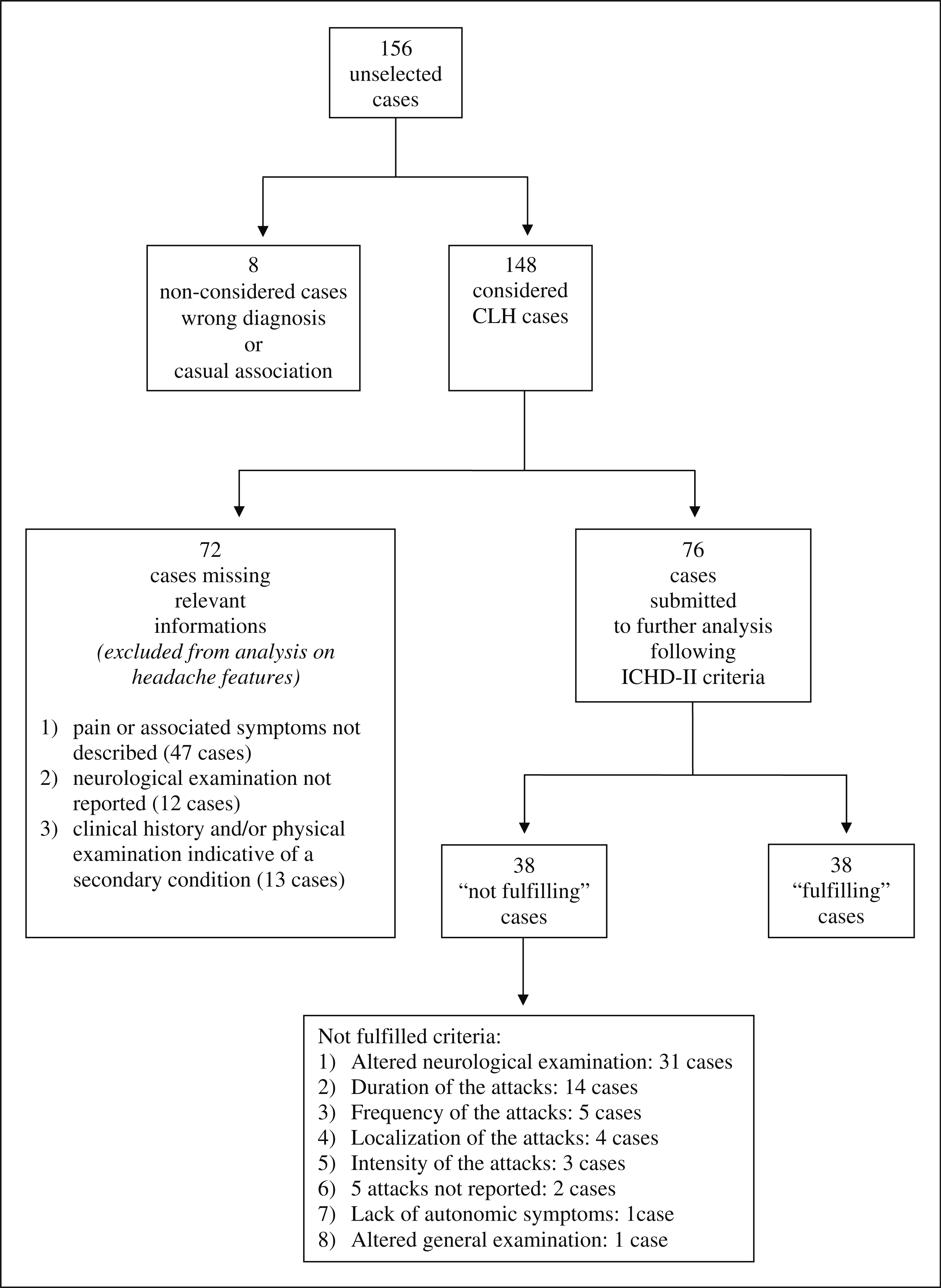
Among the primary headaches, cluster headache (CH) presents very particular features allowing a relatively easy diagnosis based on criteria listed in Chapter 3 of the International Classification of Headache Disorders (ICHD-II). However, as in all primary headaches, possible underlying causal conditions must be excluded to rule out a secondary cluster-like headache (CLH). The observation of some cases with clinical features mimicking primary CH, but of secondary origin, led us to perform an extended review of CLH reports in the literature. We identified 156 CLH cases published from 1975 to 2008. The more frequent pathologies in association with CLH were the vascular ones (38.5%, n = 57), followed by tumours (25.7%, n = 38) and inflammatory infectious diseases (13.5%, n = 20). Eighty were excluded from further analysis, because of inadequate information. The remaining 76 were divided into two groups: those that satisfied the ICHD-II diagnostic criteria for CH, ‘fulfilling’ group (F), n = 38; and those with a symptomatology in disagreement with one or more ICHD-II criteria, ‘not fulfilling’ group (NF), n = 38. Among the aims of this study was the possible identification of clinical features leading to the suspicion of a symptomatic origin. In the differential diagnosis with CH, red flags resulted both for F and NF, older age at onset; for NF, abnormal neurological/general examination (73.6%), duration (34.2%), frequency (15.8%) and localization (10.5%) of the attacks. We stress the fact that, on first observation, 50% of CLH presented as F cases, perfectly mimicking CH. Therefore, the importance of accurate, clinical evaluation and of neuroimaging cannot be overestimated.
Although the first description of cluster headache (CH) is credited to the Dutch doctor Nicolaas Pieterszoon Tulp in 1641, and other authors like Willis (1), Van Swieten (2) and Oppermann (3) later noted isolated occurrences with similar features, CH acquired nosographic status only in the 1930s, when it received the eponym of Horton's headache and later of histaminic cephalalgia (4). The current name was introduced by Kunkle in 1952 (5). Already included in the first edition (1988) of the International Headache Classification (6), at present CH diagnostic criteria are defined in Chapter 3 of the International Classification of Headache Disorders, 2nd edn (ICHD-II) (7), according to which there must be at least five attacks; severe unilateral pain in the orbital, supraorbital and temporal areas associated with at least one of the following symptoms: ipsilateral conjunctival injection and/or lacrimation, nasal congestion and/or rhinorrhoea, eyelid oedema, forehead and facial sweating, miosis and/or ptosis, a sense of restlessness; and duration of the attacks ranging from 15 to 180 min with frequency of attacks from one every other day to eight per day. It is, of course, necessary to exclude secondary causes. A feature frequently mentioned by patients suffering from this disease, but which does not appear among the ICHD-II criteria, is the circadian and circannual rhythm of the attacks. Depending on the duration of the interictal phase, CH can appear either in an episodic form (remission periods > 1 month, ICHD-II code 3.1.1) or in a chronic form (remission periods < 1 month, ICHD-II code 3.1.2). In typical cases, diagnosis is not particularly difficult as it might be when one or more of the main features required by the classification is missing or when other atypical elements are present. On the other hand, it is well known that clinical features, which at the beginning are virtually indistinguishable from a primary headache, may later turn out to be related to a secondary cause: this is true not only for tension-type headache, due to its relatively non-specific features, but also for primary headaches possessing more particular characteristics such as migraine and CH. As in our recent study of rarer trigeminal autonomic cephalalgias (8), we carried out a comprehensive review of the literature on symptomatic cluster-like headache (CLH) cases published from 1975 to August 2008, with the aim of highlighting the main features that could lead to an early suspicion of a secondary condition.
Materials and methods
A literature search was carried out on Medline (Pubmed and Winspirs; keywords: cluster-like headache; symptomatic cluster headache; symptomatic headache; atypical cluster headache; vascular pathology and cluster headache; tumoral pathology and cluster headache; inflammatory pathology and cluster headache; post-traumatic cluster headache; neurological diseases and cluster headache), on Medical Current Contents and on the references of each article. The research was limited to papers written in English, French, German, Italian and Spanish.
We identified 115 papers or abstracts (9–123) reporting a total of 156 cases in which the symptomatology was dominated by a cluster-like pain, which then turned out to be associated with a secondary condition (CLH). Although we did our best to include all cases mentioned in the literature, it is possible that some might have been omitted. All cases, including those published before the ICHD-I (1988) and ICHD-II (2004), were submitted to a rigorous control, reviewing the diagnoses following ICHD-II criteria, where restlessness has been added as a criterion as an alternative to presence of autonomic symptoms. Eight cases were excluded from any further examination since either the CLH diagnosis turned out to be wrong (9): a case of migraine with aura is clearly recognizable; (26,121): the diagnosis is more likely to be that of hemicrania continua), or its association with the reported disease was clearly not causal (11: case 5; 19,43: case 2; 111: cases 1 and 2). Cases were not excluded that did not report if headache was greatly reduced or resolved after successful treatment or spontaneous remission of the causative disorder (7). We are aware that only a positive outcome after removal of the associated condition would prove unequivocally the causal connection. However, since this information is often missing, the number of CLH patients would be drastically reduced to 38 (12,14,16,27: cases 2 and 3; 29: cases 1 and 2; 34,35: cases 1–3; 40,42,44,59,60,77,78: cases 1 and 2;
80,81,86,88,91,92,94,96,97,102,104,107,113,116: cases 1 and 2; 118–120,123).
Results
Among considered CLH patients (n = 148), 74.1% of the sample were male and 25.9% female, the M : F ratio being 2.7:1 (100/38, since data on patient gender were missing in 13 cases). The age of symptom onset was 42.8 ± 15.2 years, while the age of correct diagnosis was 47.0 ± 13.4 years. Cases were then divided in seven categories depending on the condition associated with cluster-like symptomatology (Figure 1): vascular pathologies (n = 57) (10,12,18,27: cases 2 and 3; 30,33,35: case 4; 38: cases 5 and 6; 39,41–43: case 6; 44,48,51,54,56,57,62: two cases; 65: two cases; 66,70,71,73–75,77,78: case 1; 80,83: two cases; 88,90,92,95,97,98,100,102,105: two cases; 107,108,112–114: two cases; 115: case 2; 116: two cases; 118,122,123) were the most common cause of CLH, followed by tumoral pathologies (n = 38) (14–17: two cases; 23,27: case 1; 32,34,35: case 2; 36: six cases; 38: case 4; 40,43: cases 3–5; 46,50,58,59,61,63,78: case 2; 86,94,96,101,103,106,109,115: case 1; 117,119), and by inflammatory/infectious diseases (n = 20) (13,21,22,25,29: two cases; 35: cases 1–3; 38: three cases; 43: case 1; 49,52,55,60,67–69,81). The remaining cases (n = 33) were classified as post-traumatic (n = 13) (11: cases 1–4; 20,24: four cases; 37,47,64,91); other central nervous system diseases (n = 9) (31,72,76,82,84,85,99,110,120); iatrogenic or drug-related conditions (n = 7) 45,53,79: three cases; 93,104); and dental pathologies (n = 4) (28,87): two cases; 89.
Criteria of selection of 156 cluster-like headache cases found in the literature.
Among these 148 cases, we decided to exclude from further analysis of headache features those missing relevant information (n = 72) or those presenting with a clinical history and/or a physical examination immediately indicative of a secondary condition. To be more precise, in 13 cases the clinical case history and/or the physical examination upon first observation clearly pointed to a secondary cause (64,69,79: three cases; 85,93,99,100,105: two cases; 110,115: case 1); in 12 cases (11: cases 1 and 2; 22,24: case 1; 28,47,55,78: case 2; 84,89,90,114: case 2) the neurological examination was not reported; in 47 cases (11: cases 3 and 4; 17: two cases; 18,20,23,25,29: case 2; 31,36: six cases; 38: six cases; 43: cases 1 and 3–5; 45,46,48–50,52,61,62: two cases; 65: two cases; 71,82,83: two cases; 95,98,101,108,112,117) the text did not describe the pain features and/or the associated symptoms during the attack.
The remaining 76 cases where divided into two groups, depending on whether the headache features described by the author fulfilled the requirements of a formal CH diagnosis according to the ICHD-II classification (‘fulfilling’ group, F: n = 38; 24.4% of total cases and 50.0% of cases considered more specifically) (13–16,21,24: cases 2–4; 27: three cases; 29: case 1; 32,34,37,40,41,43: case 6; 44,51,53,54,58,60,72–74,77,81,86,87: case 2; 91,94,96,103,104,113,123); or whether these features were not fulfilled or presented with one or more atypical elements (‘not fulfilling’ group, NF: n = 38; 24.4% of total cases and 50.0% of cases considered more specifically) (10,12,30,33,35: four cases; 39,42,56,57,59,63,66–68,70,75,76,78: case 1; 80,87: case 1; 88,92,97,102,106,107,109,114: case 1; 115: case 2; 116: two cases; 118–120,122).
Criteria for screening the case reports according to the data reported in the articles, and the number of selected patients, are summarized in the flow chart in Figure 1. Figure 2 shows CLH cases found in the literature (n = 148), divided according to their underlying condition. Within each disease category, the number of F and NF cases is provided, as well as that of those not further analysed for the reasons already specified.
Cluster-like headache cases of secondary origin (n = 148) reported in the literature (1975–2008) divided according to their underlying condition. Each disease category has been further subdivided in different groups, as reported in the text.
Vascular pathologies
This category was the first cause of CLH (38.5%; 57/148). Among CLH cases associated with vascular diseases, 21.0% (12/57) showed features fully in accordance with a formal CH diagnosis and were thus inserted in the F group; in one-half of them (n = 6) CLH proved to be secondary to aneurysm (27: cases 1 and 2; 43: case 6; 44,54,77); other reported cases could be ascribed to dural fistula (n = 2) (73,74), ischaemic injuries (n = 2) (41,51) and cerebral venous thrombosis (n = 2) (113,123).
Vascular cases classified as NF were 43.9% (25/57): arteriovenous malformation (n = 6) (10,12,30,33,35: case 4; 39); carotid artery dissection, extracranial (n = 9) (66,80,97,102,107,115,116: two cases; 118), intracranial (n = 1) (92), vertebral (n = 2) (57,122); medullary stroke (n = 2) (70,75); intracranial aneurysm of internal carotid artery (n = 2) (42,114: case 1); carotid endarterectomy (n = 1) (56); superficial temporal artery fistula (n = 1) (78); and subclavian steal syndrome (n = 1) (88). A case of arteriovenous malformation (12) may be considered as ‘Probable CH’, since it missed only one ICHD-II diagnostic criterion, that of attack duration.
Tumoral pathologies
The second most frequent cause of CLH was tumoral pathology (25.7%; 38/148), of which 31.6% (12/38) were included in the F group: pituitary adenomas (n = 5, of which four were prolactinomas) (14,27: case 3; 86,96,103, meningiomas (n = 2) (16,34), carcinomas of the paranasal structures (n = 2) (15,32), posterior fossa epidermoid carcinoma (n = 1) (40), fifth cranial nerve neurinoma (n = 1) (58), inflammatory myofibroblastic pseudotumour (n = 1) (94). No tumours of glial origin were found. Neoplastic cases included in the NF group were 15.8% (6/38): meningiomas (n = 3) (35: case 2; 59,119); multiple cerebral metastasis from lung carcinoma (n = 1) (63), cavernous sinus metastasis due to unidentified primitive tumour (n = 1) (106), and right epidermoid lesion of the clivus (n = 1) (109).
Inflammatory/infectious pathologies
CLH due to inflammatory/infectious diseases amounted to 13.5% of cases (20/148), of which five (25.0%) (13,21,29: case 1; 60,81) were included in the F group and four (20.0%) (35: cases 1–3; 67,68) in the NF group. Among F, two cases were associated with sphenoidal aspergillosis (60,81) and one each with ophthalmic herpes zoster (13), post infection from herpes simplex (21) and maxillary sinusitis (29: case 1). Among NF cases, two were associated with sinusitis (35: cases 1–3), one with sphenoidal aspergillosis (67) and one with infection from parainfluenza virus (68). Of the two cases associated with sinusitis, one (35: case 1) may be regarded as ‘Probable CH’, in that it missed only one ICHD-II diagnostic criterion, that of attack duration.
Post-traumatic pathologies
CLH associated with post-traumatic causes were 8.8% (13/148) and included non-concussive (n = 3) (24): case 3; (37,47) and concussive cranial trauma (n = 3) (24): cases 1, 2 and 4), orbital enucleation (n = 6) (11: cases 1–4; 20,64), and penetration of a foreign body in the maxillary sinus (n = 1) (91). Five cases could be assigned to the F group (24: cases 2–4; 37,91), none to NF.
Other neurological pathologies
These amounted to 6.1% of cases (9/148): multiple sclerosis (n = 3) (72,82,85); syringomyelia (n = 2) (84,99), one of which was associated with Arnold–Chiari malformation (99); idiopathic intracranial hypertension (n = 2) (110,120); retrobulbar neuritis associated with giant aneurysm (n = 1) (31); and orbital meningioma associated with cavernous sinus granulomatosis (n = 1) (76). Only one case, secondary to multiple sclerosis (72), was included in the F group and two, secondary to orbital meningioma plus granulomatosis of the cavernous sinus (76), and idiopathic intracranial hypertension (120), were assigned to NF group.
Iatrogenic or drug-related conditions
This category represented 4.7% (7/148) and included cocaine use (n = 3) (79: three cases), chemotherapy (n = 1) (45), warfarin therapy (n = 1) (93), tonsillectomy due to presence of a carcinoma (n = 1) (53), and intraocular lens implant (n = 1) (104). These last two cases were included in the F group. None was assigned to the NF group.
Dental pathologies
CLH associated with dental pathologies were 2.7% (4/148): inclusion of the upper wisdom tooth in the pterygopalatine fossa (n = 1) (28), tooth extraction (n = 2) (87: two cases), and periostitis of the third upper molar (n = 1) (89). Only one case (87: case 2), associated with tooth extraction, was included in the F group. A second tooth extraction case (87): case 1), included in the NF group, was compatible with the diagnosis of ‘Probable CH’, since it missed only one diagnostic criterion, that of attack duration.
Fulfilling group
As stated above, the F group includes those CLH cases in which the features of the headache, upon first clinical observation, made it possible to issue a formal CH diagnosis (n = 38) as there was full accordance with ICHD-II requirements. Table 1 reports the cases belonging to this group, in their chronological order of publication. The onset age was 43.0 ± 15.7 years, while that of the diagnosis was 48.4 ± 14.0 years. The M : F ratio was 4.4:1 (31:7). As reported in Figure 2, vascular diseases accounted for 31.6% (n = 12); tumoral diseases were second (31.6%, n = 12), followed by inflammatory/infectious diseases (13.1%, n = 5). Other conditions (as a whole, 23.7%), included post-traumatic cases (n = 5) and multiple sclerosis, tonsillectomy due to carcinoma, intraocular lens implant, and dental extraction (one case for each condition) (Figure 2).
‘Fulfilling’ cases (n = 38), i.e. cluster-like headache patients in whom the clinical features, upon first clinical observation, were fully in accordance with International Classification of Headache Disorders, 2nd edn diagnostic criteria for cluster headache
Year
Reference
Associated pathology
Sex
Age at diagnosis, years
Age at onset, years
1982
Sacquegna et al.
Herpes zoster ophthalmicus (left side)
M
49
49
1982
Tfelt-Hansen et al.
Pituitary adenoma
M
52
21
1983
McKinney
Orbital exenteration (squamous cell carcinoma)
M
45
43
1984
Kuritzky
Upper cervical meningioma
M
68
68
1985
Joseph and Clifford Rose
Facial herpes simplex
M
42
35
1987
Reik (case 2)
Concussive head trauma
M
39
35
1987
Reik (case 3)
Non-concussive head trauma
M
24
22
1987
Reik (case 4)
Frontal skull fracture
M
63
20
1988
Greve and Mai (case 1)
Anterior communicating artery aneurysm + SAH
M
47
44
1988
Greve and Mai (case 2)
Left carotid artery aneurysm + dilated right carotid artery
M
58
52
1988
Greve and Mai (case 3)
Prolactinoma
M
58
57
1988
Takeshima et al.
Left fronto-ethmoidal-maxillary sinusitis
M
31
31
1989
Appelbaum and Noronha
Left nasopharyngeal carcinoma
M
45
45
1989
Hannerz
Left parasellar meningioma
M
40
28
1990
Formisano et al.
Right fronto-temporal-parietal subdural haematoma
M
39
39
1991
Levyman et al.
Epidermoid tumour of the posterior fossa
F
53
39
1991
Narbone et al.
Third ventricle calcified lesion + ischaemic temporal lesion
M
69
60
1991
Tschopp and Mumenthaler (case 6)
Anterior communicating artery aneurysm
M
29
29
1991
West and Todman
Right vertebral aneurysm
M
51
39
1993
Trucco and Badino
Left parietal-thalamic-mesencephalic ischaemic lesion
M
72
70
1993
Bonazzi et al.
Post-tonsillectomy
M
58
58
1994
Koenigsberg et al.
Cavernous sinus pseudoaneurysm
F
52
52
1995
Masson et al.
Left trigeminal neurinoma
M
45
43
1995
Zanchin et al.
Sphenoidal aspergilloma
F
64
64
1999
Leandri et al.
Multiple sclerosis
M
42
42
1999
Prat et al.
Dural fistula
M
57
35
1999
Relja et al.
Dural fistula of cavernous sinus
M
78
78
2000
McBeath and Nanda
Anterior communicating artery aneurysm
M
55
45
2000
Mainardi et al.
Sphenoidal aspergilloma
F
65
65
2001
Porta-Etessam et al.
Prolactinoma
M
30
28
2001
Sörös et al. (case 2)
Dental extraction
F
47
47
2002
Scorticati et al.
Foreign body in the maxillary sinus
F
34
26
2003
Bigal et al.
Inflammatory myofibroblastic pseudotumour
M
22
13
2003
Minguzzi et al.
Prolactinoma
F
49
46
2005
Negoro et al.
Prolactinoma
M
17
14
2005
Maggioni et al.
Intraocular lens implant
M
55
55
2007
Georgiadis et al.
Cerebral venous thrombosis
M
46
46
2008
Rodríguez et al.
Cerebral venous thrombosis
M
51
51
References are listed in chronological order.
SAH, subarachnoid haemorrhage.
Of the 38 cases belonging to this group, 29 featured a side concordance between pain and the underlying condition; in two cases pain occurred on the contralateral side; in seven cases it was not possible to obtain this information. In 12 cases the symptomatology completely ceased after surgery on what was considered to be the main cause (14,16,27: case 2; 34,40,44,60,74,77,94,96,104); in eight cases pain disappeared with medical therapy (27: case 3; 29: case 1; 54,58,86,87: case 2; 113,123). The presence of circadian rhythm of the attacks was observed in 19 cases (13,16,21,24: cases 2 and 3; 40,43,44,53,58,60,72,74,77,81,94,96,104,113); it was absent in four cases (14,27: case 2; 87,103); it was not reported in 15 cases (15,24: case 1; 27: cases 1 and 3; 29,32,34,37,41,51,54,73,86,91,123).
Not fulfilling group
This group includes the 38 CLH patients who on the first observation presented at least one feature not in agreement with ICHD-II diagnostic criteria, thus not allowing a formal diagnosis of primary CH but, for the rest, with a clinical picture that mimicked CH. Table 2 shows the cases belonging to this group. The onset age was 43.6 ± 14.1 years, while that of diagnosis was 46.6 ± 12.5 years. The M : F ratio was 2.8:1 (28:10). As reported in Figure 2, vascular diseases accounted for most of the cases (65.8%; n = 25), followed by tumours (15.8%; n = 6) and inflammatory/infectious diseases (10.5%; n = 4); in the three remaining cases headache was secondary, respectively, to orbital meningioma/granulomatosis, idiopathic intracranial hypertension and dental extraction.
‘Not fulfilling’ cases (n = 38), i.e. the cluster-like headache patients in which the clinical features, upon first clinical observation, were not in accordance with International Classification of Headache Disorders, 2nd edn diagnostic criteria for cluster headache
Year
Reference
Associated pathology
Sex
Age at diagnosis, years
Age at onset, years
1975
Thomas
AVM of right temporal superficial artery
M
39
33
1982
Mani and Deeter
AVM of left occipital artery
F
36
22
1988
Testa et al.
AVM of left cerebellar artery
F
33
27
1989
Gawel et al.
AVM of anterior cerebral artery + AVM of corpus callosum
M
44
18
1989
Molins et al. (case 1)
Left maxillary sinusitis
F
59
59
1989
Molins et al. (case 2)
Maxillary sinusitis
M
40
40
1989
Molins et al. (case 3)
Right sphenoidal meningioma
M
66
66
1989
Molins et al. (case 4)
AVM of left middle cerebral artery
M
24
24
1991
Hindfelt and Olivecrona
AVM of left temporal lobe
M
49
48
1991
Todo and Inoya
Left aneurysm of intracranial internal carotid artery
M
44
44
1994
Björne et al.
Post left carotid endoarteriectomy
M
55
20
1995
Cremer et al.
Right vertebral artery dissection
M
67
64
1995
Taub et al.
Tentorial meningioma
M
60
37
1996
Tajti et al.
Multiple brain metastases of lung cancer
M
55
55
1997
Rosebraugh et al.
Carotid artery dissection
M
34
34
1997
Heidegger et al.
Left orbito-sphenoidal aspergilloma
M
68
68
1998
Blanchard
Parainfluenza virus infection
M
66
66
1999
de la Sayette et al.
Spinal infarction (C2)
M
54
54
2000
Cid et al.
Lateral medullary infarction
M
37
37
2000
Göbel et al.
Orbital meningioma and cavernous sinus granulomatosis
F
33
33
2000
Seijo- Martinez et al.
Right superficial temporal artery fistula
M
17
17
2000
Aymerich et al.
Right extracranial internal carotid artery dissection
M
48
48
2001
Sörös et al. (case 1)
Dental extraction
M
48
48
2001
Piovesan et al.
Subclavian steal syndrome
F
60
51
2002
Mainardi et al.
Left intrapetrosal carotid artery dissection
F
41
41
2003
Frigerio et al.
Right extracranial internal carotid artery dissection
F
50
50
2005
Hannerz et al.
Right internal carotid artery dissection
M
58
58
2005
Palmieri et al.
Left cavernous sinus metastasis
F
60
60
2006
Razvi et al.
Right internal carotid artery dissection
M
44
44
2006
Massie et al.
Right epidermoid lesion of the clivus
M
39
36
2007
Valença et al. (case 1)
Left internal carotid artery aneurysm
M
47
47
2007
Straube et al. (case 2)
Left internal carotid artery dissection
M
35
35
2007
Rigamonti et al. (case 1)
Left internal carotid artery dissection
M
50
50
2007
Rigamonti et al. (case 2)
Right internal carotid artery dissection
M
49
49
2008
Tobin and Flitman
Left internal carotid artery dissection
M
55
55
2008
Alty et al.
Left trigeminal meningioma
M
30
nd
2008
Testa et al.
Idiopathic intracranial hypertension
F
28
28
2008
Kim et al.
Left vertebral artery dissection
F
48
48
References are listed in chronological order.
AVM, arteriovenous malformation.
Table 3 reports the NF cases, divided according to each specific ICHD-II criterion for the CH diagnosis that was not fulfilled. As a whole, the main ICHD-II criterion that upon first observation was not achieved resulted from physical examination: in 31 (81.6%) patients the suspicion of a secondary condition was raised by an altered neurological (n = 30) or general (n = 1) examination. Then, in descending order, a longer duration (36.8; n = 14); frequency (13.1%; n = 5); localization (10.5%; n = 4); intensity of headache, that was reported as moderate (7.9%; n = 3); in 5.2% (n = 2) fewer than five attacks had been present; in 2.6% (n = 1) attacks were not accompanied by autonomic symptoms. In all cases pain was described as strictly unilateral. Moreover, in detail, the six cases featuring a normal examination failed the following criteria. Three patients stated their attacks lasted > 180 min (12,35: case 1; 87); since they failed only one criterion, they fitted a formal ‘Probable CH’ diagnosis. In two cases the pattern differed from the primary CH diagnosis because of the presence of two atypical features, respectively, duration and localization (57) and duration and frequency (39). The last case featured four atypical elements (frequency, localization, duration and recurrence of attacks) (42). Table 4 reports the NF cases, divided according to the number and type of ICHD-II diagnostic criteria for CH not fulfilled upon first observation, which therefore should have raised the suspicion of an underlying secondary cause. One-half of the NF patients presented only one atypical feature, which was physical examination (15 patients neurological, one general), or duration (three patients). Of 38 cases belonging to this group, 31 featured a side concordance between pain and the underlying condition; in one case pain occurred on the contralateral side; in six cases it was not possible to obtain this information. In 18 cases the symptomatology completely ceased after the medical (35: cases 1 and 3; 42,80,92,97,102,107,116: cases 1 and 2; 118,120) or surgical (12,35: case 2; 59,78,88,119) treatment of the main cause; no mention of this important point was made in the remaining cases. The presence of circadian rhythm of the attacks was observed in 11 cases (10,33,35: cases 1 and 2; 67,68,80,92,102,106,115; it was absent in six cases (30,42,59,75,78,87); it was not reported in 20 cases (12,35: cases 3 and 4; 39,56,57,63,66,76,88,97,107,109,114,116: cases 1 and 2; 118–120,122); one case complained of a single CH attack, and therefore a circadian rhythm could not be confirmed (70).
Cluster-like headache (CLH) ‘not fulfilling’ cases (NF, n = 38)
ICHD-II criteria
Patients (n and %)
Authors
Neurological examination
31 (81.6%)
Thomas, 1975; Testa et al., 1988; Gawel et al., 1989; Molins et al., 1989 (cases 1-2-3); Björne et al., 1994; Taub et al., 1995; Tajti et al., 1996; Rosebraugh et al., 1997; Heidegger et al., 1997; Blanchard, 1998; de la Sayette et al., 1999; Cid et al., 2000; Göbel et al., 2000; Sejio-Martinez et al., 2000; Aymerich et al., 2000; Mainardi et al., 2002; Frigerio et al., 2003; Hannerz et al., 2005; Palmieri et al., 2005; Razvi et al., 2006; Massie et al., 2006; Valença et al., 2007 (case 1); Straube et al., 2007 (case 2); Rigamonti et al., 2007 (cases 1–2); Tobin and Flitman, 2008; Alty et al., 2008; Testa et al., 2008; Kim et al., 2008.
Duration
14 (36.8%)
Thomas, 1975; Mani and Deeter, 1982; Molins et al., 1989 (case 4); Hindfelt and Olivecrona, 1991; Todo and Inoya, 1991; Cremer et al., 1995; Cid et al., 2000; Aymerich et al., 2000; Sörös et al., 2001 (case 1); Mainardi et al., 2002; Razvi et al., 2006; Massie et al., 2006; Rigamonti et al., 2007 (case 1); Tobin and Flitman, 2008.
Frequency
5 (13.1%)
Hindfelt and Olivecrona, 1991; Todo and Inoya, 1991; de la Sayette et al., 1999; Sejio-Martinez et al., 2000; Alty et al., 2008.
Localization
4 (10.5%)
Testa et al., 1988; Todo and Inoya, 1991; Cremer et al., 1995; Taub et al., 1995.
Intensity
3 (7.9%)
Molins et al., 1989.
Five attacks
2 (5.3%)
Todo and Inoya, 1991; de la Sayette et al., 1999.
Autonomic symptoms
1 (2.6%)
Testa et al., 1988.
General examination
1 (2.6%)
Piovesan et al., 2001.
Unilaterality
0
International Classification of Headache Disorders, 2nd edn (ICHD-II) diagnostic criteria for cluster headache are listed, along with the number and percentage of CLH patients who did not meet them.
Cluster-like headache (CLH) ‘not fulfilling’ cases (NF, n = 38)
Not fulfilled criteria (n)
Patients (n and %)
Type of not fulfilled criterion
1
19 (50.0%)
Neurological examination (n = 16): Gawel et al., 1989; Björne et al., 1994; Tajti et al., 1996; Rosebraugh et al., 1997; Heidegger et al., 1997; Blanchard, 1998; Göbel et al., 2000; Frigerio et al., 2003; Hannerz et al., 2005; Palmieri et al., 2005; Valença et al., 2007 (case 1); Straube et al., 2007 (case 2); Rigamonti et al., 2007 (case 2); Testa et al., 2008; Kim et al. 2008.
General examination (n = 1) Piovesan et al., 2001.
Duration (n = 3): Mani and Deeter, 1982; Molins et al., 1989 (case 4); Sörös et al., 2001.
2
16 (42.1%)
Neurological examination + duration (n = 8): Thomas, 1975; Cid et al., 2000; Aymerich et al., 2000; Mainardi et al., 2002; Razvi et al., 2006; Massie et al., 2006; Rigamonti et al., 2007 (case 1); Tobin et al., 2008.
Duration + localization (n = 1): Cremer et al., 1995.
Duration + frequency (n = 1): Hindfelt and Olivecrona, 1991.
Duration + frequency + localization + <5 attacks (n = 1): Todo and Inoya, 1991.
Number and type of not fulfilled International Classification of Headache Disorders, 2nd edn diagnostic criteria for cluster headache are listed, along with the number and percentage of CLH patients who did not meet them.
Discussion
In general terms, when dealing with a diagnosis of secondary headache, an important causal relationship criterion to establish is the disappearance or clear improvement of headache when the associated condition is removed (7). This also holds true for patients presenting with a cluster-like symptomatology. In 2002 a review was published of 68 CLH cases occurring between 1980 and 2001 (124), fulfilling the strict requirements set forth by the authors, i.e. headache features compatible with CH diagnosis according to International Headache Society 1988 classification criteria (6); negative general and neurological examination both during attacks and in the interictal phase; localization of the second condition consistent with a likely triggering of the trigeminovascular system; and CLH symptom remission without recurrence after adequate treatment of the other conditions.
The assessment of the outcome after specific intervention on the alleged cause of pain is often difficult because of lack of information in the text and of various interpretations by the authors: in our study, only 38 cases report on the remission of symptoms following the lesion treatment. Focusing this evaluation on the two groups F and NF, which are considered most in detail and where all information relevant for a formal CH diagnosis is available, only in 27 cases is reference made to the disappearance of the symptoms after removal of the associated condition. Therefore, the cases that might be regarded as CLH sensu stricto would be too limited by lack of information, preventing any further analysis. Bearing in mind this choice, we selected the patients as specified in Materials and methods.
Age at onset
CH onset usually occurs between the third and the fifth decade (125). In a recent observational study carried out over three decades, the onset peak was placed between 20 and 29 years of age for both sexes (126): therefore, late onset of symptoms compatible with CH diagnosis would represent per se an element that requires attention, although onset in the elderly has been reported (127–129), particularly in female patients (130). The need for special caution for older groups is confirmed by our reappraisal of symptomatic cases, since the average onset in CLH patients turns out to be at the age of 42.7 years.
Interval between clinical onset and diagnosis
As a whole, in CLH the average time elapsed between symptom onset and correct diagnosis turns out to be 3.0 years in the NF group, whereas it stretches to 5.4 years in the F group. Therefore, the correct diagnosis in the F group of CLH, which so closely mimics CH, presents a delay of > 2 years in comparison with the NF group.
Male/female ratio
The concept that CH is chiefly a male disease has been challenged by two reports of a significant increase of cases in female patients, with a reduction of the male : female ratio from 5.9:1 to 3.1:1 (126) and 6.2:1 to 2.1:1 (129). In order to explain this, it has been assumed that this change may be due to social and cultural modifications that took place in recent decades, especially to changes in the behaviour and living habits of women, progressively more similar to those of men both in work and leisure. The behavioural factor, according to this view, should concur to determine the clinical occurrence of CH. On the other hand, CH also seems to be related to increasingly demonstrated genetic factors (131). However, the decrease of male:female ratio was reported in patient sample studies, and with a decreasing trend over years (126): ratio M:F from 5.9:1 for patients with CH onset before 1960 to 3.1:1 for patients with CH onset from 1990 to 1997; (129): ratio M:F from 6.2:1 for patients with CH onset before 1960 to 2.1:1 for patients with CH onset in the 1990s; (132): ratio M:F from 11:1 for patients with CH onset during 1982–1997 to 3.6:1 from 2001 to 2003), whereas in a recent meta-analysis (133) of population-based studies reporting on the epidemiology of CH up to August 2007, the overall sex ratio was 4.3 (range 1.3–14). Therefore, the authors did not confirm the finding that the sex ratio has changed over recent decades with an increasing rate of female cluster patients.
In our study, gender ratio in CLH is close to that reported in the last decade for CH (126,132), reaching 2.7:1. Unfortunately, due to the limited number of cases available in the literature, it has not been possible to evaluate the male:female ratio of CLH patients in the different decades of the period considered in our study (1975–2008), or to check if any trend could be detected. However, male prevalence is unexpected in CLH, where the identified secondary causes as a whole are not gender related, nor genetically determined, nor dependent on behavioural factors. A possible explanation could be the anatomical and possibly physiological differences of the hypothalamus in the two genders, since it is known that the male hypothalamus with its suprachiasmatic nucleus possesses a greater volume in comparison with the female one (134). If we accept this explanation, then these remarks would lead us to view CH as a clinical picture resulting in a multifactorial state where the interaction of genetics and environment acts on the structure of the hypothalamus, more susceptible in men than in women, whereas CLH male preponderance would be consequent on the hypothalamic anatomical differences between the two genders.
CLH-associated conditions
Vascular pathologies are largely represented among CLH patients, accounting for about one-third of cases; they are followed by tumoral pathologies (about one-fifth) and inflammatory (about 13%), as reported in Figure 2. It is difficult to state whether this is due to their higher incidence in the population, or if they favour per se the occurrence of CLH. Since the specific lesions are heterogeneous within different categories, it is likely that CLH occurrence is more related to the anatomical site involved than to a specific pathogenic role of the associated condition. This hypothesis is supported by evidence that the underlying conditions mostly involve the trigeminovascular system. The absence of the glial series from CLH-associated tumours is interesting: possibly the infiltrating nature lowers its potential to act on the structures triggering CLH.
Red flags
One of the main objectives of this review was to identify the possible atypical elements that are part of CLH symptomatology after the first observation, and that therefore can help in raising early suspicion of a secondary cause. Compared with CH, CLH cases, in our review, are present at older age at onset of about 42 years. Therefore, as stated before, late onset represents a condition that requires careful evaluation.
The analysis of the CLH NF group (Table 3) highlighted evidence that an altered neurological examination is the most frequent red flag, present in about three-quarters of these cases. Its importance is further stressed by the fact that this was the only suspect element in 16/38 NF patients (Table 4). An attack duration exceeding the limit of 180 min set forth by the ICHD-II constitutes another element of suspicion, present in more than one-third of NF cases (Table 3), usually along with other missing criteria, but in about 7% of cases as the only missing criterion.
A recent survey of 289 patients with ‘Probable CH’, missing only one diagnostic criterion for a CH diagnosis, showed that the criterion most often not met was attack duration, which in about 65% of these cases was > 180 min. Therefore, it was proposed to reconsider the criteria, suggesting a duration > 180 min (135). Our study has shown that, should the criterion of attack duration be extended to > 180 min, an important element raising the suspicion of a possible secondary origin could be lost, increasing the risk of classifying as CH forms that are actually CLH.
Other, less frequent, red flags are, in descending order of occurrence, localization of pain (10.5%) and frequency of attacks (13.1%); headache intensity, described as moderate in 7.9%. In 5.2% of cases fewer than five attacks occurred and in 2.6% the attacks did not present with accompanying symptoms.
Finally, it has to be stressed that, at first observation, 50% of CLH patients clinically presented as F cases, perfectly mimicking CH. Therefore, the likelihood that a secondary cause is responsible for a clinical picture mimicking a primary CH, albeit low, should always be considered to provide a correct diagnosis and appropriate treatment. In this context, besides accurate clinical evaluation, the importance of neuroimaging cannot be overestimated. This opinion is in accordance with the review by Favier et al. (136), which recommends neuroimaging in all patients with trigeminal autonomic cephalalgias. We suggest that the diagnostic management of a patient featuring CH symptoms should include cerebral magnetic resonance imaging (MRI) with contrast medium and further examinations in accordance with MRI findings or the clinical general or neurological picture. This measure, taking into consideration the low occurrence of the disease, justifies the relatively small economic outlay.
References
1.
WillisT. De Anima Brutorum. Oxford: E Theatro Sheldoniano, 1672.
2.
Van SwietenG. Commentaria in Hermanni Boerhaave Aphorismos de cognoscendis et curandis morbis. Vol. IILugduni Batavorum (Leiden): Apud Johannem et Hermanum Verbeek, 1745.
3.
OppermannJ. Dissertatio medica inauguralis de hemicrania horologica. Halle: Hilliges J1747
KunkleECPfeifferJRWilhoitWMHamrickLW. Recurrent brief headaches in ‘cluster’ pattern. Trans Am Neurol Assoc1952; 77: 240–3.
6.
Headache Classification Committee of the IHSClassification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia1988; 8(Suppl. 7): 1–96.
7.
Headache Classification Subcommittee of the International Headache SocietyThe International Classification of Headache Disorders, 2nd edition. Cephalalgia2004; 24(Suppl. 1): 1–160.
8.
TruccoMMainardiFMaggioniFBadinoRZanchinG. Chronic paroxysmal hemicrania, hemicrania continua and SUNCT syndrome in association with other pathologies: a review. Cephalalgia2004; 24: 173–84.
Tfelt-HansenPPaulsonOBKrabbeA. Invasive adenoma of the pituitary gland and chronic migrainous neuralgia. A rare coincidence or a causal relationship?. Cephalalgia1982; 2: 25–8.
15.
McKinneyAS. Cluster headache developing following ipsilateral orbital exenteration. Headache1983; 23: 305–6.
16.
KuritzkyA. Cluster headache-like pain caused by an upper cervical meningioma. Cephalalgia1984; 4: 185–6.
17.
LefèvreJPSimmatGBatailleBSallesMGilRBoissonnotLRoualdesG. Algies vascularies de la face dues à un méningiome. Presse Méd1984; 13: 2323–2323.
18.
MorettiGManzoniGCBanchiniEVillaniLGCusmanoF. Cluster headache: remission following ascending aorta/innominate artery bypass surgery. Case report. Ital J Neurol Sci1984; V: 319–21.
19.
CanepariCRivaM. Considerazioni a proposito di un caso di cefalea a grappolo e processo occupante spazio intracerebrale. Min Med1985; 76: 1285–7.
20.
PrusinskiALiberskiPRSzulc-KuberskaJ. Cluster headache in a patient without an ipsilateral eye. Headache1985; 25: 134–5.
21.
JosephRClifford RoseF. Cluster headache and herpes simplex: an association?. BMJ1985; 290: 1625–6.
22.
HardeboJE. An association between cluster headache and herpes simplex. N Engl J Med1986; 314: 316–316.
23.
BondJBWesleyRE. Cluster headache after orbital exenteration. Ann Ophthalmol1987; 19: 438–438.
24.
ReikL. Cluster headache after head injury. Headache1987; 27: 509–10.
25.
GiacovazzoMMartellettiP. Cefalea a grappolo insorta dopo sindrome di Ramsay Hunt ed antigeni del sistema HLA. Descrizione di un caso. Min Med1987; 78: 1029–30.
26.
De AngelisLMPayneR. Lymphomatous meningitis presenting as atypical cluster headache. Pain1987; 30: 211–16.
27.
GreveEMaiJ. Cluster headache-like headaches: a symptomatic feature?. Cephalalgia1988; 8: 79–82.
28.
RomoliMCudiaG. Cluster headache due to an impacted superior wisdom tooth: case report. Headache1988; 28: 135–6.
29.
TakeshimaTNishikawaSTakahashiK. Cluster headache like symptoms due to sinusitis: evidence for neuronal pathogenesis of cluster headache syndrome. Headache1988; 28: 207–8.
30.
TestaDFredianiFBussoneG. Cluster headache-like syndrome due to arteriovenous malformation. Headache1988; 28: 36–8.
31.
SjaastadOSaunteCFredriksenTAde Souza CarvalhoDFragosoYDDaleLGHørvenJ. Cluster headache-like headache, Hageman trait deficiency, retrobulbar neuritis, and giant aneurysm. Autonomic function studies. Cephalalgia1988; 8: 111–20.
GawelMJWillinskyRAKrajewskiA. Reversal of cluster headache side following treatment of arteriovenous malformation. Headache1989; 29: 453–4.
34.
HannerzJ. A case of parasellar meningioma mimicking cluster headache. Cephalalgia1989; 9: 265–9.
35.
MolinsALópezMCodinaATitusF. Cefalea agregada (cluster headache) sintomática? A propósito de cuatro observaciones. Med Clin (Barc)1989; 92: 181–3.
36.
GiacovazzoMDi SabatoFBernoniRMMartellettiP. Cefalea a grappolo, infezione da virus di Epstein-Barr e Linfoma di Burkitt. Eur Rev Pharmacol Sci1989; XI: 1–4.
37.
FormisanoRAngeliniADe VuonoGCalissePFiaccoFCatarciT. Cluster-like headache and head injury: case report. Ital J Neurol Sci1990; 11: 303–5.
38.
FrieraGJiménezMDIriarteL. Falsos casos de cefalea en racimos. Neurología1991; 6: 311–311.
39.
HindfeltBOlivecronaH. Cerebral arteriovenous malformation and cluster-like headache. Headache1991; 31: 514–17.
40.
LevymanCdos Santos Poça Dagua FilhoAMota VolpatoMParente SettanniFACerqueira de LimaW. Epidermoid tumor of the posterior fossa causing multiple facial pain—a case report. Cephalalgia1991; 11: 33–6.
41.
NarboneMCD'AmicoDDi MariaFArenaMGLongoM. Cluster-like headache and a median intracranial calcified lesion: case report. Headache1991; 31: 684–5.
42.
TodoTInoyaH. Sudden appearance of a mycotic aneurysm of the intracavernous carotid artery after symptoms resembling cluster headache: case report. Neurosurgery1991; 29: 594–9.
43.
TschoppPMumenthalerM. Symptomatische Clusterkopfschmerzen: Koinzidenz oder kausale Beziehung?. Nervenartz1991; 62: 383–7.
44.
WestPTodmanD. Chronic cluster headache associated with a vertebral artery aneurysm. Headache1991; 31: 210–12.
45.
GiacovazzoMDi SabatoFMartellettiP. Cefalea a grappolo insorta in soggetto affetto da morbo di Hodgkin in trattamento roentgen-chemioterapico, immunodepresso. Progr Med1991; 47: 19–20.
MassonCLehericySGuillaumeBMassonM. Cluster-like headache in a patient with a trigeminal neurinoma. Headache1995; 35: 48–9.
59.
TaubEArgoffCEWinterkornJMSMilhoratTH. Resolution of chronic cluster headache after resection of a tentorial meningioma: case report. Neurosurgery1995; 37: 319–22.
60.
ZanchinGRossiPLicandroAMFortunatoMMaggioniF. Clusterlike headache. A case of sphenoidal aspergilloma. Headache1995; 35: 494–7.
61.
MilosPHaveliusUHindfeltB. Clusterlike headache in a patient with pituitary adenoma. With a review of the literature. Headache1996; 36: 184–8.
TajtiJSasKSzokDVörösEVécseiL. Clusterlike headache as a first sign of brain metastases of lung cancer. Headache1996; 36: 259–60.
64.
EversSSörösPBrillaRGerdingHHusstedtIW. Cluster headache after orbital exenteration. Cephalalgia1997; 17: 680–2.
65.
FerraroRMaiquesJCPliegoLATraña MatusCGiannaulaRJ. Cluster type headache and brain lacunar infarction. J Neurol Sci1997; 150: S303–S303.
66.
RosebraughCJGriebelDJDiPetteDJ. A case report of carotid artery dissection presenting as cluster headache. Am J Med1997; 102: 418–19.
67.
HeideggerSMattfeldtTRieberAWikstroemMKernPSchreiberH. Orbito-sphenoidal aspergillus infection mimicking cluster headache: a case report. Cephalalgia1997; 17: 676–9.
68.
BlanchardBM. Cluster headache associated with parainfluenza virus, preceded and succeeded by migraine. Headache1998; 38: 132–4.
69.
Jiménez-JiménezFJGarcía-AlbeaEZurdoMMartínez-OnsurbePRuiz de VillaespesaA. Giant cell arteritis presenting as cluster headache. Neurology1998; 51: 1767–8.
70.
de la SayetteVSchaefferSCoskunOLeprouxFDeferG. Cluster headache-like attack as an opening symptom of a unilateral infarction of the cervical cord: persistent anaesthesia and dysaesthesia to cold stimuli. J Neurol Neurosurg Psychiatry1999; 66: 397–400.
71.
ErtseyCFolyovichABozsikGBodrogiLJelencsikL. Left internal carotid aneurysm causing trigeminal neuralgia followed by cluster-like headaches. Cephalalgia1999; 19: 432–3.
72.
LeandriMCruccuGGottliebA. Cluster headache-like pain in multiple sclerosis. Cephalalgia1999; 19: 732–4.
73.
PratJJatoMCallénAMartinezJACalopaMRubioF. Cluster-like headache secondary to dural fistula. Cephalalgia1999; 19: 430–1.
74.
ReljaGNiderGKoscicaNMuscoGNegroC. The role of cavernous sinus in cluster and other headaches. Ital J Neurol Sci1999; 20: S42–5.
75.
CidCGBercianoJPascualJ. Retro-ocular headache with autonomic features resembling ‘continuous’ cluster headache in lateral medullary infarction. J Neurol Neurosurg Psychiatry2000; 69: 134–134.
76.
GöbelHMehdornHMHeinzeAHeinze-KuhnKAustermannKLindnerV. Symptomatic cluster headache associated with granulomatous tissue in the cavernosus sinus: a case report. Cephalalgia2000; 20: 328–328.
77.
Mc BeathJGNandaA. Sudden worsening of cluster headache: a signal of aneurysmal thrombosis and enlargement. Headache2000; 40: 686–8.
78.
Seijo-MartínezMCastro del RíoMCervigonECondeC. Cefalea en racimos sintomática: presentación de dos casos. Neurología2000; 15: 406–10.
79.
PeñarrochaMBagánJVPeñarrochaMASilvestreFS. Cluster headache and cocaine use. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2000; 90: 271–4.
80.
AymerichJGallegoJSorianoGVillanuevaJA. Diseción carotidea extracraneal manifestada como cefalea en brotes. Rev Neurol2000; 31: 594–5.
KitamiK. Cluster headache-like pain in carotid cavernous fistula: report of two cases. Cephalalgia2001; 21: 512–512.
84.
MorísGVidalJAMoralA. Is there a causal association between upper cervical spine pathology and cluster headache or is this an uncommon coincidence?. Cephalalgia2001; 21: 514–514.
85.
LüttmannRJFreseABethkeFHusstedtIWEversS. Multiple sclerosis diagnosed in a cluster headache patient—a case report. Cephalalgia2001; 21: 515–515.
86.
Porta-EtessamJRamos-CarrascoABerbel-GarcíaÁMartínez-SalioABenito-LeónJ. Clusterlike headache as first manifestation of a prolactinoma. Headache2001; 41: 723–5.
87.
SörösPFreseAHusstedtIWEversS. Cluster headache after dental extraction: implications for the pathogenesis of cluster headache?. Cephalalgia2001; 21: 619–22.
88.
PiovesanEJLangeMCWerneckLCKowacsPAEngelhornAL. Cluster-like headache. A case secondary to the subclavian steal phenomenon. Cephalalgia2001; 21: 850–1.
89.
90.
ShapiroRE. Chronic cluster headache associated with a contralateral hypothalamic cyst. Headache2002; 42: 412–412.
91.
ScorticatiMCRainaGMicheliF. Cluster-like headache associated to a foreign body in the maxillary sinus. Neurology2002; 59: 643–4.
MainardiFMaggioniFDaineseFPalestiniCZanchinG. Cluster-like headache due to warfarin therapy?. Cephalalgia2003; 23: 476–8.
94.
BigalMERapaportAMCamelM. Cluster headache as a manifestation of intracranial inflammatory myofibroblastic tumour: a case report with pathophysiological considerations. Cephalalgia2003; 23: 124–8.
95.
CevoliSMagnificoFPierangeliGMinguzziECortelliPMontagnaP. Cluster headache (CH) with aura associated with parieto-occipital arteriovenous malformation (AVM). Cephalalgia2003; 23: 669–70.
BrighinaLFrigerioRSantoroPMarinaRFerrareseCAgostoniE. Dissecting aneurysms of the extracranial internal carotid artery presenting with cluster-like headache: treatment with endovascular stent. Neurol Sci2003; 24(Suppl.): S131–S131
99.
Seijo-MartinezMCastro del RíoMCondeCBrasaJVilaO. Cluster-like headache: association with cervical syringomielia and Arnold–Chiari malformation. Cephalalgia2004; 24: 140–2.
100.
BarbantiPFabbriniGTruiniACruccuG. Symptomatic cluster headache following an ischaemic lesion of the trigemino-cervical complex. Cephalalgia2004; 24: 785–785.
101.
PatrunoGMRomoriniAAlbertiG. Clinical and radiological findings in a case of probable cluster-like syndrome. J Headache Pain2004; 5(Suppl. 1): S38–S38.
NegoroKKawaiMTadaYOgasawaraJIMisumiSMorimatsuM. A case of postprandial cluster-like headache with prolactinoma: dramatic response to cabergoline. Headache2005; 45: 604–14.
104.
MaggioniFDaineseFMainardiFLisottoCZanchinG. Cluster-like headache after surgical crystalline removal and intraocular lens implant: a case report. J Headache Pain2005; 6: 88–90.
105.
LaiSLChangYYLiuJSChenSS. Cluster-like headache from vertebral artery dissection: angiographic evidence of neurovascular activation. Cephalalgia2005; 25: 629–32.
RazviSWalkerLTeasdaleETyagiAMuirK. Cluster headache due to internal carotid artery dissection. J Neurol2006; 253: 661–3.
108.
GentileSFontanellaMLo GiudiceRRaineroIRubioEPinessiL. Resolution of cluster headache after closure of an anterior communicating artery aneurysm: the role of pericarotid sympathetic fibres. Clin Neurol Neurosurg2006; 108: 195–8.
109.
MassieRSirhanDAndermannF. Chronic cluster-like headache secondary to an epidermoid clival lesion. Can J Neurol Sci2006; 33: 421–2.
StraubeAFreilingerTRütherTPadovanC. Two cases of symptomatic cluster-like headache suggest the importance of sympathetic/parasympathetic balance. Cephalalgia2007; 27: 1069–73.
116.
RigamontiAIurlaroSReganatiPZilioliAAgostoniE. Cluster headache and internal carotid artery dissection: two cases and review of the literature. Headache2008; 48: 467–70.
117.
Eimil-OrtizMMaría-SalgadoFFontán-TiradoCGonzález-SantiagoRVillar-VillarEMartínE. Pseudo-cluster-like headache secondary to contralateral epidermoid cyst of the pontocerebellar angle. Headache2008; 48: 471–2.
118.
TobinJFlitmanS. Cluster-like headaches associated with internal carotid artery dissection responsive to verapamil. Headache2008; 48: 461–6.
119.
AltyJKempsterPRaghavS. Cluster-like headache secondary to trigeminal meningioma. Neurology2008; 70: 1938–1938.
120.
TestaLMittinoDTerazziEMulaMMonacoF. Cluster-like headache and idiopathic intracranial hypertension: a case report. J Headache Pain2008; 9: 181–3.
121.
HarleyJSAhmedF. Cluster-like headache heralding inflammatory orbital pseudotumour. Cephalalgia2008; 28: 401–2.
GiraudPJouanneauEBorson-ChazotFLanteri-MinetMChazotG. Cluster-like headache: literature review. J Headache Pain2002; 3: 71–9.
125.
ZanchinGMainardiFDaineseFMaggioniF. Epidemiologia e classificazione delle cefalee. In: GallaiVPiniLA (eds) Trattato delle cefalee. Torino: Centro Scientifico editore, 2002, p.17–33
126.
EkbomKSvenssonDATräffHWaldenlindE. Age at onset and sex ratio in cluster headache: observations over three decades. Cephalalgia2002; 22: 94–100.
127.
EkbomKWaldenlindE. Cluster headache in woman: evidence of hypofertility? Headaches in relation to menstruation and pregnancy. Cephalalgia1981; 1: 167–74.
128.
PeatfieldRCPettyRGClifford RoseF. Cluster headache in women. Cephalalgia1982; 2: 171–2.
129.
ManzoniGC. Gender ratio of cluster headache over the years: a possible role of changes in lifestyle. Cephalalgia1998; 18: 138–42.
130.
LisottoCPalmieriAMainardiFMucchiutMZanchinG. Age at onset and gender ratio in cluster headache: clinical observations over 12 years. J Headache Pain2007; 8(Suppl.): 29–30.
131.
RusselBRTrembathRC. Genetics of cluster headaches. In: OlesenJGoadsbyPJRamadanNMTfelt-HansenPWelchKMA (eds) The headaches, 3rd edn. Philadelphia: Lippincott Williams & Wilkins, 2006, p.747–50
132.
LinKHWangPJFuhJLLuSRChungCTTsouHKWangSJ. Cluster headache in the Taiwanese—a clinic-based study. Cephalalgia2004; 24: 631–8.
133.
FischeraMMarziniakMGralowIEversS. The incidence and prevalence of cluster headache: a meta-analysis of population-based studies. Cephalalgia2008; 28: 614–18.
134.
SwaabDFHofmanMALucassenPJPurbaJSRaadsheerFCVan de NesJA. Functional neuroanatomy and neuropathology of the human hypothalamus. Anat Embryol (Berl)1993; 187: 317–30.
135.
Van VlietJAEekersPJEHaanJFerrariMDfor the Dutch RUSSH Study Group. Evaluating the IHS criteria for cluster headache—a comparison between patients meeting all criteria and patients falling one criterion. Cephalalgia2006; 26: 241–5.
136.
FavierIvan VlietJARoonKIWitteveenRJWVerschuurenJJGMFerrariMD. Review of 31 cases. Arch Neurol2007; 64: 25–31.