
Abstract
Cluster headache (CH) is diagnosed according to criteria of the International Headache Society (IHS), but, in clinical practice, these criteria seem too restrictive. As part of a nation-wide study, we identified a group of patients who met all criteria minus one (IHS-CH-1), and assessed in which way they differed from CH patients meeting all criteria (IHS-CH). We performed a nation-wide questionnaire study for CH and CH-like syndromes, including questions based on the IHS criteria, and additional features such as restlessness during attacks, nocturnal onset of attacks, circadian rhythmicity of attacks and response to treatment. IHS-CH and IHS-CH-1 patients were compared. Of 1452 responders to two questionnaires, 1163 were IHS-CH and 289 were IHS-CH-1. The majority of the IHS-CH-1 patients were classified as such because their attacks exceeded 3 h (64%, median attack duration: 5 h), or came in a frequency of less than 1 per 2 days (16%). Age at onset was similar between the groups. The male to female ratio was 3.7 : 1 in the IHS-CH group and around 1.6 : 1 in the IHS-CH-1 groups (P < 0.005). Patients with attacks exceeding 3 h less often reported a circadian rhythmicity (IHS-CH-1: 49%, IHS-CH: 64%), episodic periodicity (IHS-CH-1: 65%, IHS-CH: 78%), nocturnal attacks (IHS-CH-1: 67%, IHS-CH: 78%), smoking (IHS-CH-1: 90%, IHS-CH: 80%) and restlessness during attacks (IHS-CH-1: 64%, IHS-CH: 76%) than IHS-CH patients (P < 0.005). Photo- or phono-phobia (IHS-CH-1: 67%, IHS-CH: 54%) and nausea (IHS-CH-1: 38%, IHS-CH: 27%) were more frequently reported by patients who reported to have attacks exceeding 3 h (P < 0.005). Similar proportions reported effect of verapamil on their attacks (IHS-CH-1: 54%, IHS-CH 61%). We conclude that average attack duration exceeding 3 h was frequently the reason for not fulfilling IHS CH criteria. Symptoms often accompanying CH such as restlessness, nocturnal attacks and an episodic attack pattern were relatively frequently present in IHS-CH-1 patients with longer attacks. These patients may therefore be diagnosed with CH. Attack frequency may not be a useful criterion for the diagnosis of CH. The upper limit of 3 h should be increased in future diagnostic criteria.
Introduction
Cluster headache (CH) is characterized by severe attacks of short duration, associated with one or more signs of autonomic dysfunction on the painful side. As diagnostic tests are not available, the diagnosis is made clinically, according to the criteria of the International Headache Society (IHS) (1). Such strict and recognizable criteria are important for scientific reasons, but, in clinical practice, they can prove to be too restrictive, as patients with syndromes resembling CH are likely to exist and probably will benefit from CH specific treatment.
As part of a nation-wide study among CH and CH-like patients, we identified a large group of patients that met the IHS criteria for CH minus one. The aim of this study was to describe this group of patients and compare them with patients who fulfilled all diagnostic criteria in order to investigate whether the present criteria of the IHS should be applied with more flexibility in clinical practice.
Methods
Subject recruitment
A nation-wide search for CH and CH–like syndromes was performed, using mailings to all Dutch Neurologists (c. 560) and general practitioners (GP's) (c. 5800). Patients could also apply via a CH web-site and the Dutch Society for Headache Patients. In the GP mailing, we included a card with the diagnostic criteria for CH. We specifically asked physicians to refer all patients with CH-like syndromes such as other trigeminal autonomic cephalagias (TAC's) (2, 3) and patients with a clinical picture resembling CH, but not completely fulfilling the criteria for CH.
After referral, patients were sent a questionnaire containing items concerning the IHS criteria for CH, but also including a variety of questions on additional clinical features (e.g. restlessness and nausea during attacks, nocturnal onset of attacks). Those who met all but one of the diagnostic criteria (IHS-CH-1 patients) were compared with patients who met all IHS criteria for CH (IHS-CH patients).
Statistical analysis
All data were entered into a database (MS Access) and analysed using SPSS software. Data are expressed as percentage, mean (SD) or median (range). χ2-test was used for comparisons between categorical data. Because of multiple comparison issues, a P-value of < 0.005 was considered as statistically significant.
Results
Nation-wide survey
Between May 1998 and March 2001 a total of 2001 subjects were recruited: 713 (36%) by neurologists (181 from our own out-patient clinic), 419 (21%) by GP's and 505 (25%) patients responded to an announcement in the magazine of the Dutch Migraine Patients Society. Two hundred and thirty-five (12%) responded via a web-site. The remaining CH patients were family members of patients with CH (n = 84) or were included via other media (n = 23). The reason for referral in a small group could not be elucidated (n = 22).
Of the 2001 patients, 1433 had IHS-CH and 396 had IHS-CH-1. The remaining 172 patients missed 2 or more IHS criteria and were excluded from this study.
After the first questionnaire, a second, more extensive questionnaire was mailed to all IHS-CH and IHS-CH-1 patients. Of the 1452 patients who filled in this extensive questionnaire, 1163 had IHS-CH and 289 had IHS-CH-1. The data of these patients are reported in this article.
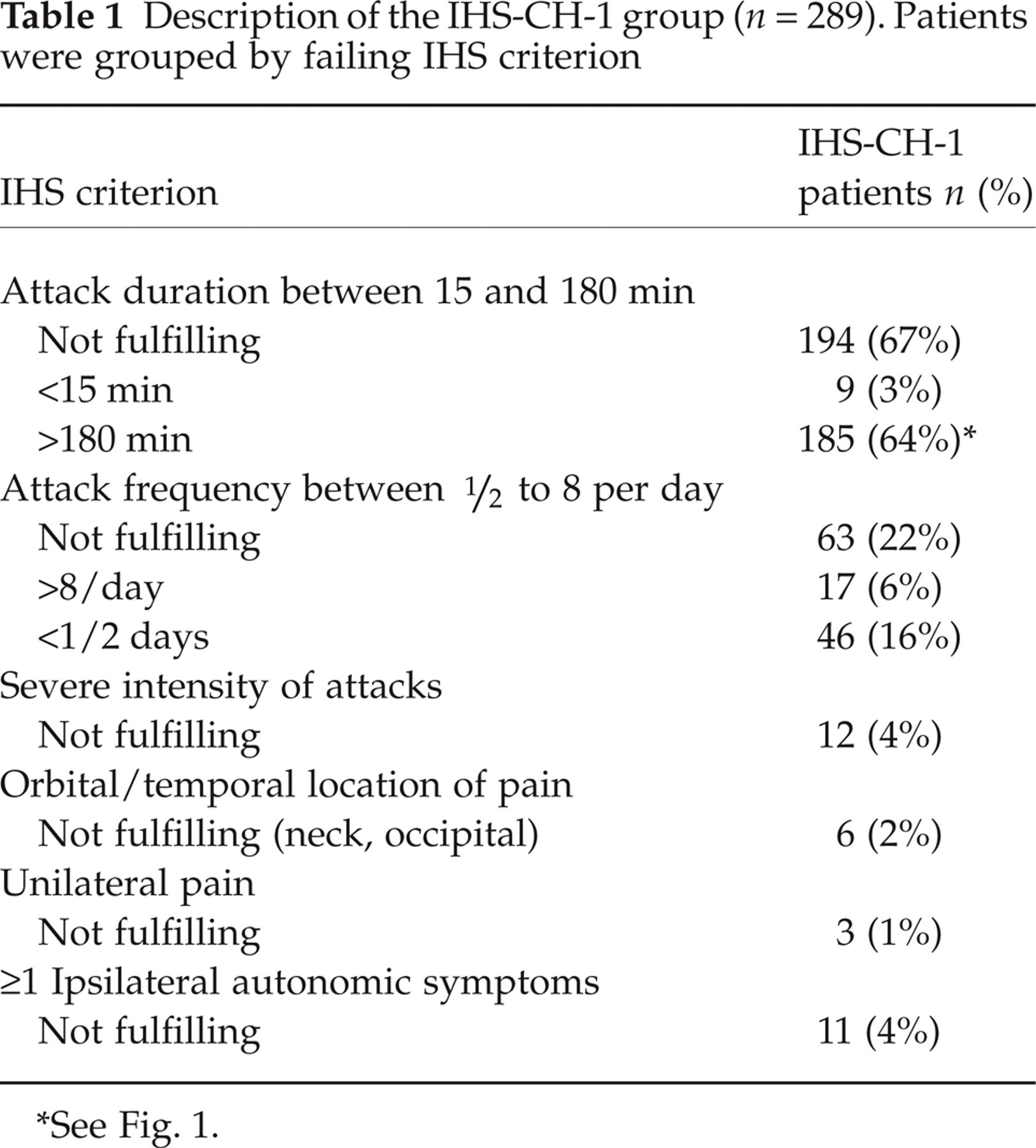
In the IHS-CH-1 group, the criteria for attack duration (n = 194, 67%) and attack frequency (n = 63, 22%) were most often failed, while there were only rarely other lacking criteria (Table 1). In the IHS-CH-1 patients with attack duration longer than 3 h (n = 185, 64%), attack duration ranged between 190 min to 5 days (median 5 h). Ninety patients reported attacks that lasted 6 h or longer (48 men and 42 women). Of these, 36 reported attacks that lasted longer than 24 h(12 men and 24 women) (Fig. 1).
Description of the IHS-CH-1 group (n = 289). Patients were grouped by failing IHS criterion
See Fig. 1.

Attack duration in the IHS-CH-1 patients who reported attacks succeeding 3 h (n = 187). □ females; ▪ males.
Forty-two percent of the IHS-CH-1 group with on average long attacks, reported that in occasional attacks the duration was shorter than 3 h. This means that, in general, these patients have long lasting attacks (the reason for classifying them as IHS-CH-1), but they also have attacks that do fulfil the IHS criteria. In the IHS-CH-1 group with a too low attack frequency (n = 46, 16%), the mean attack frequency was 2.0 per week (SD 1.0).
IHS-CH-1 patients who reported long attack duration were compared to IHS-CH patients on a variety of clinical characteristics (Table 2). Mean age at onset did not differ between the groups. The male to female ratio was lower in the IHS-CH-1 patients compared to IHS-CH patients (P < 0.001). Restlessness and nocturnal onset were less often present in the IHS-CH-1 group, as were a circadian rhythm of attacks and smoking (P < 0.001).
Comparison of clinical characteristics of IHS-CH and IHS-CH-1 patients with attacks exceeding 3 h

P≤ 0.005.
The standard CH treatments were tried in little more than half of all IHS-CH patients: oxygen was used by 51%, sumatriptan SC by 56% and verapamil by 50% (Table 3). IHS-CH-1 patients with longer attack duration were less frequently were tried on oxygen (P < 0.001). A combination of both acute (oxygen or sumatriptan SC) and prophylactic (verapamil or lithium) treatment was reported by 54% of the IHS-CH patients and 45% of the IHS-CH-1 patients (P = 0.03). Treatment with propranonol, ergotamine, sumatriptan tablets, carbamazepin and amitriptyline was reported in both groups.
Treatment for cluster headache in the IHS-CH-group (n = 1163) and IHS-CH-1 with longer attacks (n = 187) group

% based on patients who had tried this medication.
Discussion
In this population-based study we found a relatively large group of patients that failed one of the criteria for CH (IHS-CH-1), but further met all other criteria. An average attack duration exceeding 3 h was frequently (64%) the reason for not fulfilling the IHS CH criteria. Symptoms often accompanying CH such as restlessness, nocturnal attacks and an episodic attack pattern were relatively frequently present in IHS-CH-1 patients with longer attacks. These patients may therefore be diagnosed with CH. Attack frequency may not be a useful criterion for the diagnosis of CH and should be applied with some flexibility in clinical practice.
CH was first described in detail by Horton et al. (4, 5) and Kunkle (6), who noted that CH attacks usually lasted shorter than 30 min, but could last up to 7 h. As the time limit of three hours seems to be arbitrary, this criterion should be used more flexible in clinical practice and may be subject for discussion for revision of the diagnostic criteria. Dutch physicians did not seem to use the IHS criteria too strictly, as specific CH treatment(e.g. verapamil) was tried in IHS-CH-1 patients in 45%.
It is important to examine the patients carefully, as there may be a higher risk for an underlying cause when established criteria are not fully met. It is not very likely, however, that an underlying structural disease will change the duration of attacks, or the frequency. We did not investigate whether CH-1 patients are more prone to underlying causes, and therefore we can not state that CH-1 patients are more likely to have a secondary headache syndrome. This would be a valuable opportunity for future research.
The lower male to female ratio in the IHS-CH-1 group was remarkable, but no other important clinical differences between IHS-CH and IHS-CH-1 patients were found on a variety of characteristics (although differences were statistically significant due to the large numbers of patients).
In studies involving clinical data of primary headaches, data are usually collected retrospectively, as only rarely patients are seen during an attack. Patients may have both longer and shorter attacks, and therefore some attacks may fulfil the criteria for CH, while other attacks may not. We found that 42% of the patients, who on average had long attacks, reported that some of their attacks were shorter than 3 h. As patients most likely remember their most severe attacks, overestimation of attack duration may occur. A prospective study could provide more definite answers in this matter.
The second largest group included patients with a lower attack frequency (mean: 2 attacks per week) who were therefore diagnosed with IHS-CH-1. However, as the individual attacks meet the current criteria for CH, it may be favourable to diagnose these patients with CH by using the criteria for attack frequency not too strictly.
Typical CH features such as restlessness during attacks and an episodic attack pattern were relatively frequently found in the IHS-CH-1 group, stressing our suggestion that IHS-CH-1 patients have a form of CH, and may benefit from CH treatment. This spectrum hypothesis is further supported by the finding that 42% of the IHS-CH-1 patients with long attacks occasionally had attacks that fulfil the IHS-CH criteria. Nausea and photophobia have increasingly been recognized in CH attacks (7, 8), and were frequently found in both patient groups in our study. According to the IHS criteria, the presence of these symptoms does not exclude CH, but in clinical practice it may cause confusion with migraine.
Footnotes
Acknowledgements
JA van Vliet is supported by the Asclepiade foundation. The Dutch RUSSH (Rare and Unusual Severe and Short-lasting Headaches) group consists (in addition to the authors) of: JWM ter Berg (Sittard), FEAM Bussemaker (Hoorn), EGM Couturier (Amsterdam), D Herderschee (Hilversum), JBM 10 Holter (Deventer), A Knuistingh Neven (Krimpen a/d IJssel), PJ Koehler (Heerlen), JH Kok (Den Helder), JBM Kuks (Groningen), JAM Kuster (Haarlem), LJJM Mulder (Rotterdam), E Siebenga (Gouda), TJ Tacke (Hengelo). The authors would like to thank L. van Berkel, H. van Dongen, F. van Dijk, J. Tjon, R. Rampaart, M. Swinkels, C. Leenaars and A. Douma for their help in data-entry.