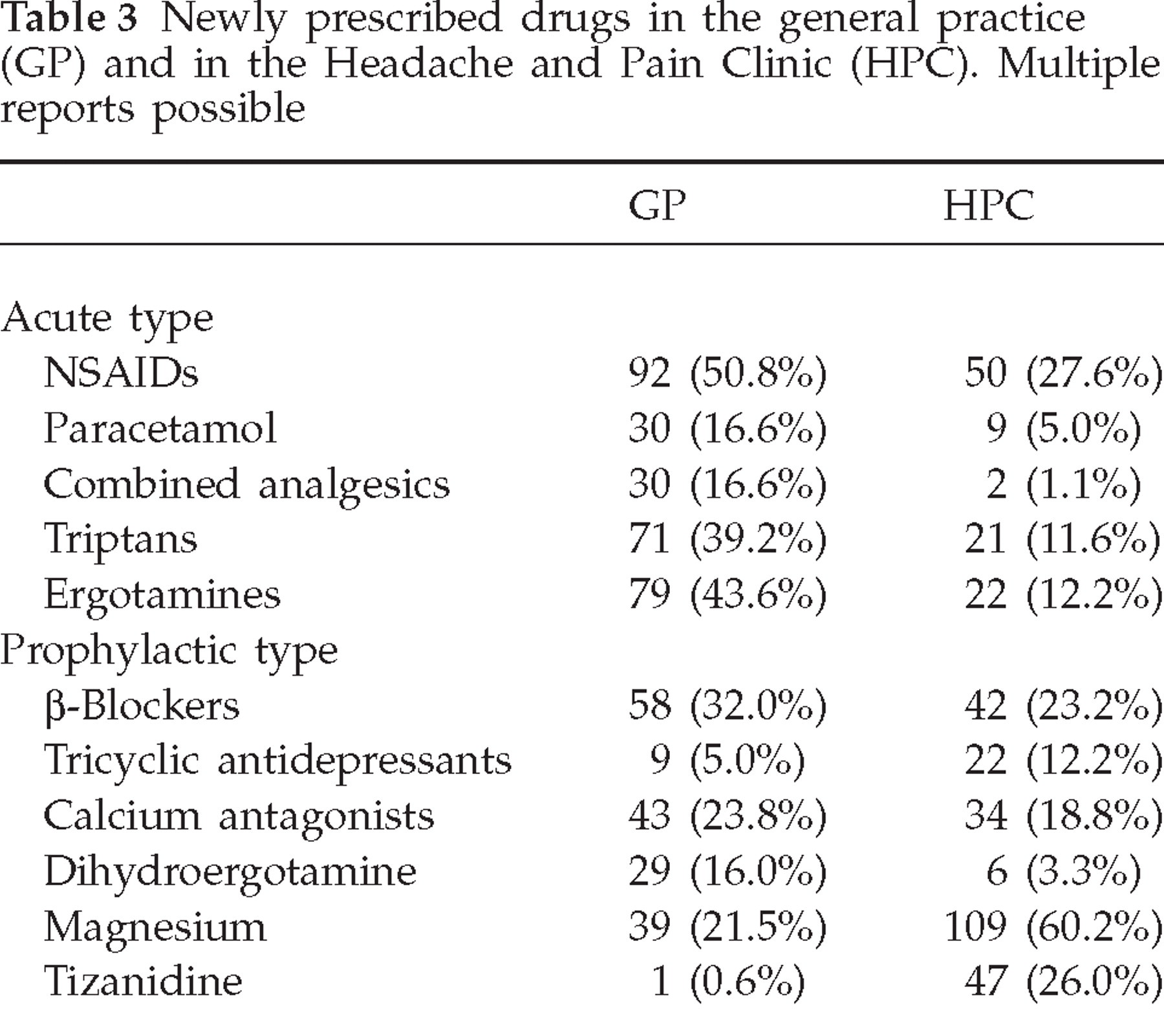
In the GP sample, 89.5% were using treatment for attacks and 59.7% were currently on prophylactics or had tried them in the past. In the HPC 90.6% had some instant relief type drug and 67.4% were on a preventive drug. Table 3 gives an overview of newly prescribed drugs in the two samples. The specialists newly prescribed triptans in 11.6%; the total of patients using triptans in the HPC was 26.5%, whereas 39.2% of the GP patients were using triptans. Only nine patients in both samples had never tried any medication for their headaches.
Newly prescribed drugs in the general practice (GP) and in the Headache and Pain Clinic (HPC). Multiple reports possible
In the GP sample there were 62 patients (34.3%) who reported other than drug treatment, seven of whom had tried additional physiotherapy, autogenous training or hypnosis. In the HPC, 109 patients (60.2%) reported additional therapy, 53 of whom had tried one of the three above. Forty-seven GP patients (26.0%) and 56 (30.9%) HPC patients had used the following complementary and alternative medicine (CAM): acupuncture, aromatherapy, Atlaslogy, Bach flowers, bio-resonance, china oil, chiropractic, colour therapy, craniosacral therapy, electrotherapy, foot reflex massage, homeopathy, laser treatment, lymph drainage, magnetopathy, morphology, neural therapy, neurolinguistics, osteopathy, phytotherapy, psychophonie, Reiki, Shiatsu, vitalogy, yoga. The most frequently reported CAM treatments were acupuncture and homeopathy.
Discussion
Demographic characteristics
The distribution of demographic characteristics in both samples was typical of treatment samples. There was a preponderance of women of nearly 3 : 1, the ratio usually found in migraine patients (5). Similar to a study of tertiary care patients in a Hungarian headache clinic (6), only 6.6% of the HPC patients were >60 years and almost half of them were in their most productive years (between 20 and 40 years old). In the GP sample the patients were older, nearly one-fifth being >60 years old, and only 28.2% were in their 20s and 30s. This may reflect more pressure from working life in the tertiary care patients vs. a quest for better quality of life in the GP patients, and also the lifetime course of migraine, which tends to become less severe in the later years of life.
The marital status of the patients presented no important differences from the distribution in the general population of Switzerland in 1998 (7), where 42% were single, 46.6% married, 5.5% divorced and 5.9% widowed.
The educational characteristics showed no differences between the two samples, apart from a group of patients without education, which appeared only in the GP sample. Compared with the Swiss population, higher learning was rare, slightly below the level of females in the general population (7). This appears to contradict the popular illusion of migraine as a disease of intellectuals (8), if it is not simply a result of the socioeconomic downward drift caused by the impact of the headache syndromes. The latter possibility was not systematically researched. More than one-third of the HPC patients and more than one-quarter of GP patients were native speakers of languages other than German, the official tongue of the region of Zürich (general population of the region of Zürich: 20.9% (9)). Again, the socially underprivileged appear to be overrepresented in both samples, but more so in the HPC, where the impact of headache was more severe, especially in the most productive age groups.
Clinical characteristics and impact
In our Swiss headache clinic there were 44.7% with CDH. This is in line with the number of patients with CDH in other headache clinics (10). The most common diagnosis of 638 CDH patients visiting a US headache clinic was chronic migraine (87.4%), two-thirds of them associated with medication overuse (11). Bahra et al. have reported that medication overuse headache would occur more often in patients with migraine (12). We had not collected data to distinguish primary chronic headache reliably from medication overuse headache, but unlike the studies above, we found more cTTH than cM in our Swiss headache clinic. These differences point to characteristics probably related to coping and self-management strategies.
In a Norwegian study, 195 headache patients were examined by GPs and neurologists and their diagnoses have been compared (13). The GPs diagnosed migraine in 116 cases, the neurologists in 144 cases. In only 104 cases (53.3%) did their diagnoses agree. The GPs in this sample made more correct diagnoses compared with the referring doctors of our recent study of 1625 consecutive HPC patients (1), where many patients' headaches were merely classified as ‘headache’. Is it too easy – and therefore not challenging – for general physicians to diagnose correctly and manage primary headaches, or is it too difficult? The pressure of cost-effectiveness on the duration of consultations usually prohibits adequate management of patients with severe and chronic headaches in general practice. A recent study of 180 consecutive patients attending a specialty clinic in the UK concluded that the burden of headache, represented by the number of headache days per month, was the driving force for patients to seek help from a specialist. Patients with migraine and chronic headache reached the highest scores in tests for psychopathological and general social impairment (14).
The combination of migraine with TTH was less often diagnosed in the GP sample than in the headache clinic. This can be ascribed to the following reasons: the GPs' preference of dealing with the more troublesome complaint, or, alternatively, the specialists' more detailed background from experience, study results and discussions on diagnoses and treatment indications, including the usually neglected treatment recommendations of the national headache societies. Furthermore, most physicians in Switzerland use one simple code in their invoices for all headache syndromes, with only one qualifier for chronic or recurrent forms, a very good reason for them not to bother with specific diagnoses or treatment indications. There is a widespread illusion about the ability of GPs to apply complicated codes to their diagnoses. It is obvious that the IHS classifications of 1988 and 2004 (2, 4) prescribe much more detailed coding than can possibly be applied in any clinical practice outside scientific epidemiological and other systematic studies. However, our limited project provided an incentive for the participating GPs to take a closer look at the diagnosis and management of individual headaches.
Treatment
Most referred patients in the specialty clinic were on an attack treatment, therefore only a few analgesics were newly prescribed. The number of triptans in the GP sample was quite high for 1998 (almost 40%). In comparison, only 15% of the HPC patients were using a triptan before they have been referred to the clinic (1). This difference could be partly explained by the ongoing proliferation of triptans with concomitant intensification of their marketing during the time of our observation. With regard to preventive drugs, there was not much difference between the GP and the HPC, but the classes of drugs were quite different. Where GPs prescribed mainly the older, well-known drugs (propranolol and flunarizine), the specialists from the HPC used newer drugs with better tolerability profile (nadolol and cyclandelat). The GPs prescribed ergotamine derivates as prophylactics in 16% of the patients. This is a high proportion in view of the possible complications of vascular problems and medication overuse headache (15, 16). The high percentage of patients on magnesium (67%) in the HPC sample, and the seven patients on riboflavin and seven on anticonvulsants only in the HPC, may be explained by newly emerging strategies which found their way into headache management by studies published more recently and abstracts presented at international conferences (17, 18). Tizanidine was also used only in the HPC in 1998, in chronic headache with sleep disorder. Belatedly, a study from 2001 (19) has shown its effect in chronic daily headache. One-third of the HPC patients were treated with a selective serotonin reuptake inhibitor, mainly for comorbid depressive illness.
The number of special investigations seems excessive in relation to the relatively minor severity of the headache problems in the GP sample. This reflects an important feeling of insecurity of both the patient and the GP, driving them to seek help from the system. The frequent use of EEGs indicates a common information deficit of GPs and their neurologists. Less than 5% of all headaches are of a secondary nature (5), excluding headaches associated with systemic infection. They are usually identified by thorough interview and neurological examination, leading to strictly indicated further investigations.
One salient feature is the high amount of non-drug treatment. Surprisingly in tertiary care, in a mainstream medical context, more procedures without drugs (two-thirds) are used than in general practice (one-third). However, half of the non-drug treatments in the HPC were therapies which had found their way into mainstream medicine in recent years (20). The effects of these types of treatment should be assessed in future controlled studies (21).
Conclusion
Most results only confirm the expected difference in impairment due to headache between patients seen by GPs and those attending a headache clinic. The correlation between duration and frequency of migraine was unexpected and may be understood as an argument for early systematic prophylaxis. The relationship of early onset to more frequent and disabling migraines would even be an argument for prevention from childhood or adolescence onwards.
There is still a great need for better information and education of primary care providers in the diagnosis and treatment of headache. However, the GPs in our study made more correct diagnoses and prescribed more specific migraine medication than the referring GPs of the headache and pain clinic (1). We are reminded of Heisenberg's uncertainty principle. The observation itself appears to change the observed subject. The participating GPs belonged to the same primary care community as the GPs who referred patients to the HPC, but they appeared to change their attitude to the diagnosis and management of migraine.
There were no formal questions about the motivation of physicians to take part in this project, but they appear not to have had serious misgivings about exposing their methods to scrutiny. On the other hand, the project did attract their attention to a large group of their own patients not usually subject to detailed investigation. This focusing of their attention must have encouraged a closer look at their own management of those cases. We conclude that differences in headache appraisal and management between primary and tertiary care may be minimized by the simple expedient of involving GPs in similar non-commercial studies where they will take care to appear updated. This method may be more efficient in advancing the know-how of GPs than traditional continuing medical education (CME) programmes, update exercises, public relations campaigns and sales promotion drives.
Our opinion is that patients with primary headaches would best be served if GPs diagnosed and treated them according to the methods of HPC specialists. It may be true that the newest preventives may not work better than their older counterparts but this can be determined only by using both kinds in the appropriate order, namely, using the more expensive newer preventive drugs after the others have failed. This procedure works for HPC specialists, but it will also work for the GP if both groups of physicians work closely together.