
Abstract
We have previously shown decreased lipolysis in both phases of cluster headache (CH), as an indication of a sympathetic dysregulation. Reduced lipolysis could be a result of diminished β-receptor sensitivity in adipose tissue. The aim of this study was to measure the lipolytic response to noradrenaline in 10 CH patients in remission and in 10 healthy subjects, to estimate β-receptor function. Microdialysis technique was used to measure the increase of glycerol, the end-product of lipolysis, during infusion of noradrenaline into the adipose tissue. Noradrenaline infusion resulted in a distinct elevation of glycerol. The average glycerol increase was significantly higher in CH patients (121± ± 48) than in healthy subjects (77± ± 41) (P < 0.05), which indicates increased β-receptor response to noradrenaline in CH patients in remission. This may be due to up-regulated β-receptor sensitivity, secondary to reduced sympathetic outflow and a primary autonomic disturbance in CH.
Introduction
Cluster headache (CH) attacks are associated with local cranial autonomic symptoms ipsilateral to the side of pain, as well as systemic autonomic effects on heart rate (1, 2), heart rate variability (3), circadian rhythmicity of blood pressure (4) and lipolysis (5). Findings from neuroendocrine studies (6), functional positron emission tomography (7) and magnetic resonance imaging volumetry (8) have demonstrated involvement of the posterior inferior hypothalamus in CH pathophysiology. The source of the autonomic disturbance in CH is still unclear. There is evidence for a local, postganglionic lesion (9), but since the hypothalamus is essential for the integration of autonomic nervous system signals, a disturbance in this area may lead to a generalized autonomic dysfunction in CH.
In a previous paper we have reported diminished nocturnal adipose tissue lipolysis in CH patients, both during the active headache period as well as in remission (5). Activation of the sympathetic nervous system is one of the major stimulating factors of lipolysis (10–12), mainly through release of noradrenaline (NA) from peripheral sympathetic nerve endings in the adipose tissue, but also via circulating catecholamines released from the sympatho-adrenal system. Catecholamines stimulate lipolysis by activation of β-receptors, which results in enhanced glycerol release, one of the end-products of lipolysis (13). Reduced lipolytic activity in CH may therefore be an effect of altered secretion of catecholamines or a primary defect in the β-receptor function in the adipose tissue.
Using the microdialysis technique, it is possible to measure glycerol concentrations continuously in subcutaneous adipose tissue, as an estimate of the lipolytic rate. It is also possible to add different substances to the perfusion fluid, which provides a unique opportunity to mimic the release of substances in situ and to measure the acute metabolic response.
The aim of this study was to investigate the lipolytic response to NA in CH patients in remission, as an estimate of the local β-receptor function in adipose tissue. By using the microdialysis technique, NA was perfused into the subcutaneous adipose tissue and glycerol concentrations were compared between CH patients and healthy subjects.
Materials and methods
Subjects
Ten patients, suffering from CH according to the 2nd edition of the International Headache Society criteria (14), participated. All patients were in remission phase. One CH patient had mild hypertension and was medicated with hydrochlorotiazid + amilorid, otherwise all patients were healthy and took no chronic medication. In addition, 10 healthy volunteers were included, none of them suffering from headache (Table 1). The Ethics Committee of Karolinska University Hospital approved the study and written informed consent was obtained from all subjects.
Clinical characteristics of cluster headache (CH) patients and healthy subjects

CH patients and healthy subjects were matched with regard to sex, body mass index (BMI) and smoking habits. With respect to age, CH patients were significantly older than healthy controls.
P < 0.05 (Mann–Whitney U-test).
Microdialysis device
The microdialysis catheter consisted of a double-lumen cannula with a semipermeable membrane at the top. The catheter was inserted into the adipose tissue and perfused with a physiological solution. The outgoing dialysate mirrored the composition of the extracellular space (15, 16). It was also possible to add different substances to the perfusion fluid. Variations in adipose tissue blood flow (ATBF) may influence extracellular fluid composition. In the present study, ATBF was measured using the ethanol technique (17).
Study protocol
All subjects attended the hospital the day before the study day. With help of a guide cannula (1.4 × 54 mm), two microdialysis catheters (CMA 60, 0.6 × 30 mm, molecular cut-off 20.000 kDa; CMA/Microdialysis AB, Stockholm, Sweden) were inserted into the abdominal subcutaneous adipose tissue, on each side of the umbilicus. Using a high-precision pump (CMA 106 or 107; CMA/Microdialysis AB), the catheters were perfused with Ringer's solution at a rate of 0.3 µl/min. In addition, a third catheter for simultaneous blood flow measurements was implanted about 5 cm away from the second one and perfused with Ringer's solution containing 5 m
All subjects had fasted from 18.00 h, although they were allowed to drink water. They were not allowed to smoke. On the study day, study subjects arrived at the hospital at 08.30 h. From the two first catheters, dialysates were collected every 20 min for 2 h, after which the catheters were perfused with NA (10−6
Analyses
Dialysate concentrations of glycerol and glucose were measured with a commercial method using enzymatic reagents and colorimetric measurements (CMA 600 Microdialysis Analyser; CMA/Microdialysis AB). The ethanol ratio used for blood flow measurements was determined using an enzymatic fluorometric method (18).
Evaluation
After analysis of all samples, one of the two catheters was selected systematically in accordance with predetermined criteria (5). First, as a measure of recovery, the majority of the basal samples had to have dialysate glucose concentrations of ≥3.5 mmol/l. If both catheters met the first criterion, the catheter with the least number of missing values was chosen. The mean basal concentrations of glycerol and glucose were calculated from three samples collected during 60 min before addition of NA. Glycerol data are presented as the maximum increase as well as the average increase during infusion of NA and expressed as a percentage of basal concentration as well as in absolute values when applicable. ATBF is presented as ethanol outflow/inflow ratio. An increase in blood flow is indicated by a decrease in ethanol outflow/inflow ratio.
Statistics
Glycerol and glucose data were estimated to be normally distributed and Student's t-test was used for comparisons between CH patients and healthy controls. When comparing the time from addition of NA to maximum glycerol concentration as well as the data for ethanol outflow/inflow ratio, non-parametric statistics (Mann–Whitney's U-test) were applied.
Results
Glycerol
In all subjects, addition of NA resulted in a distinct increase in microdialysis glycerol concentrations (Fig. 1a). The average glycerol increase during infusion of NA, expressed as percentage of basal concentration, was significantly higher in CH patients than in healthy subjects (Table 2). Expressed in absolute values, the maximum glycerol increase and the average glycerol increase were higher in CH patients than in healthy subjects, but these differences did not reach statistical significance (Table 2). In all CH patients except one the maximum concentration after addition of NA occurred in the first 20-min sample. In healthy subjects, the peak concentration occurred in the first 20-min sample in five subjects, in the second in four subjects and in the third in one subject, but the time of the peak concentration did not differ significantly between CH patients and healthy subjects. Baseline concentrations of interstitial glycerol were similar in CH patients and healthy subjects (Table 2).
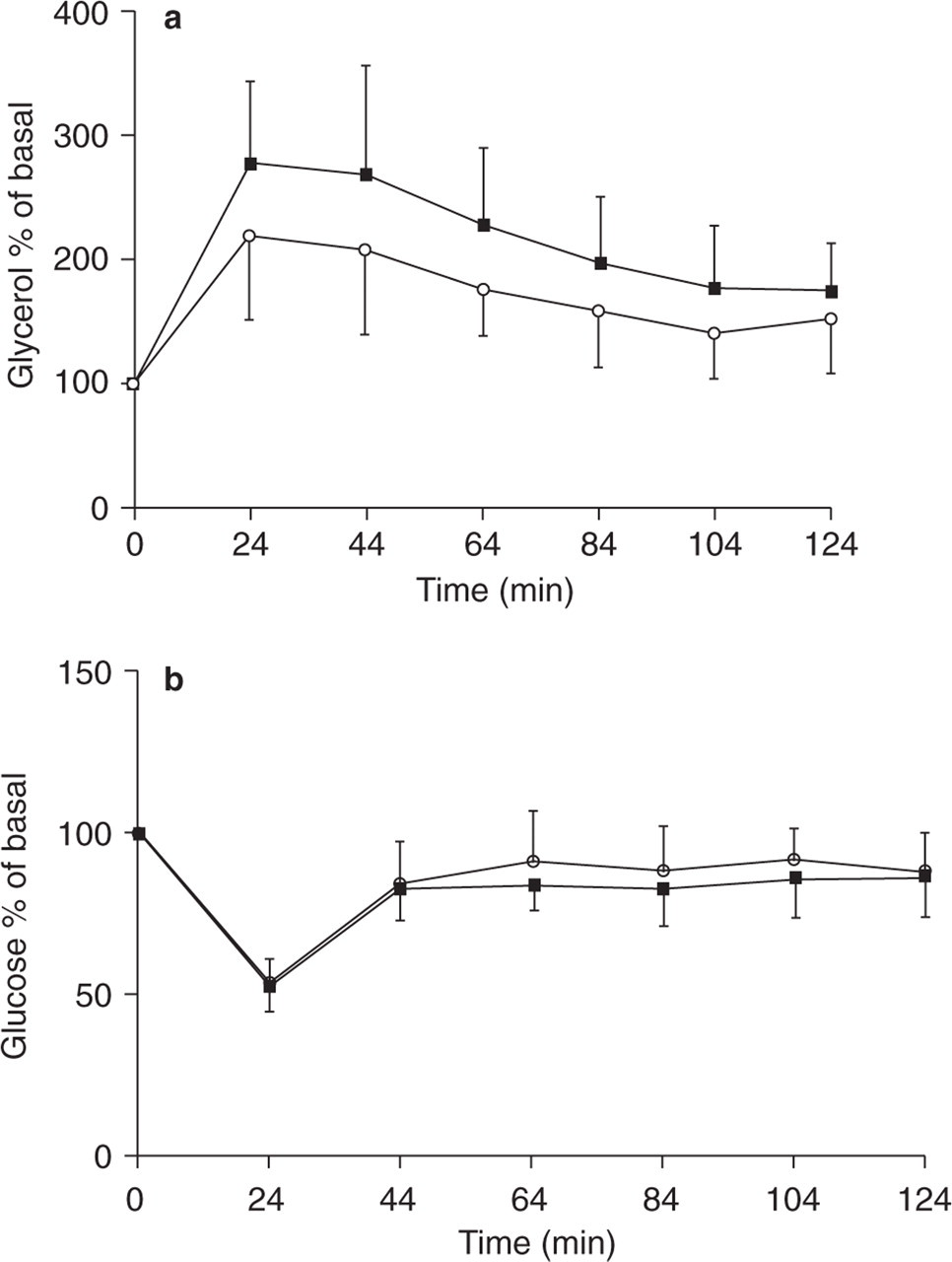
The effect of noradrenaline (NA) (10−6
The effect of infusion of noradrenaline on lipolysis in cluster headache (CH) patients and healthy subjects

A mean baseline value was calculated during 1 h, after which noradrenaline (NA) was added to the perfusion fluid. In CH patients, as well as in healthy subjects, addition of NA resulted in a marked, statistically significant elevation of glycerol in both groups (P < 0.01, Student's t-test for dependent samples). The average glycerol increase during infusion of NA, presented as a percentage of the basal level, was significantly higher in CH patients than in healthy subjects. In CH patients, the maximum response to NA was slightly higher than in healthy subjects, but the difference did not reach statistical significance.
CH patients were found to be a mean 10 years older than healthy subjects (Table 1). For that reason, regression analysis was carried out to evaluate if age influenced the outcome of the variable maximum glycerol increase and average glycerol increase in the age range of CH patients and controls. However, no significant correlation was found.
Glucose
Mean basal glucose concentrations were 4.91 ± 0.64 mmol/l (mean ± SD) in CH patients and 4.64 ± 0.56 mmol/l in healthy subjects. Twenty-four minutes after addition of NA to the perfusion fluid, both CH patients as well as healthy subjects demonstrated a significant decrease in glucose concentrations (Fig. 1b). In CH patients, glucose concentrations dropped by 47.3 ± 8.2% (P < 0.0001) and in healthy subjects by 46.4 ± 7.5% (P < 0.0001). The nadirs did not differ between groups. The average glucose concentration during infusion of NA was 3.88 ± 0.63 mmol/l in CH patients and 3.80 ± 0.48 mmol/l in healthy subjects. There was no difference between the groups.
Adipose tissue blood flow
It was possible to measure the ethanol outflow/inflow ratio in eight CH patients and six healthy subjects. Basal ratios did not differ between CH patients and healthy controls, nor did the average ethanol ratios after addition of NA to the adjacent catheter (data not shown). In healthy controls, the ethanol ratio dropped by 11% 24 min after addition of NA to the adjacent catheter and in CH patients by 1%. There was no significant difference in ethanol ratios between the groups (data not shown).
Discussion
The present study did not show any indications of diminished lipolytic response to NA in CH patients. In contrast, during NA infusion, average glycerol concentrations rose significantly higher in CH patients compared with healthy controls. The maximum response to NA tended to be higher also in the CH group, even though this difference was not significant. These results may indicate an increased β-adrenergic receptor response in CH patients. Therefore, our previous results showing lowered lipolysis at night in CH appear not to be explained by a decreased β-receptor response.
Up-regulation of β-adrenoceptor activity may be a result of hyponfuction of the sympathetic nervous system, such as reduced release of catecholamines, as has been shown in experimental studies of healthy subjects. During sustained head-down bed rest, resulting in sympathetic inhibition, increased lipolytic sensitivity to β-receptor agonists has been shown in adipose tissue (19) as well as increases in heart rate and vasodilatory responses (20). Indications of up-regulated adrenoceptors have also been observed in disorders with severe autonomic disturbance at both pre- and postganglionic level, such as multiple system atrophy (21) and diabetic peripheral neuropathy (22).
Activation of the β-receptors stimulates the adenylate-cyclase system via a stimulatory G-protein (Gs-protein) and results in an increase of cAMP concentrations and lipolysis. Catecholamines, mainly adrenaline, may also have a minor inhibitory effect on lipolysis via activation of α2-receptors and an inhibitory Gi-protein-mediated pathway (23). There are some previous suggestions of altered adrenoreceptor function in CH. Thus, studies have shown hypofunction of Gi-proteins (24) as well as diminished expression of Giα mRNA in lymphocytes (25), both in CH and in migraine, which may result in an altered balance between the activating and inhibiting signals to the adenylate-cyclase systems. In the present study, we were unable to demonstrate any significant differences in basal morning glycerol concentrations between CH patients and healthy subjects, which may indicate that other lipolytic factors and hormones have compensatory functions. From a clinical point of view there are also indications of altered adrenoreceptor function in CH. For example, the prophylactic effect of β-blockers in migraine is not observed in CH. In fact, exacerbation of the headache during treatment with β-blockers has been noticed (26).
When evaluating the results, the effect of the microcirculation has to be considered. An increase in blood flow (decreased ethanol outflow/inflow ratio) results in a decrease in interstitial glycerol concentrations, as circulating glycerol is transported out of the adipose tissue. In contrast, interstitial glucose concentrations will be increased (27, 28). In the present study, we could not demonstrate any major differences in ethanol outflow/inflow ratios or glucose concentrations between the groups. It is therefore unlikely that variations in microcirculation explain the difference in microdialysis glycerol concentrations.
The lipolytic response to catecholamines has been reported to be blunted in 50–78-year-old healthy individuals compared with 20–30-year-old subjects (29). Our CH patients were found to be about 10 years older than the healthy controls, but the lipolytic response was higher in the CH patients, not lower. Furthermore, in this cohort of subjects ranging from 30 to 67 years old, regression analysis showed no significant correlation between age and glycerol concentrations. It is therefore not likely that the difference in increased lipolytic response in CH is explained by age.
When evaluating the results, circadian variation has to be considered. In healthy subjects, lipolysis in adipose tissue has been shown to have a distinct circadian rhythm with a gradual increase during the night (30). Also, the sympathetic nervous system shows a circadian rhythm with nadirs for NA and adrenaline secretion in the middle of the night (31). In the previous study we showed reduced nocturnal adipose tissue lipolysis in CH patients, but also a different nocturnal lipolysis rhythm in CH patients in remission (5). With the protocol used in the present study, studying the β-receptor response in the morning between 09.00 h and 13.00 h, we found no reduction in the lipolytic response to NA. This clearly indicates that there is no primary β-adrenergic receptor dysfunction in patients with CH. In contrast, we observed a slightly increased β-receptor response in CH patients. This could be a result of lowered sympathetic activity at night leading to increased sensitivity of the β-receptors in the morning. However, disturbed secretion of other hormones affecting both lipolysis and β-adrenergic function, such as cortisol and Growth Hormone (GH) (32), may also be of importance.
In conclusion, an enhanced β-receptor response to NA, as seen in CH patients, could be due to sensitization of the β-receptors or alterations of the postreceptor cascade, as a result of reduced sympathetic activity. These findings may be interpreted as support for a generalized, sympathetic dysfunction in CH. Whether this disturbance is localized in the hypothalamus or anywhere downstream of the sympathetic pathway is still unclear. The fact that our patients were studied in the remission phase indicates that the autonomic disturbance in CH not only is a secondary effect of the active headache period but may be interpreted as a primary autonomic dysfunction.
Acknowledgements
This study was supported by grants from VR 9941, Svenska Frimurare barnorden, GlaxoSmithKline AB, Sweden and AstraZeneca AB, Sweden.