
Abstract
Few cluster-like headaches have been described. Idiopathic intracranial hypertension (IIH) presents with headaches in more than 90± of patients. We describe a male patient with new onset cluster-like headache secondary or related to IIH.
Keywords
Case report
A 40-year-old black patient presented with a new-onset headache of 1 month that had started 2 weeks after a mild viral infection. He described a severe (10/10) throbbing, stabbing pain around and behind the left eye and ipsilateral temporal area. The headache was associated with ipsilateral conjunctival injection, tearing of the eye, eyelid oedema, nasal congestion and rhinorrhoea, and a sensation of restlessness, of 2 h duration. The headache frequency was between two and three attacks per day, 3–4 days per week. At least one headache attack occurred during sleep. None of the attacks was associated with migrainous symptoms. The headache did not improve with common analgesic medications. The patient had first consulted an ophthalmologist who noted bilateral papilloedema (Fig. 1); because of this, the patient was referred to the neurologist.
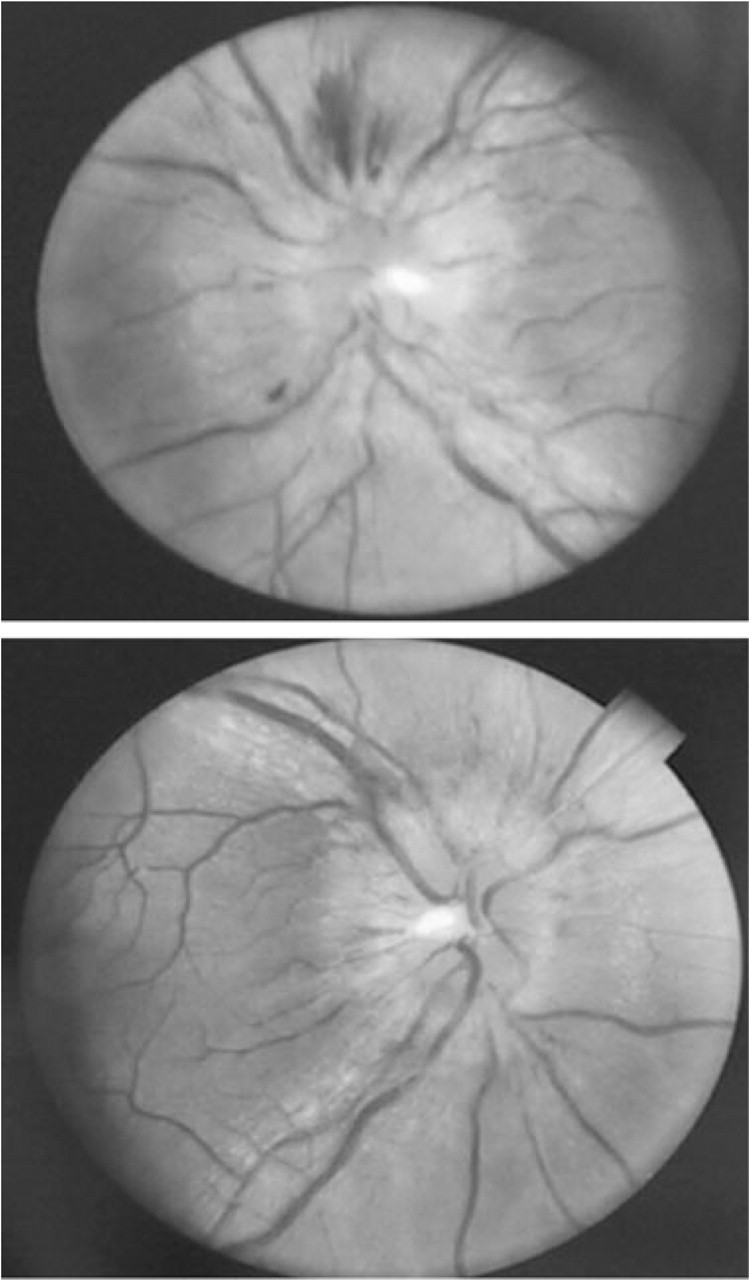
Funduscopic evaluation during the papilloedema and during the resolution period.
On physical examination, blood pressure was 140/90, pulse 76/min, weight 76 kg and height 1.73 m, with normal neck, cardiopulmonary and abdominal evaluations. On neurological examination he had bilateral papilloedema, with no other abnormalities. Past medical history was unremarkable; family history was positive for hypertension in both parents and migraine in one sister.
With a presumed diagnosis of intracranial hypertension (IH), a computed tomographic scan and magnetic resonance imaging–venography of the brain with and without contrast were done 5 and 6 weeks after the headache onset, respectively, both of which were normal. A lumbar puncture done at the end of the sixth week in a right lateral decubitus position was abnormal, with an opening pressure of 270 mmH2O. Cerebrospinal fluid examination revealed a cell count of four lymphocytes, glucose 53, protein 37 and negative microbiological studies [Venereal Disease Research Laboratory (VDRL), direct, Gram, KOH, mycobacterium, aerobic and fungus cultures negative]. The serum glucose, electrolytes, serum white blood count, sedimentation rate and C-reactive protein, thyroid, liver and kidney function were normal, and serum antinuclear antibodies, anticardiolipin antibodies, lupus anticoagulant, VDRL and HIV were negative.
Because of the patient's failure to respond to previous analgesic treatment and the notable high blood pressure, abortive treatment was initiated with oxygen through a non-rebreathing mask 7 l/min, resulting in complete headache control within 20 min for some of the attacks. Acetazolamide 250 mg t.i.d., initiated 7 weeks after the headache onset, was used as preventive treatment for 8 weeks. The headache ceased completely 3 weeks after acetazolamide initiation. A second lumbar puncture done at week 10 after headache onset showed normal opening pressure (180 mmH2O). The papilloedema resolved by the fifth month (Fig. 1); the patient was headache free after 8 months’ follow-up.
Discussion
Cluster headache (CH) is the most frequent trigeminal autonomic cephalalgia (TAC) (1). CH has a prevalence of 0.01–0.9%; in the UK the calculated prevalence can be as high as 0.1% and in the USA it is thought to affect 0.4% of males and 0.08% of females (male : female ratio of 2.5 : 1), with an incidence around 9.8/100 000 people per year (1).
Accurate CH diagnosis is routine in the presence of episodic ocular pain with conjunctival injection lasting >20 min with attack frequency less than five per day (P < 0.005) (2). The headaches described by our patient matched this clinical description, as well as the CH criteria of the second edition of the International Classification of Headache Disorders (ICHD-2) (1) (Table 1).
Cluster headache and idiopathic intracranial hypertension diagnostic criteria

CSF, Cerebrospinal fluid.
Modified from The International Classification of Headache Disorders.
Modified from Friedman (6).
Cluster-like headaches have been described related to intracranial pathologies, usually with atypical features (3–5).
Idiopathic intracranial hypertension (IIH) is a disease nine times more common in females, with an incidence of 0.9/100 000 in the general population, rising to 3.5/100 000 in women between 15 and 44 years old. Clinically, IIH can present with isolated IH, isolated papilloedema and isolated visual symptoms (Table 1) (6), Headache is described by more than 90% of patients (6). In our patient, headache and papilloedema were the predominant features.
In a retrospective study of 82 patients with treated IIH, 68% had headaches that met criteria for primary headaches as defined by the ICHD-1 (7); the most frequent were tension-type headache (30%), migraine without aura (20%), chronic tension-type headache (10%) and analgesic overuse headache (8%). Interestingly, one patient was diagnosed with cluster headache (1%) after the IIH was diagnosed. Unfortunately, no other clinical data are available (D. Friedman, personal communication) (7). Additionally, in a 10-year retrospective study of 16 patients from Colombia, headaches associated with IIH met criteria for migraine without aura or new daily persistent headache (8).
Clinically, the most important IIH finding is bilateral papilloedema (98–100%) (6). Definitive diagnosis of IIH relies on the elevated opening CSF pressure at lumbar puncture, with normal CSF composition and normal neuroimaging studies (6). Many conditions such as obstruction to venous drainage, endocrine disorders, autoimmune diseases, exogenous agents and infectious or post-infectious illnesses have been associated with IIH, although the only factors demonstrated in case–control studies are weight and obesity (6, 8).
Recent research points to the hypothalamus as the possible generator of CH (9). The hypothalamus is thought to have direct communication with C1-C2 spinal cord nociceptive neurons via the trigeminal system by the nucleus caudalis and the locus coeruleus. Additionally, a reflex is present between the trigeminal nucleus caudalis and the cranial parasympathetic superior salivatory nucleus (9, 10).
The pathophysiology of IIH is not clear. Hypotheses include increased or diminished CSF production, impaired CSF absorption and increased brain volume, and serotonin and norepinephrine abnormal regulation (6). There have been reports of elevated cerebral venous sinuses pressure, CSF outflow obstruction, decreased sinus wall compliance, reduced venous pulsatility and primary sinovenous stenosis (6, 10, 11).
Diminished anterior pituitary function (11), leptin abnormal secretion (12), morphological changes in the pituitary and interstitial brain oedema have been described with IIH (13, 14). Trigeminovascular system and cranial parasympathetic pathway activation secondary to hypothalamic dysfunction related to a hypothalamic–pituitary axis alteration could cause cluster-like headache. Additionally, there could be vascular nociceptive receptor activation (4), turning on local trigeminal pain fibres and/or autonomic nerves secondary to cavernous sinus and tributary venous outflow obstruction (5, 15).
This patient was previously headache free. The diagnosis of cluster-like headache secondary to IIH was based on clinical features and absence of positive laboratory findings. As a cautionary note, this patient fits criteria A–D for primary CH according to ICHD-2, but what makes likely secondary cluster-like headache caused or triggered by IIH is the temporal coincidence. The possibility of primary cluster is not easily dismissed and a longer follow-up will help to clarify the final diagnosis. Because of the intracranial hypertension and the clinical progression, we consider this patient should not be diagnosed with primary cluster headache.
To our knowledge, this is the first case report of cluster-like headache secondary to IIH in Colombia. It highlights the need for thorough physical and diagnostic testing in previously headache-free patients with new-onset headache, especially with TACs.