
Abstract
The aim of this study was to compare acupuncture, relaxation training and physical training in the treatment of chronic tension-type headache (CTTH). The study comprised 90 consecutive patients with CTTH who were randomly allocated to acupuncture, relaxation training or physical training. Headache intensity, headache-free days and headache-free periods were registered using a visual analogue scale and a headache diary. The measurements were made 4 weeks before, immediately after, and 3 and 6 months after the treatment period. Immediately after the last treatment, the number of headache-free periods and of headache-free days was higher in the relaxation group compared with the acupuncture group. There were no other significant differences between the groups at any time point. The clinical implications of our findings are that relaxation training induced the most pronounced effects directly after the treatment period, compared with acupuncture and physical training.
Introduction
The International Headache Society (IHS) introduced the classification ‘tension-type headache’ (TTH) in 1988 (1) and a revised version in 2004 (2). IHS subclassifies the diagnosis TTH into an episodic and a chronic form (1, 2). For a TTH to be classified as episodic (ETTH), it must have occurred at least 10 times, but for not more than 15 days (1, 2). To be classified as a chronic TTH (CTTH), the headache must occur at least 15 days per month for at least 6 months (1, 2). To be diagnosed as ETTH or CTTH, the headache must fulfil additional diagnostic criteria and have other defining characteristics according to the IHS classification (1, 2). These characteristics pertain to pain, muscle tenderness, physical activity, nausea, photophobia and a history of physical and neurological examinations (1, 2).
ETTH and CTTH are also subclassified according to whether or not the headache is associated with pericranial tenderness (1, 2). Patients who suffer from migraine can often have TTH and patients who suffer from TTH sometimes also experience episodes of migraine-like headache (2, 3). A migraine will sometimes gradually transform into a CTTH, but more frequently it is the ETTH that evolves into a CTTH (2, 4).
The origin of TTH is multifactorial (5, 6). The pathogenesis of TTH is unclear, and most investigators seem to agree that several different pathophysiological factors influence TTH (5–7). Muscular factors are considered to be very important (6, 8). A common symptom in patients with TTH is increased tenderness of pericranial myofascial tissue (9, 10). It has been suggested that CTTH is not directly linked to muscle contractions but thattenderness is closely related to greater general pain sensitivity (5, 8–10).
One predominant theory in CTTH is that sustained nociceptive input from the pericranial myofascial tissue increases the excitability of the central nervous system (4) by sensitizing it (4, 8, 10). Sustained pericranial myofascial nociception may be responsible for the transformation of ETTH into CTTH (4). Investigators believe that the higher sensitivity of the nociceptive pathways may be important in the pathophysiology of CTTH (11).
Pharmacological treatment of TTH includes muscle relaxants and antidepressants, as well as analgesics (12). Several studies have documented the positive effects of ibuprofen on TTH (13, 14). Pharmacological treatment with amitriptyline has also been found to be effective in patients with chronic daily headache (15). CTTH was not found to improve significantly following treatment with botulinum toxin (16), but the role of botulinum toxin has not yet been fully defined (17). Amitriptyline seems therefore to be the drug that best prevents chronic daily headache at this time (15, 17).
The efficiency of paracetamol in CTTH has still not been proven. Many patients with headache tend to increase their consumption of analgesics, and this can increase headache frequency (2, 12, 18, 19). When the episodic form of TTH becomes chronic, the overuse of drugs frequently plays a role in aggravating the ETTH disorder (2). Paradoxically, the use of medication decreases if the headache becomes chronic (20). It is important to reduce analgesic consumption as a first step in the treatment of TTH (7, 14, 15).
There are few controlled studies of non-pharmacological treatment for patients with CTTH. Non-pharmacological treatments in patients with CTTH might decrease the excitability and sensitization of the central nervous system, thereby decreasing general pain sensitivity, as theorized above (4, 8, 10). Relaxation training and acupuncture have been evaluated in controlled studies (21–24). The relaxation techniques most widely used in the treatment of patients with TTH are progressive relaxation training (25) and autogenic relaxation training (26). In previous studies, relaxation training has been found to improve TTH significantly (23, 24). In a school-based, nurse-administered relaxation training study on TTH, a long-term effect of relaxation training was shown (23). No other controlled studies on CTTH and relaxation training have been found.
There have been many controlled studies of acupuncture treatment in TTH (21, 22, 27–30). It has been found to be both effective (31) and ineffective (21) in reducing headache scores compared with controls. No conclusion can therefore be drawn concerning the effect of acupuncture on CTTH. Other non-pharmacological treatments for the alleviation of TTH include physical training, ergonomic instruction, massage, transcutaneous electrical nerve stimulation and cold or heat treatment, but their effect has so far not been scientifically evaluated.
The aim of the present study was to compare the treatments acupuncture, physical training and relaxation training in patients with CTTH regarding headache intensity, headache-free days and headache-free periods with a follow-up period of 6 months after the last treatment.
Methods
Patients
Of the 90 patients with CTTH, 17 were men and 73 women, aged 18–65 years. All had been examined and referred for physiotherapy treatment by their physicians at three primary care units in the city of Göteborg and its suburbs from March 1997 to September 1999. The patients were also examined a second time by one of the authors (E.S., a registered physiotherapist) at their respective primary care units to confirm the diagnosis before randomization of the patients to the treatment groups.
The inclusion and exclusion criteria were established according to guidelines for trials of drug treatments in TTH (12). Inclusion criteria were age between 18 and 65 years and a diagnosis of CTTH as defined by the IHS, at least 15 days for at least 6 months (1).
Exclusion criteria were as follows: headache that began after the age of 50 years, migraine more than once a month during the last year, inability to speak or read Swedish, serious somatic or psychiatric disease, or drug abuse or use of analgesics and triptans >10 days per month (12).
The patients received written information about the study. After agreeing to participate, patients signed the informed consent. Ninety patients were randomized, using sealed envelopes, into one of three different treatment groups: an acupuncture group (n = 30), a physical training group (n = 30) or a relaxation training group (n = 30). The study comprised a pretreatment period of 4 weeks, a treatment period of 2.5–3 months and a post-treatment period of 7 months. The Ethics Committee of Göteborg University approved the study.
Assessments
One of the authors (E.S.) made all assessments but did not perform any treatment. Outcome measures were headache intensity, headache-free days and headache-free periods. Headache intensity was measured using a visual analogue scale (VAS), which consists of a 100-mm straight line with ‘no pain’ as the left end-point and ‘worst possible pain’ as the right end-point (32). The patients marked their actual pain intensity on the line.
The patients were asked to keep headache dairies for 4 weeks before treatment and again 4 weeks immediately after treatment. Beginning 3 months and 6 months after the last treatment session, the patients were again asked to keep a headache diary for 4 weeks. Each diary contained one VAS per page, four pages per day, so that the patients could make four ratings of pain intensity per day and be as little influenced as possible by their previous rating.
Headache-free days per week (range 0–7) and headache-free periods per week (range 0–28) were calculated for each group.
Treatments
Seven registered physiotherapists treated the patients at their usual primary care units (three different clinics). All therapists had documented education at a comparable level for all treatments.
In the acupuncture group, acupuncture was given mainly by five registered physiotherapists at the three different clinics. They used the same technique and all had long experience in treating patients with acupuncture. Disposable needles (Huanchou, Medema, Stockholm, Sweden) with a dimension of 15 × 0.25 mm and 30 or 40 × 0.30 mm were used. The needle length was dependent on the location of the acupuncture point. The needles were inserted to a depth of 2–5 mm or 10–30 mm, depending on location. The needles were twilled by hand, until the patient felt the characteristic needling sensation, the so-called ‘de qi’ sensation, of soreness, numbness or distension, three times during each 30-min treatment. The recommended (33) and clinically most used acupuncture points for CTTH were chosen for the area of the pain, segmental points, in total 10–12 needles, of which not more than eight were distal, peripheral needles in the hands and legs (33). Mandatory points to be needled were GB 20, GB 14, LI 4 and ST 44; optional points were PC 6, PC 7, SP 6, GB 34, ST 8, EX 2 and EX 1 (30). Treatment comprised 10–12 sessions during a period of 10–12 weeks. Twenty-nine patients underwent 12 treatments and one patient underwent 10 treatments.
In the physical training group, training was performed by five, mainly four, registered physiotherapists working at three different clinics. The therapists had long experience and documented education of treating patients with physical training. Treatment lasted 2.5–3 months and included 10 training sessions at the clinic and an additional home training programme. The training consisted of the same exercises for all patients, but the weights were individually adapted.
The patients performed either two 45-min training sessions a week at the clinic for 5 weeks and then a home-training programme three times a week for 5 weeks (a total of 25 training sessions) or one training session at the clinic and a home training programme once or twice a week for 10 weeks (a total of 25 training sessions). The physical training at the clinic was performed according to the principles of Medical Training Therapy (MTT) (34), which include achieving 80% of maximum fatigue. Both the performance and the amount of exercise were the same for all patients.
Each training session consisted of five exercises repeated 35 times and three sets of each (105 times). The patient rested for 1–2 min between each exercise. The exercises focused on the neck and shoulder muscles. Each session began with 5–10 min of ergometric bicycling. The training took place in a group of a maximum of five patients. At least eight of 10 training sessions were carried out under the supervision of a physiotherapist.
The home exercise programme also focused on the neck and shoulder muscles. It consisted of five exercises repeated 10 times and three sets of each (30 times). The patient rested 1–2 min between each exercise. Each session began with two warm-up exercises and ended with one stretching exercise.
In the relaxation group, relaxation was performed mainly by three registered physiotherapists working in three different clinics. The physiotherapists each had long experience and documented skills for treating patients with relaxation training. The relaxation training programme described by Larsson and Daleflod and based on progressive and autogenic relaxation techniques was used (25, 26). Progressive relaxation training by Jacobson is a neuromuscular technique in which different muscle groups are systematically tensed and relaxed (25). Autogenic relaxation training by Schultz is a form of self-hypnotic training where the patient is taught a method to control the body's physiological reactions by repeating selective sentences (26). Besides progressive (25) and autogenic relaxation training (26), the relaxation group practised relaxation and breathing techniques, stress coping techniques, how to relax during activity and how to relax in everyday living. Eight to 10 sessions of relaxation training were performed individually under the supervision of a physiotherapist once a week. Twenty-nine patients performed 10 sessions and one patient performed eight sessions. The patients also received an audiotape for home practice. The audiotape included the last training session and the patients were instructed to train once daily. After the last session the patients received a tape that included all eight to 10 training sessions and instructions to continue training once a day.
The patients performed the training in a comfortable, recumbent position on their back; sitting in chairs; or standing or walking depending on the type of relaxation training. All training took place in a darkened environment.
Statistics
Non-parametric tests were chosen because of the use of the VAS, which is regarded as an ordinal scale with no distinct starting or ending points (32). Within- and between-group analyses were performed on the 90 participants who were randomized for the intention-to-treat (ITT) analysis using a ‘last value carried forward technique’ (assuming no change for non-completers). This technique is a conservative means of applying ITT methodology. In it, the last value recorded before dropping out was carried forward to each missing time period. The assumption was that a patient's score at the time of removal from the study would neither increase nor decrease from that point. When comparing all groups at once, the Kruskal–Wallis test was used. If significant differences between all three groups were found, Fisher's non-parametric permutation test (35) was used to evaluate which groups differed. To evaluate the therapeutic effect of each specific treatment, the time point before intervention was compared with the time immediately after the last treatment. For this comparison over time within groups, Fisher's non-parametric permutation test for matched pairs (35) was used. All tests were two-tailed. A difference of P < 0.05 was considered to be statistically significant.
Results
In the present study the response rate was 100% directly after the last treatment. All patients completed the treatment and the first follow-up directly after treatment with collected diaries.
At the 3-month follow-up, three patients in the acupuncture group, four in the physical training group and four in the relaxation training group did not return their diaries.
At the 6-month follow-up, one patient in the acupuncture group had been in a car accident and was excluded, one refused to continue keeping a diary and 11 patients did not return their diaries. In the physical training group, 11 patients did not send in their diaries. In the relaxation training group, one patient chose to seek other treatment and 10 did not return their diaries (Fig. 1).

Flow chart of the number of diaries kept by the three treatment groups (acupuncture, physical training and relaxation training) during the course of the study.
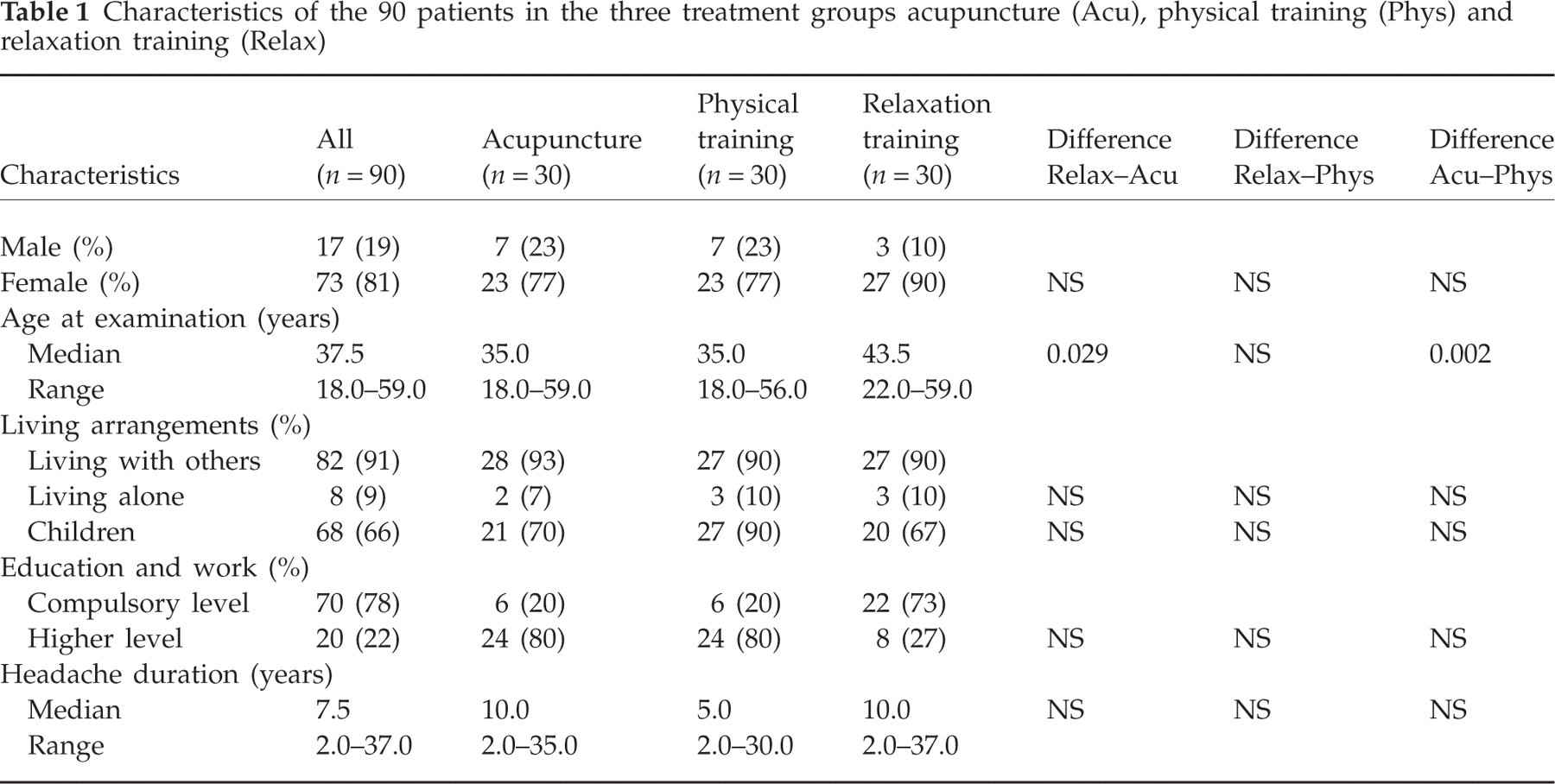
Patient characteristics and social and headache history variables are listed in Table 1. Differences of sex, living arrangements, education, work and headache duration were non-significant between the three treatment groups before treatment (Table 1). The mean age in the relaxation group was significantly higher compared with the acupuncture group (P < 0.05) and the physical training group (P < 0.01).
Characteristics of the 90 patients in the three treatment groups acupuncture (Acu), physical training (Phys) and relaxation training (Relax)
Between-group comparisons
Differences at baseline, after the last treatment and after 3 and 6 months in headache intensity, headache-free periods and headache-free days were compared to investigate whether there were any between-group differences (Table 2). There were no significant differences in headache intensity, headache-free days or headache-free periods between the three treatment groups during baseline ratings 4 weeks prior to the treatment period. The relaxation group reported a significantly higher number of headache-free periods (P < 0.05) and a significantly higher number of headache-free days (P < 0.01) compared with the acupuncture group immediately after the last treatment. There were no other significant group differences between the study groups at any time point.
Differences before and immediately after the treatment period (1–2); differences before and 3 months after the treatment period (1–3), statistically corrected (sc) with ‘last value carried forward’, and differences before and 6 months after the treatment period (1–4) sc with ‘last value carried forward’ in headache intensity, headache-free periods and headache-free days between the groups

Within-group comparisons
In the acupuncture group, headache intensity had decreased significantly both 3 and 6 months after the last treatment compared with baseline (Table 3). Differences in headache-free days and headache-free periods, however, were non-significant in this group. In the physical training group, headache intensity decreased and headache-free days and headache-free periods increased significantly immediately after the last treatment and again at the 6-month follow-up compared with baseline. No significant differences were found at the 3-month follow-up compared with baseline (Table 3). In the relaxation training group, headache intensity decreased and headache-free days and headache-free periods increased immediately after, and 3 and 6 months after the last treatment (Table 3).
Headache variables during 4 weeks before treatment (baseline), period 1; immediately after the last treatment, period 2; 3 months after the last treatment, period 3; and 6 months after the last treatment, period 4. Values are statistically corrected (sc) with ‘last value carried forward’

Discussion
The present study demonstrates that relaxation training and physical training result in a long-lasting reduction in headache intensity, more headache-free days and more headache-free periods in patients with CTTH. Repeated acupuncture treatments resulted in a long-lasting reduction of headache intensity. Patients in the relaxation group had significantly more headache-free periods and more headache-free days directly after the last treatment compared with the acupuncture group. There were no other group differences at the 3- and 6-month follow-ups.
In the relaxation training group, the median age was significantly higher compared with the acupuncture and physical training groups. In addition, there were more women and fewer patients with a high educational level in the relaxation training group, but this difference was not significant.
To obtain a representative picture of a patient's headache problem, it is important that the patient keep a headache diary over a long period and record headache intensity at least once every 24 h (12). In this study we used a simple diary and asked the patient to make four entries every 24 h, so that it would be possible to determine not only headache intensity and headache-free days but also headache-free periods. This would allow us to track the course of the headache throughout the day. The drop-out rate at the follow-ups would perhaps have been lower if we had used a simpler diary, but it would not have allowed us to determine headache-free periods. In the present study, we followed the IHS guidelines for studies of CTTH.
Headache diaries should comprise a baseline of 4 weeks before treatment and an evaluation of 4 weeks after treatment (12). The 4-week registration was repeated again at 3 and 6 months after the last treatment. These data confirmed that the TTH patients in the present study suffered from the chronic form of TTH: they had headache at least 15 days a month.
The main aim of the study was to compare the three non-pharmacological treatments acupuncture, physical training and relaxation training. These are therefore the only results presented in the abstract. Since we had no control group, any report of ‘regression to the mean’ would be a potential bias. Therefore, effects such as participation in a study and recovery that may be a result of the natural course of the illness should be taken into account when considering within-group results. In this study, the patients had an extensive headache history (median 7 years, range 2–37). They also had a pretreatment period of 4 weeks, which should limit the effect of improvement due to the natural course of the illness.
All treatments had a significant, positive, long-lasting effect on different variables and these results are an indication of the importance of evaluating non-pharmacological treatments used in daily clinical practice so that they can be optimized for patients with CTTH.
The statistical analysis used was based on ITT and the technique ‘last value carried forward’ to avoid missing values.
The use of a VAS to measure pain has been documented as a valid measure of perceived pain intensity (30). Each scale was on a separate page of the diary so that patients could not easily compare their measurements. The study was conducted over a period of 3.0 years. The patients were recruited from areas representing the inner city, the suburbs and rural areas around Göteborg. The geographical spread was therefore fairly even and probably did not influence the outcome. The examinations and measurements as well as patient instruction were carried out by the same person and therefore consistent with no interpersonal effects.
Treatment was conducted by a group of physiotherapists. They had received detailed information about the treatment procedure well in advance of the first patient. They were constantly interviewed by the main author about their progress and experience in performing the treatment to ensure consistency over time. The treatment modes were designed to mimic everyday physiotherapist treatments. Hence, several units and physiotherapists were involved in the study. No difficulties were reported related to treatment design. The use of these treatments in clinical practice therefore seems realistic. All patients completed the treatment during the study.
Participation in this study and the attention from the physiotherapists may have affected compliance favourably.
Acupuncture treatment for relief of various types of headache has previously been evaluated in a number of studies. A recent study by Vickers et al. (22) has shown that repeated acupuncture treatment results in a long-lasting reduction in headache scores measured on a Likert scale (22) in patients with chronic headache (22). It should be noted that both patients with migraine and patients with TTH were included in the study. In studies evaluating the effect of acupuncture by Karst et al. (21) and Karakurum et al. (29), headache intensity decreased, but not significantly compared with sham stimulation (21, 22, 29). One might conclude that the effect of acupuncture in the treatment of TTH is weak.
In accordance with previous studies, we found that relaxation training significantly improved TTH (23, 24) concerning headache frequency and the number of headache-free days. In a school-based, nurse-administered relaxation training intervention in TTH, a remaining effect at the 6-month follow-up was noted (23). One plausible explanation might be that the patients learn to control their headache by themselves. They are taught to use recommended techniques and strategies and can perform relaxation training at home.
To the best of our knowledge, this is the first study on patients with CTTH in which the effect of physical training has been compared with other treatment strategies. It demonstrates a long-lasting positive effect of moderate physical training. The patients were instructed to perform home exercises.
We found that the patients improved in all parameters, both directly after the treatment period and 6 months after the treatment period. If the patients continued with their home training during the 6-month follow-up period, this might explain the long-lasting effect.
Improvements in all parameters occurred in all study groups but were non-significant. One reason for the lack of significance might be the relatively low number of patients in the study groups from the start and also the low number of patients who continued to keep their pain diaries as requested at the last two follow-ups.
Conclusion
The clinical implications of our findings are that relaxation training induced the most pronounced effects directly after the treatment period, compared with acupuncture and physical training. There were no long-lasting differences between the interventions. All treatments reduced the symptoms of CTTH. Owing to the multifactorial causes of CTTH, a combination of relaxation training, physical training and acupuncture would perhaps generate the best result. Further studies are needed to investigate the effect of such a combination.
Footnotes
Acknowledgements
This study was supported by grants from Vårdalsstiftelsen, Kommunala Landstingsförbundet för Landstingsangelägenheter, the Renee Eanders Fond, and GlaxoSmith Kline. Thanks to all colleagues at Distriktssjukgymnastiken, Partille Primärvård, KrokslättsVårdcentral and Partille Sjukgymnastik, and especial thanks to Lotta Kymmer.