
Abstract
Our aim was to compare the need for analgesics/drugs of abuse between headache patients—chronic and episodic headache sufferers—and addicts, by the Leeds Dependence Questionnaire (LDQ). This is a self-completion 10-item instrument to measure dependence upon a variety of substances. We administered the LDQ questionnaire to 122 chronic daily headache (CDH) sufferers who had been taking one dose of analgesic drug every day for at least 1 year; 71 subjects suffering from episodic headache (EH) using analgesics only occasionally; 115 consecutive drug addicts (DA) with a diagnosis of substance dependence. The mean LDQ total score was similar in the CDH (11.58 ± 6.35) and DA (10.37 ± 6.51) groups, and for both it was significantly higher than the score in the EH (5.61 ± 3.00) group (P < 0.001). The CDH group had the highest scores, and higher scores than the DA group (Z = −8.18, P < 0.001) in item 8, assessing the primacy of effect over the kind of analgesic used, and in item 10 (Z = −5.03, P < 0.001), asking if it is difficult to live without the analgesic; the DA group had the highest scores, and higher scores than the CDH group, in item 9 (Z = −5.07, P < 0.001) addressing the need for the continued administration of the drug to maintain well-being, and in item 3 (Z =−2.39, P < 0.05), exploring compulsion to start the use of the drug. The EH group had lower scores in all items (P < 0.05) except for item 9, where there was no difference from CDH group; the EH group had also lower scores (P < 0.001) than the DA group, except for item 8, where, instead, the score was higher than in the DA group (Z = −5.33, P < 0.001). A strong link develops between chronic headache patients and the analgesics they use. This sort of ‘dependence’ appears to be a consequence of headache, originating from the necessity for the analgesic to cope with everyday life.
Introduction
Headache sufferers commonly take analgesics (1) and obviously they use more analgesics when the headache worsens, becoming more and more frequent. Analgesic overuse is a predictive factor of chronic pain, more typical for chronic daily headache (CDH) than for other kinds of chronic pain, like neck or low back pain (2). CDH associated with medication overuse is a growing problem worldwide (3); it has been found that 5% of general population (4, 5) and up to 80% of patients seen in subspecialty clinics (6–8) are affected by this condition. These headaches, even if heterogeneous, share the characteristic that the more analgesics are taken, the more frequent headache becomes (9). The second edition of the International Headache Society (IHS) classification (2004) (10) now allows these conditions to be diagnosed more accurately than in the past, as ‘medication-overuse headache’ (MOH). Nevertheless, the relationship between headache sufferers and analgesics have not been extensively analysed. Using terms borrowed from drug addiction, this relationship is described as abuse and dependence (9, 11–13) even if the dosage involved is usually in the therapeutic range (14).
This condition is similar to ‘pseudo-addiction’, a term that indicates an iatrogenic syndrome characterized by abnormal behaviour in patients treated with strong opioids, which superficially mimics the behaviour observed in addicts. Pseudo-addiction is caused by undermedication and is cured with an effective treatment of pain (15, 16). However, in Europe headache patients do not take strong opioids, but usually only non-steroidal anti-inflammatory drugs (NSAIDs), alone or associated with codeine or caffeine, which are devoid of significant abuse liability (17). Furthermore, the use of combinations with barbiturates, which can induce dynamic and kinetic tolerance (18), of ergot alkaloids, which cause withdrawal headache (19), and of codeine, is decreasing, but the prevalence of chronic headaches associated with overuse of symptomatic drugs has not changed (20). Moreover, triptans, which are generally not much used by patients who should instead benefit from them (21), in animal models induce aversive effects (22). Even if their overuse is increasing (23), it seems to be limited to patients who have already overused other drugs (24).
While systematic methods have been proposed to differentiate the behaviour of patients with chronic non-malignant pain treated with opioids from true addiction (25, 26), there are no appropriate instruments to assess the relationship between CDH patients and their analgesics. If they were available they could be included in the clinical evaluation and they could provide information useful for the care of patients with MOH, care which is difficult and complex (27–29).
The Leeds Dependence Questionnaire (LDQ) is a self-administered questionnaire (30) which can measure dependence upon every substance, exploring systematically ICD-10 diagnostic criteria (31) for defining dependence.
The aim of our study was to analyse, by means of the LDQ questionnaire, the need for analgesics among chronic and episodic headache patients, and to compare such need with the addicts’ need for their abused drugs.
Patients and methods
Subjects
Three groups of subjects were recruited (Table 1).
Patients' characteristics
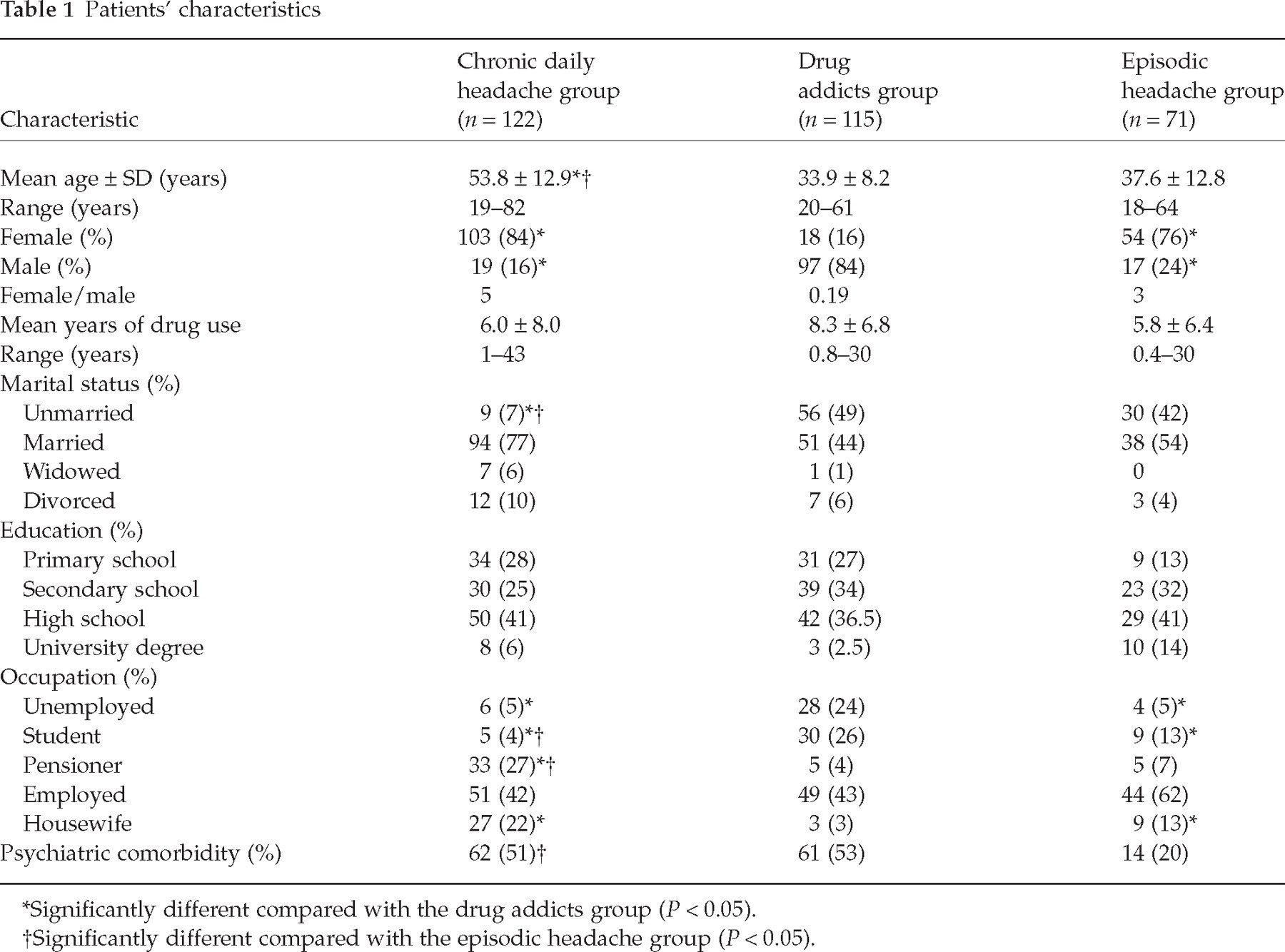
Significantly different compared with the drug addicts group (P < 0.05).
Significantly different compared with the episodic headache group (P < 0.05).
Chronic daily headache group
This group comprised 122 subjects who had been suffering from headache for at least 1 year, had been taking one or more analgesic daily over a period of at least 1 year, and had been consecutively admitted to the in-patients’ ward of the Headache Centre of the University of Modena and Reggio Emilia, to undergo withdrawal from their overused medications. At the outset the headache, according to the IHS criteria (1988) (32), was migraine with and/or without aura in 96 (79%) patients, and chronic tension-type headache in 26 (21%) patients. Self-reported favoured symptomatic medications were: NSAIDs, alone and/or in combination with caffeine, codeine, acethaminophen in 56 (46%) subjects; a combination of indomethacin, prochlorperazine and caffeine (IPC) in 28 (23%) subjects; triptans in 23 (19%) subjects; a combination of analgesics with butalbital in 12 (10%), and ergot alkaloids in three (2%) subjects.
Episodic headache group
This group consisted of 71 subjects who had been suffering from episodic headache (EH) and only occasionally used analgesics, consecutively visiting the out-patients’ ward of the Headache Centre for the first time, and referred by their general practitioner. Diagnosis, made according to the IHS criteria (1988) (32), was: migraine with and/or without aura in 55 (77%) subjects, episodic cluster headache, not in active phase, in nine (13%) subjects, and episodic tension-type headache in seven (10%) subjects. This group's favoured symptomatic medications were: NSAIDs, alone and/or in combination with caffeine, codeine, acetaminophen in 47 (66%); triptans in 17 (24%); and IPC in five (7%) subjects.
Drug addicts group
The drug addicts (DA) group consisted of 115 consecutive out-patients with diagnosis of substance dependence according to the criteria of the DSM-IV (33), attending the Town of Modena Drug Service Unit, for a rehabilitation programme comprising pharmacological and non-pharmacological interventions. Their favoured self-reported substances were: heroin in 62 (54%) subjects, cocaine in 24 (21%) subjects, alcohol in 14 (12%) subjects, cannabis derivatives in 12 (10%), and amphetamines in three (3%) subjects.
Questionnaire
The LDQ is a self-completion, 10-item, 0–3 scale according to the frequency (0 = never, 1 = sometimes, 2 = often, 3 = nearly always) instrument, designed to measure the severity of dependence upon a variety of substances, independently of the type or the quantity of substance used, and to be sensitive to change over time (30). It has been validated for use in alcohol and opiate consumers, in addiction and psychiatric settings (34). Test–retest reliability was found to be high (r = 0.95). The LDQ total score is expected to increase with the degree of substance dependence. No cut-off score indicative of dependence has been established (30). In order to have a questionnaire appropriate for our three groups, we made a slight variation in wording: the version for chronic and episodic headache patients referred to ‘analgesic/s’, whereas that for addicts referred to ‘drink or drug/s’.
Procedures
The LDQ questionnaire was administered to the subjects on their first arrival, respectively, at the Headache Centre for headache sufferers and at the Drug Service Unit for addicts, by two trained medical graduates. They explained the aim of the study and asked each person if they wished to participate; all subjects consented. Each subject was told that the questionnaire was being used only for research purposes. In answering the questions every subject was instructed to think about the last week, to think about their main analgesic/drink/drug (and to specify it), and to tick the response that was the most appropriate. Symptomatic headaches were excluded; none of the headache patients had either a prior history of drug and/ or alcohol abuse or a strong opioid analgesic assumption.
All patients’ diagnoses, psychiatric comorbidity and other characteristics were recorded by clinical documentation. Participants were enrolled between March 2002 and March 2003.
Data analysis
All data were checked by trained physicians and inserted in an apposite database. All statistical analyses were performed by SPSS 8.0 statistical software (SPSS Inc., Chicago, IL, USA). A complete descriptive analysis of the patients’ sampled parameters was carried out, as well as the Kolmogorov–Smirnov normality test. Since none of the parameters studied followed a normal distribution, comparisons between groups were made using the Kruskal–Wallis analysis of variance for non-parametric variables, followed by the Mann–Whitney U-test for independent samples. Percentages were compared by the χ2 test, followed by Fisher's exact test. P < 0.05 was chosen as significant for all the tests (35).
Results
The mean total LDQ score (Table 2) was similar between the CDH (11.58 ± 6.35) and DA groups (10.37 ± 6.51) and for both, significantly higher than for the EH group (5.61 ± 3.00) (P < 0.001). The pattern of responses of chronic headache patients differed from that of addicts in six out of 10 items. In particular, CDH patients had much higher scores than drug addicts in the items assessing the primary importance of the effect (item 8) (Z =−8.18, P < 0.001), the cognitive set (item 10) (Z =−5.03, P < 0.001), and the number of assumptions (item 6) (Z =−3.10, P < 0.005). The DA group had, instead, higher scores than the CDH group in item 3, assessing the compulsion to take drugs (Z =−2.39, P < 0.05), in item 7, investigating the compulsion to go on taking the drug (Z =−1.90, P = 0.05) and in item 9, concerning the need to maintain the effect (Z =−5.70, P < 0.001). The two groups showed no statistically significant differences in the mean scores of items 1, 4 and 5.
Leeds Dependence Questionnaire (LDQ) score (mean ± SD) for the three groups of patients

LDQ questionnaire given to the drug addicts group referred to ‘drink or drug/s’ instead of ‘analgesic/s’.
Chronic daily headache (CDH) vs. episodic headache (EH):
P < 0.05;
P ≤ 0.001. CDH vs. drug addicts (DA):
P ≤ 0.05;
P = 0.000. EH vs. DA: for all items and total score P < 0.001.
Differences between the DA and EH groups were statistically significant for all items (P < 0.05). In particular, the DA group had higher values in all items, except for item 8, which was, in contrast, much higher in he EH group (Z =−5.33, P < 0.001).
In the EH group the score for each item was lower than in the CDH group, except for item 9, whose score was not significantly different between the two groups.
Analysing the answers to each item of LDQ, the CDH group had the highest score in item 8, which explores the primary importance of the effect over the type of analgesic used. Item 10 had the second highest score. This item investigates the cognitive set, asking in particular if it is difficult to cope with life without an analgesic; item 9, assessing the necessity for constancy of a drug-induced state, had the lowest score. In the DA group, in contrast, this item had the highest score, followed by item 7, exploring the compulsion to go on taking the drug. In the EH group, item 8 had the highest score, as in the CDH group.
Discussion
The result of our study indicates that CDH patients had a very strong need for analgesics. The intensity of this need was similar to that of addicts for drugs of abuse: there were no significant differences in LDQ total score (Table 2) between the CDH (11.58 ± 6.53) and DA (10.37 ± 6.51) groups. This need was supported, first of all, by the necessity to relieve headache. In fact, in the CDH group, item 8 of the LDQ questionnaire, asking if achieving the effect is more important than the kind of drug, had the highest score. Patients suffering from chronic non-malignant pain, who were being treated with opioids, had the same opinion: answering a specific questionnaire, administered to investigate behavioural differences from ‘street’ heroin users, indicated the efficacy as a priority, independently of the type of drug, while all addicts stated a preference for one particular substance (26). Considering the slight importance attributed to the kind of drug by the CDH group, we can speculate that the analgesics more used by chronic headache patients are generally those which they find to be the most effective. This hypothesis is supported by the fact that the pharmaco-epidemiology of analgesic overuse varies in time and according to the pharmaceutical market, while its prevalence does not change (3, 20). To chronic headache patients studied, the analgesic was a sort of necessary crutch to cope with life in spite of daily pain. In fact, these patients gave item 10 of the LDQ questionnaire, asking if it is difficult to live without the drug, the second highest score. Examining only items 8 and 10, we find that the CDH group needed the analgesic even more than addicts needed the drug, since the DA group gave much lower scores for these two items (P < 0.001).
Even if the total score was similar in the two groups, the pattern of answers was, nevertheless, different. Addicts needed a constant effect of the drug much more than CDH patients in order to feel well and to avoid abstinence symptoms. In item 9, assessing this issue, the CDH group had the lowest score, while, in contrast, the DA group had the highest score (Z =−5.70, P < 0.001). In addition, the DA group had scores much higher than the CDH group in items assessing compulsive use, which represents dependence according to DSM-IV criteria. Also, the pseudo-addiction observed in patients with chronic non-malignant pain does not include the psychological dependence typical of addiction, even if these patients are treated with strong opioids, which induce tolerance and have reinforcing properties (15). Opioid pharmacology is considered dual, and different between pain patients and addicts. In chronic cancer pain the reason for increasing the dose of opioid is usually an increase in pain rather than the development of tolerance (36, 37).
Overuse, in the CDH patients we examined, concerns drugs which have a very little abuse liability. This term refers to the likelihood that a drug with psychoactive effects sustains patterns of non-medical self-administration that result in disruptive consequences (38). Our chronic headache patients, instead, use analgesics therapeutically, to relieve pain and maintain a normal life style. To sum up, even if many authors (9, 11–13) mention analgesic abuse and dependence, when chronic headache patients overuse analgesics it is in fact because of pain. In the addict, drug use controls the user's behaviour (39), while in the chronic headache patient it is pain which controls the user's behaviour (14).
EH patients used the analgesic in a very cautious way, since the LDQ total score was significantly lower than in the CDH and DA groups (P < 0.001). Many EH patients are stoical in face of pain and take the analgesic only when headache becomes unbearable (40). On the other hand, even EH patients established some involvement with their favourite analgesic. In fact, the total LDQ score of these patients (5.61 ± 3.00) was much higher than that reported in subjects with no substance use disorder (1.72 ± 3.62) (34). This result is also likely to depend on their headache, since the pattern of answers was similar to that of the CDH group, while all the scores were significantly lower (P < 0.001) than those of the DA group, except in item 8. Here, in contrast, the score was much higher than in the DA group. This item, assessing the primacy of effect over the kind of drug, therefore appears to be the hallmark of headache, either episodic or chronic (P < 0.001).
Our study has some limitations. As with all surveys of this type, reliance is placed upon respondents providing accurate information. Headache patients had no reason to answer incorrectly or with bias. With regard to addicts, validity of self-report is high when independent of consequences (41). However, addicts were assessed in a treatment environment, which reduces drug craving (42), while we recruited headache patients who definitely overused analgesics. Both these factors could have contributed to render the LDQ total score similar in the CDH and DA groups.
In conclusion, our results show that LDQ testing allows one to distinguish the need of the drug deriving from headache and drug addicts’ primary dependence. The hallmark of CDH patients who overuse analgesics was a much higher score than both the DA and EH groups in item 10, addressing the need of analgesics to cope with life.
The link between CDH patients and their analgesic is very strong. This ‘dependence’ does not derive from the addicting properties of the analgesics, but from their capacity to help patients to cope with life, in spite of daily headache. The LDQ questionnaire might prove to be a simple and quick method that should be included in clinical evaluation of headache patients, allowing the detection of subjects at risk of overuse or relapse and to measure progress in treatment.